
Abstract
Background:
Ankle fractures occur at an estimated rate of 4.22 per 10 000 person-years, occurring most frequently within the 21- to 30-year-old demographic. This retrospective cohort study used the TriNetX research network to evaluate the association between perioperative glucagon-like peptide-1 receptor agonist (GLP-1RA) use and postoperative complications following operative ankle fixation.
Methods:
Adults were stratified by GLP-1RA exposure (n = 1199 for the 3-month cohort and n = 1397 for both the 6- and 12-month cohorts). These cohorts were balanced via 1:1 propensity score matching for age, race, sex, wound healing risk factors, and diabetes; matching was attempted for body mass index (BMI) and glycated hemoglobin (HbA1c) but was not obtained. The 6 complications were assessed from 1 day to 3 months, 6 months, and 1 year postoperatively.
Results:
Results demonstrated that GLP-1RA therapy was significantly associated with increased risk of hardware failure, beginning at 3 months (log rank test [LRT] χ2 = 3.838, P = .050) and persisting through 12 months (LRT χ2 = 5.527, P = .019; risk difference [RD] = 0.017, P = .018). Nonunion/malunion rates in the GLP-1RA cohort were more common, with significance found at 6 months (RD = 0.010, P = .047) and 12 months postoperatively (RD = 0.014, P = .008). No association was observed with postoperative infection across any time point. Furthermore, a neutral significance was established for wound dehiscence and procedural complications. Although test statistics suggested potential variance, primary longitudinal measures did not demonstrate significant divergence between cohorts (12-month LRT P = .131 and P = .482, respectively).
Conclusion:
These findings suggest that perioperative GLP-1RA use is associated with increased rates of hardware failure and nonunion/malunion, identifying a risk profile localized to osseous integrity. No association was found with postoperative infection, and a neutral significance was established for soft tissue complications. Interpreted in the context of residual imbalance in BMI and HbA1c, these findings are hypothesis-generating rather than confirmatory.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Ankle fractures remain one of the most common fractures treated in orthopaedic practice, with an estimated incidence of 4.22/10 000 person-years, with young adults aged 21-30 years having the highest injury rates.1,2 These injuries represent a substantial source of health care utilization and morbidity, particularly among patients with metabolic conditions like obesity and type 2 diabetes. 3 These are both known factors that can increase fracture risk and reduce bone quality and effective lower-limb biomechanics, further contributing to the associated risk.4-6
With obesity impacting up to 40% of American adults, and 38 million people with type 2 diabetes, glucagon-like peptide 1 receptor agonists (GLP-1RAs), initially indicated for glycemic control, are now being widely prescribed as a cornerstone therapy for weight management.7,8 Widely prescribed agents such as semaglutide, retatrutide, and tirzepatide produce substantial metabolic changes that contribute to weight reduction, which has led to widespread adoption. 9
Preclinical and clinical studies suggest that GLP-1RAs may influence bone metabolism by promoting formation, inhibiting resorption, and potentially improving bone quality; however, the overall impact of GLP-1 receptor agonists on fracture risk remains uncertain and may be influenced by weight loss. 10 There are also competing studies that suggest potentially adverse associations with fracture risk, whereas other studies suggest that there is no change in the risk of fracture with those patients taking GLP-1RA medications.11,12 These changes may also be impacted by alterations in biomechanical loading across the ankle joint and alter gait biomechanics, potentially influencing injury patterns.
Given the rapid adoption of GLP-1RAs and the orthopaedic burden of ankle fractures, there is a need to better understand potential associations between GLP-1RA use and ankle fracture postoperative complications on a population level. The objective of this study is to evaluate the association between perioperative GLP-1RA use and postoperative complications following operative ankle fracture fixation using a retrospective cohort analysis of a federated EHR database.
Methods
Data Source and Study Design
We conducted a retrospective cohort study using TriNetX, a federated electronic health record (EHR) research network that supports analysis of deidentified patient data across participating health care organizations. 13 The TriNetX Analytics platform contains structured information on demographics, diagnoses, procedures, medications, and laboratory values and provides built-in tools for cohort construction, propensity score matching, and outcome analyses (Supplemental Table S4). All analyses were performed on March 13, 2026, using the historical data available in TriNetX at that time. As a dynamic, federated system, these results are a snapshot and subject to change as member institutions update their records. Furthermore, platform-level constraints may exclude certain index events that fall outside allowable historical windows.
We identified adults ≥18 years of age who underwent operative management of ankle fracture–related pathology using a basket of ankle surgery procedure codes. The index event for each patient was the most recent instance of an included ankle surgery procedure. The ankle surgery basket includes Current Procedural Terminology (CPT)-based operative fixation and related ankle procedures, as well as International Classification of Diseases, Tenth Revision–Procedure Coding System (ICD-10-PCS) ankle joint reposition with internal fixation. The full code list used to define the ankle surgery index event is provided in Supplemental Table S1. Through this system, 2 cohorts were defined as detailed below.
(1) GLP-1 exposure cohort (ankle surgery on GLP-1): Patients were included if they had evidence of GLP-1 therapy within 6 months on or before the most recent ankle surgery event. GLP-1 therapy was defined using a medication concept set that included ATC A10BJ (GLP-1 analogues) and individual GLP-1 agents mapped within TriNetX (semaglutide, liraglutide, dulaglutide, exenatide, lixisenatide, albiglutide; see Supplemental Table S1).
(2) No GLP-1 cohort (never-use comparator): Patients meeting the same ankle surgery index definition were assigned to the comparator cohort if they had no recorded GLP-1 therapy at any time in their available TriNetX medication history (ie, the GLP-1 medication concept set was included as an exclusion criterion).
This cohort design is visually shown in Figure 1.
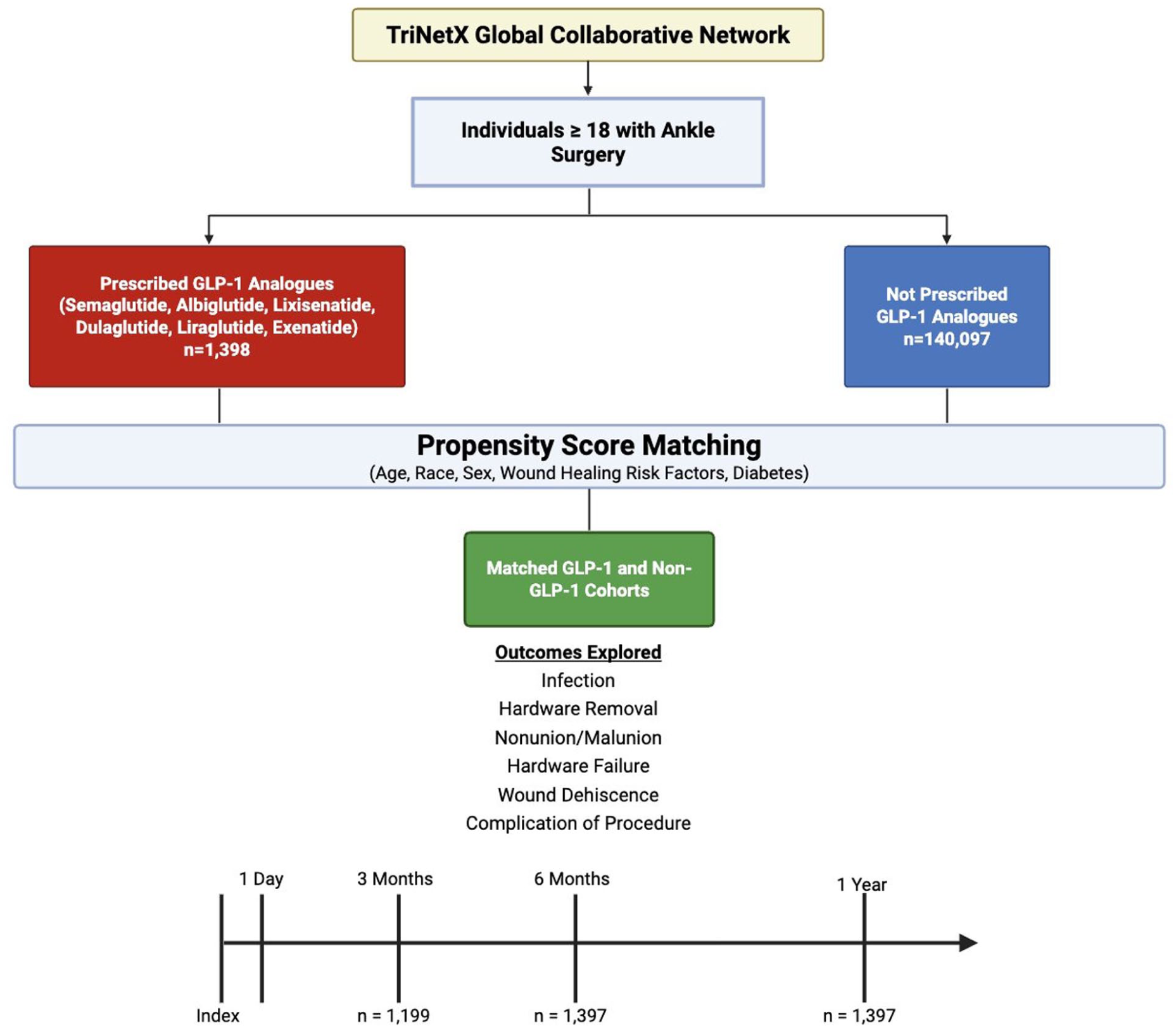
Study design and patient selection flowchart. (Patients aged ≥18 years undergoing ankle surgery were identified from the TriNetX Global Collaborative Network and divided into GLP-1 analogue (n = 1398) and non-GLP-1 (n = 140 097) cohorts. Propensity score matching was performed on age, race, sex, wound healing risk factors, and diabetes. Six postoperative complications were assessed from 1 day to 3 months, 6 months, and 1 year.).
Baseline Characteristics, Outcomes, and Propensity Score Matching
As this study is exploratory with no prespecified primary outcome, to address confounding, we selected baseline characteristics based on their clinical relevance to fracture healing, postoperative risk, and infection/complication susceptibility. These variables were saved within TriNetX and used for propensity score matching. Covariates included age, sex, and race/ethnicity. Comorbidities included diabetes mellitus, chronic kidney disease, chronic ischemic heart disease, heart failure, and chronic obstructive pulmonary disease. Tobacco exposure was captured through nicotine dependence, active tobacco use, and personal history of nicotine dependence (Supplemental Table S2). This set was chosen to balance key metabolic and cardiopulmonary risk factors, renal disease burden, and tobacco-related impairment of wound and bone healing, while avoiding an exhaustive list that could limit matching. Continuous variables BMI and hemoglobin A1c were originally included in the matching algorithm; however, adequate balance was not achieved for either variable. This is further discussed below.
Outcomes were assessed at 3 months, 6 months, and 1 year after the index ankle surgery to reflect clinically meaningful stages of postoperative recovery and fracture healing. Six outcomes were defined using diagnosis and procedure code groupings (Supplemental Table S3): a composite infection-related outcome, hardware removal, nonunion/malunion, hardware failure/mechanical complication, wound dehiscence, and a broad complications-of-procedures category. It is important to note that nonunion/malunion was captured using ICD-10 Clinical Modification (ICD-10-CM) code M84 as a union-complication proxy, given coding heterogeneity across health care organizations. For each follow-up window, patients with documented evidence of the outcome before the start of the window were excluded from that specific outcome analysis to isolate postoperative event incidence. Time-to-event analyses, Kaplan-Meier, were also performed using TriNetX for applicable outcomes. No minimum follow-up requirement was applied.
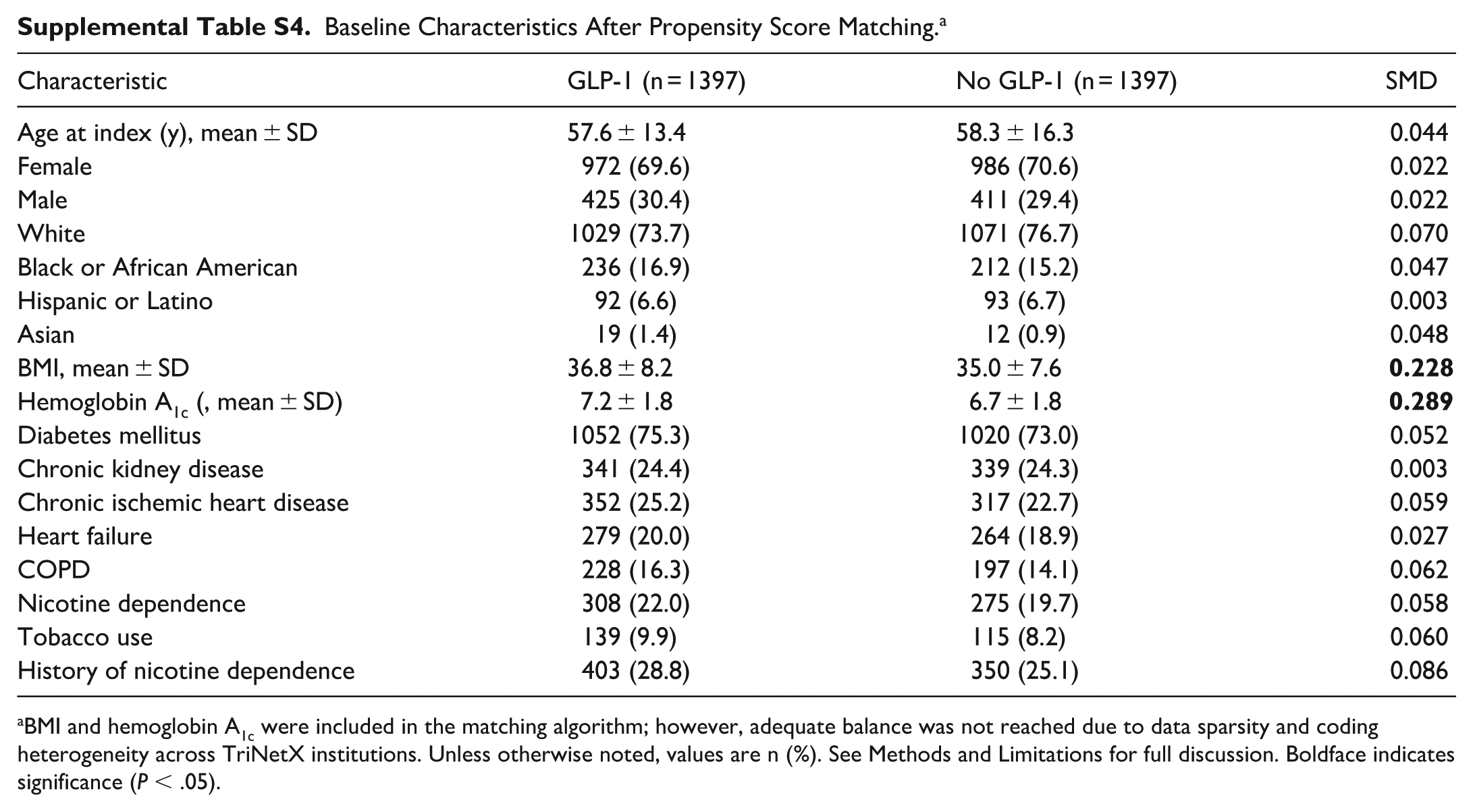
Propensity score matching was performed within TriNetX using 1:1 matching between the GLP-1 exposure cohort and the never-use comparator cohort based on the covariates listed above. Cohort balance after matching was evaluated using TriNetX-provided standardized mean difference (SMD) diagnostics, with an SMD ≤ 0.10 used as the generally acceptable threshold for proper balance. Covariate balance improved substantially after matching; however, BMI (SMD = 0.228) and HbA1c (SMD = 0.289) demonstrated residual imbalance exceeding this threshold in the matched cohorts (Supplemental Table S4). Several platform-level constraints inherent to TriNetX contribute to this limitation. First, both variables are summarized using only patients with a recorded value, reflecting the fact that various electronic health record platforms handle data capture differently, and many do not have this information readily available for analysis in their systems. Consequently, the subset with available measurements may differ systematically between cohorts. Second, both BMI and HbA1c were captured using the platform’s default most recent recorded value rather than a strictly pre-index measurement, introducing variability in measurement timing and clinical context across contributing health care sites. Third, because GLP-1 receptor agonists are prescribed preferentially in patients with more advanced metabolic disease, complete distributional overlap in BMI and glycemic control between GLP-1-exposed patients and a never-use comparator population is inherently constrained, independent of matching algorithm performance. Overweight and obesity status was explicitly included as a categorical matching covariate alongside continuous BMI, which may mitigate the impact of residual imbalance in the continuous BMI variable. It is important to note that TriNetX does not permit post hoc modification of matching parameters or iterative caliper refinement once an analysis has been executed. Nevertheless, readers should consider the potential for residual confounding by metabolic disease severity when interpreting the outcome associations reported herein, as discussed further in Limitations.
Statistical Analysis
All analyses were performed within the TriNetX Analytics environment. Outcomes were compared between matched cohorts at each specified time point using TriNetX’s risk analysis outputs. Kaplan-Meier methods were used for time-to-event comparisons. Baseline cohort characteristics were compared using TriNetX’s built-in statistical tests, which apply t tests for continuous variables and z tests or χ² tests for categorical variables. Statistical significance was assessed using a 2-sided alpha threshold of .05.
Results
Statistical significance for postoperative outcomes was evaluated through the log-rank test (LRT), hazard ratio (HR), risk difference (RD), and test statistic (TS). The LRT served as the primary longitudinal measure to assess differences in cohort survival curves over the study period. The HR was used to quantify the instantaneous relative risk and identify early signals of increased hazard within specific intervals. The RD measured the absolute difference in the proportion of events at specific time points to determine cumulative clinical impact. The TS provided the mathematical basis for P value derivation across all analyzed metrics.
Study Population and Analysis
The study used a retrospective cohort design to identify patients who underwent major ankle procedures and stratified them by perioperative GLP-1 receptor agonist exposure. To ensure internal validity, 1:1 propensity score matching was performed across 3 distinct follow-up intervals. Covariate balance was achieved across the majority of variables; however, 2 covariates demonstrated residual imbalance exceeding the conventional SMD ≤0.10 threshold: BMI (GLP-1 group 36.8 ± 8.2 vs No-GLP-1 group 35.0 ± 7.6, SMD = 0.228) and HbA1c (7.2% ± 1.8% vs 6.7% ± 1.8%, SMD = 0.289) (Supplemental Table S4). Both variables are mechanistically relevant to the outcomes reported in this study and represent a constraint on causal interpretation, as discussed further in Limitations. The first was the 3-month cohort, which included 1199 patients per group because of limited reporting. For the 6-month and 12-month cohorts, the study population was successfully expanded and matched to 1397 patients per group. The following tables include all RD, LRT, HR, and TS P values for each cohort. Nonunion/Malunion is absent for the 3-month cohort because of the smaller cohort size. All bolded values were found to be significant (P < .05).
Hardware Failure
Hardware failure emerged as the most consistent and statistically significant adverse outcome associated with GLP-1 therapy, demonstrating a clear increase in significance over the 12-month study period. An early signal of increased hardware failure was detected in the 3-month cohort, with the LRT reaching statistical significance (P = .050) with a χ2 value of 3.838 on 1 degree of freedom (Table 1). This early divergence occurred despite the smaller cohort size (n = 1199), suggesting a potent immediate postoperative risk. By 6 months, the HR of 1.536, with a 95% CI of 0.988 to 2.391 confirmed a statistically significant increased relative risk of failure for GLP-1 users (P = .023) (Table 2). At the conclusion of the study during the 12-month mark, hardware failure was identified as a consistent finding across multiple metrics, including the LRT χ2 of 5.527 (P = .019) and absolute RD of 0.017 with a 95% CI of 0.003 to 0.031 and a P value of .018 (Table 3).
Statistical Analysis of Postoperative Outcomes for the 3-Month Cohort. a
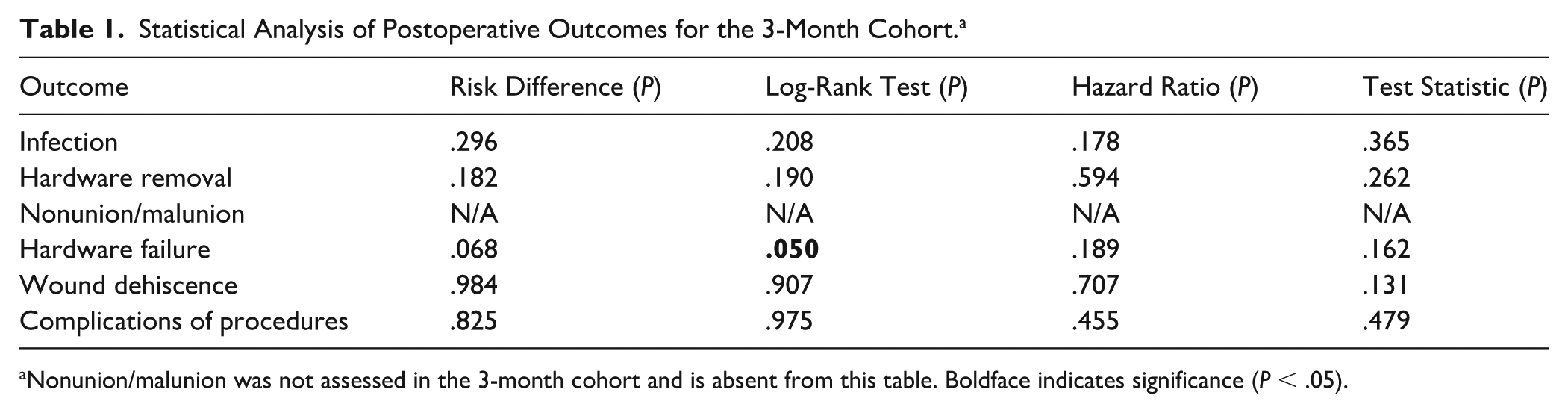
Nonunion/malunion was not assessed in the 3-month cohort and is absent from this table. Boldface indicates significance (P < .05).
Statistical Analysis of Postoperative Outcomes for the 6-Month Cohort. a
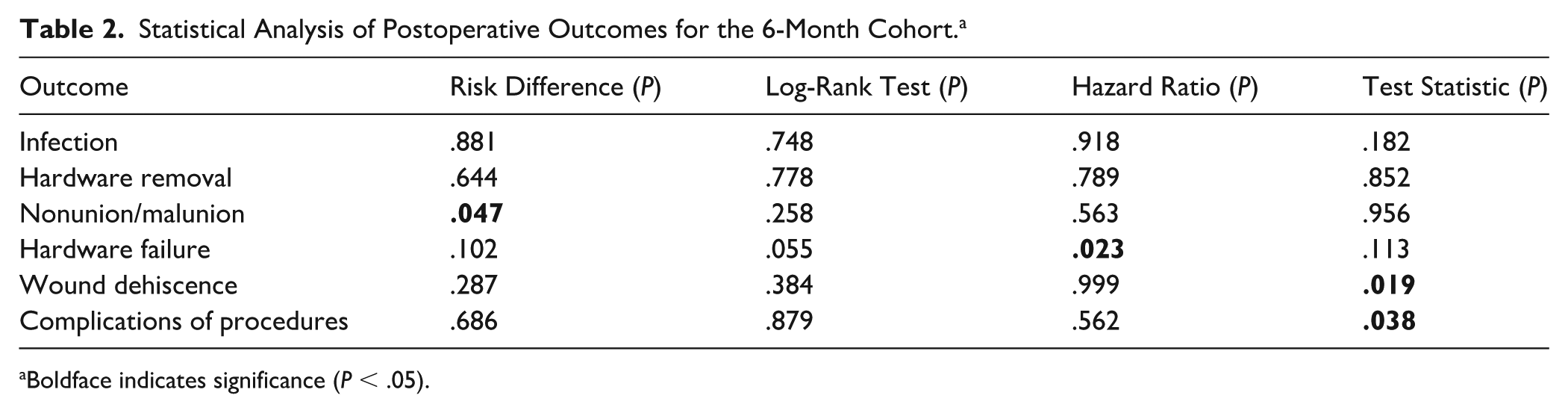
Boldface indicates significance (P < .05).
Statistical Analysis of Postoperative Outcomes for the 12-Month Cohort. a

Boldface indicates significance (P < .05).
Nonunion and Malunion
Bone-healing outcomes showed a temporal divergence between cohorts, with significant increases in nonunion and malunion only becoming statistically detectable during the 6- to 12-month follow-up period. Although the overall survival curve did not yet reach significance at 6 months (LRT P = .258), a significant RD (P = .047) of 0.010 and a 95% CI of 0.000 to 0.019 in the proportion of patients with nonunion was observed (Table 2). At 12 months, the GLP-1 cohort demonstrated a highly significant increase in the RD of 0.014 with a 95% CI of 0.004 to 0.024 in nonunion/malunion compared with the control group (P = .008) (Table 3).
Infection and Wound Care
Despite the increased failures with hardware and non/malunion, GLP-1 receptor agonists demonstrated a neutral impact on biologic infection and soft tissue integrity. There were no statistically significant differences in infection rates at any time point, with the 12-month LRT showing no significant deviation between the 2 cohorts (P = .864) (Table 3).
Rates of wound dehiscence and general complications of the procedure remained statistically comparable across both cohorts when evaluated by LRT and RD. Although the TS suggested potential divergences for wound dehiscence (P = .019 at 6 months; P = .029 at 12 months) and procedural complications (P = .038 and t = 2.382 at 6 months; P = .028 and t = 2.093 at 12 months), these findings did not reach statistical significance via LRT or RD (Tables 2 and 3). Specifically, the 12-month LRT and RD confirmed a lack of significance for both wound dehiscence (LRT P = .131 and RD P = .074) and procedural complications (LRT P = .482 and RD P = .281) (Table 3). Consequently, the data identifies a neutral correlation between GLP-1RA exposure and these safety outcomes.
Discussion
The results of this retrospective cohort analysis identify a statistically significant association between perioperative GLP-1RA use and an increased risk of hardware failure and nonunion/malunion following ankle surgery. These correlations were sustained throughout the 12-month study period, whereas no significant association was found between GLP-1RA use and soft tissue complications such as surgical site infection or wound dehiscence.
A longitudinal correlation was observed between GLP-1RA use and hardware failure, beginning in the early postoperative phase. An initial signal was detected at 3 months (LRT χ2 = 3.838, P = .050) and reached definitive significance by 6 months, where the hazard of failure was significantly higher in the GLP-1RA cohort (HR = 1.536; P = .023) (Tables 1 and 2). This correlation persisted through the 12-month follow-up, as evidenced by both the longitudinal survival analysis (LRT χ2 = 5.527, P = .019) and the absolute risk difference (RD = 0.017, P = .018) (Table 3). In contrast, other investigations have reported differing early trends; Morningstar et al 14 observed that at 30 days, patients in the non-GLP-1RA cohort exhibited significantly higher rates of hardware removal (OR = 1.953, 95% CI = 1.062-3.591, P = .028) compared with the GLP-1RA cohort.
The correlation between GLP-1RA use and impaired bone healing demonstrated a temporal divergence, with statistical significance emerging in the latter half of the study year. Although early data at 3 months did not reach significance, a significant absolute difference in nonunion rates was detected at 6 months (RD = 0.010, P = .047) (Tables 1 and 2). By 12 months, this association strengthened significantly (RD = 0.014, P = .008), identifying a strong correlation between the use of this medication class and a higher incidence of nonunion or malunion (Table 3). Although our findings suggest a long-term risk to osseous consolidation, Morningstar et al 14 found no statistically significant differences in risk for any complication at the 1-year and 5-year marks.
In contrast to the mechanical and biological healing complications, GLP-1RA use demonstrated a neutral correlation with traditional postoperative safety metrics. There was no statistically significant difference in rates of infection (LRT P = .864) or wound dehiscence (LRT P = .131) at the 12-month mark (Table 3). These findings suggest that the risks associated with GLP-1RA therapy in this population are limited to hardware integrity and osseous consolidation, rather than generalized surgical site complications. Additionally, when analyzing long-term outcomes such as post-traumatic arthritis, there appears to be no statistically significant difference in development within 5 years of surgery (OR = 1.313; 95% CI = 0.895-1.927) or at any point post index surgery (OR = 1.323; 95% CI = 0.909-1.925) based on GLP-1RA usage according to Morningstar et al 14
The associations observed between GLP-1RA use and hardware failure and nonunion/malunion must be interpreted in the context of residual covariate imbalance identified in the post-matching analysis. Both variables are independently associated with impaired osseous consolidation and mechanical fixation failure and represent the most mechanistically proximate confounders for the outcomes reported. It is therefore possible that the elevated complication rates observed in the GLP-1RA cohort reflect, at least in part, more advanced underlying metabolic disease burden rather than a direct pharmacologic effect of GLP-1 receptor agonism. These findings should not be interpreted as confirmatory evidence of causality and are best understood as hypothesis-generating, warranting prospective investigation with granular metabolic phenotyping to better disentangle drug exposure from disease severity.
Limitations
As a retrospective analysis of the TriNetX database, this study identifies statistical associations consistent with observational administrative data; these findings should be interpreted as hypothesis-generating rather than establishing a definitive causal link between GLP-1RA use and surgical failure. The reliance on administrative diagnosis and procedure codes for outcomes, specifically hardware failure and nonunion/malunion, serves as a primary limitation. These codes cannot necessarily confirm specific clinical or radiographic findings and may reflect documentation heterogeneity across the various institutions within the network.
A foundational limitation regarding medication exposure is that identified prescription records in the 6 months preceding surgery do not confirm patient adherence to the documented GLP-1RA therapy. Furthermore, the specific dose, patient adherence, and the precise temporal relationship between active drug exposure and the surgical event remain unknown and cannot be verified through administrative records. The initial 3-month analysis was limited by a smaller cohort size (n = 1199) compared with the 6- and 12-month analyses (n = 1397), which may have influenced the power of early-stage findings. Although propensity score matching was used to control for known comorbidities and demographics, adequate balance was not achieved for all covariates. Specifically, BMI (SMD = 0.228) and HbA1c (SMD = 0.289) remained above the conventional SMD ≤0.10 threshold, indicating residual imbalance in 2 variables that are directly associated with impaired fracture healing, nonunion, and hardware failure. Matching was achieved using categorical ICD-10 diagnostic codes for obesity and diabetes mellitus rather than continuous BMI and HbA1c values, which loses the gradient of information captured via continuous measurement. The inability to achieve adequate balance on these continuous variables reflects platform-level constraints of data sparsity and cross-institutional coding heterogeneity in the recording of BMI and HbA1c values. The GLP-1RA cohort had meaningfully higher BMI and worse glycemic control than the matched comparator group, and the current analysis cannot fully disentangle the independent contributions of metabolic disease severity from GLP-1RA exposure on the reported outcomes. This residual confounding represents a substantive limitation on causal interpretation, and these findings should be considered hypothesis-generating rather than confirmatory.
Conclusion
This retrospective cohort analysis identifies a statistically significant association between GLP-1RA use and increased rates of hardware failure and nonunion/malunion following ankle surgery; however, these findings must be interpreted with caution, given residual imbalance in BMI (SMD = 0.228) and HbA1c (SMD = 0.289) in the matched cohorts. As both variables are independently associated with impaired fracture healing and hardware integrity, the possibility that observed outcome differences reflect underlying metabolic disease severity rather than a direct effect of GLP-1RA therapy cannot be excluded, and these results are considered hypothesis-generating rather than confirmatory. Furthermore, a neutral significance was established for wound dehiscence and procedural complications. Although isolated test statistics suggested potential variances, the primary longitudinal and absolute measures did not demonstrate significant divergence. These findings suggest that the risk profile is localized to mechanical fixation and osseous integrity rather than generalized soft tissue complications. Given the hypothesis-generating nature of these results, surgeons should maintain heightened postoperative surveillance for hardware-related issues in this cohort. Future prospective studies are needed to establish causality, verify patient adherence and dosing, and guide evidence-based management protocols for patients on GLP-1RA therapy.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261453350 – Supplemental material for Association Between GLP-1RAs and Postoperative Complications Following Operative Ankle Fracture Fixation: A Retrospective Cohort Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114261453350 for Association Between GLP-1RAs and Postoperative Complications Following Operative Ankle Fracture Fixation: A Retrospective Cohort Study by Shawn K. Monteiro, Nabeel A. Khatri, Deen B. Sari and Christopher Sanford in Foot & Ankle Orthopaedics
Footnotes
Appendix
Baseline Characteristics After Propensity Score Matching. a
| Characteristic | GLP-1 (n = 1397) | No GLP-1 (n = 1397) | SMD |
|---|---|---|---|
| Age at index (y), mean ± SD | 57.6 ± 13.4 | 58.3 ± 16.3 | 0.044 |
| Female | 972 (69.6) | 986 (70.6) | 0.022 |
| Male | 425 (30.4) | 411 (29.4) | 0.022 |
| White | 1029 (73.7) | 1071 (76.7) | 0.070 |
| Black or African American | 236 (16.9) | 212 (15.2) | 0.047 |
| Hispanic or Latino | 92 (6.6) | 93 (6.7) | 0.003 |
| Asian | 19 (1.4) | 12 (0.9) | 0.048 |
| BMI, mean ± SD | 36.8 ± 8.2 | 35.0 ± 7.6 |
|
| Hemoglobin A1c (, mean ± SD) | 7.2 ± 1.8 | 6.7 ± 1.8 |
|
| Diabetes mellitus | 1052 (75.3) | 1020 (73.0) | 0.052 |
| Chronic kidney disease | 341 (24.4) | 339 (24.3) | 0.003 |
| Chronic ischemic heart disease | 352 (25.2) | 317 (22.7) | 0.059 |
| Heart failure | 279 (20.0) | 264 (18.9) | 0.027 |
| COPD | 228 (16.3) | 197 (14.1) | 0.062 |
| Nicotine dependence | 308 (22.0) | 275 (19.7) | 0.058 |
| Tobacco use | 139 (9.9) | 115 (8.2) | 0.060 |
| History of nicotine dependence | 403 (28.8) | 350 (25.1) | 0.086 |
BMI and hemoglobin A1c were included in the matching algorithm; however, adequate balance was not reached due to data sparsity and coding heterogeneity across TriNetX institutions. Unless otherwise noted, values are n (%). See Methods and Limitations for full discussion. Boldface indicates significance (P < .05).
Ethical Considerations
This study was a retrospective cohort analysis using deidentified data and did not require institutional review board approval.
Consent to Participate
This study was a retrospective cohort analysis using deidentified data and did not require informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.