
Abstract
Background:
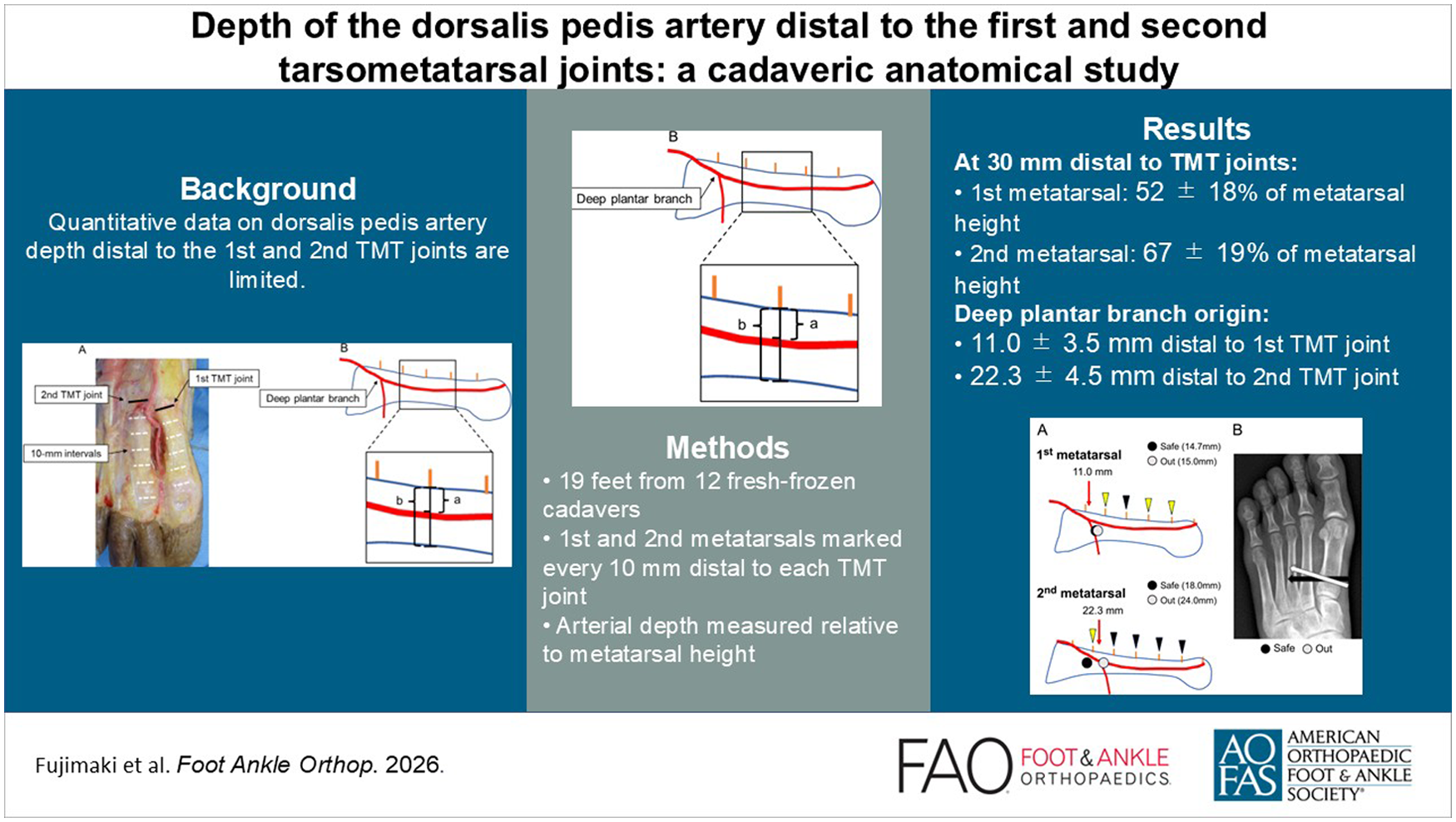
Surgical procedures involving the region between the first and second metatarsals distal to the tarsometatarsal (TMT) joints are common. However, detailed quantitative information regarding the depth of this arterial axis, encompassing the dorsalis pedis artery proximal to the branching point and the first dorsal metatarsal artery distally, remains limited. This study aimed to characterize the depth of the dorsalis pedis artery distal to the first and second TMT joints.
Methods:
Nineteen feet from 12 cadavers were analyzed. The first and second metatarsals were marked at 10-mm intervals distal to each TMT joint. The arterial depth at each point was expressed as a percentage of total metatarsal height, measured from the dorsal cortical surface (0%) toward the plantar cortex.
Results:
The deep plantar branch originated 11.0 ± 3.5 mm distal to the first TMT joint and 22.3 ± 4.5 mm distal to the second TMT joint. At 30 mm distal to the TMT joints, the arterial depth corresponded to 52% ± 18% of the metatarsal height in the first metatarsal and 67% ± 19% in the second metatarsal. Mean metatarsal lengths were 61.2 ± 3.1 mm (first) and 74.5 ± 3.7 mm (second).
Conclusions:
Distal to the TMT joints, the dorsalis pedis artery initially courses plantarly and gradually returns dorsally. These findings provide quantitative anatomical information regarding the trajectory of the dorsalis pedis artery in the intermetatarsal region distal to the TMT joints. Awareness of this depth trajectory may help surgeons minimize unnecessary arterial contact, particularly during screw placement across the intermetatarsal space.
Level of evidence:
Level V, cadaveric anatomical study.
Introduction
The dorsalis pedis artery originates from the anterior tibial artery, passes beneath the inferior extensor retinaculum, and courses distally beneath the extensor hallucis brevis muscle. After giving rise to the arcuate artery, it continues as the first dorsal metatarsal artery, which runs between the first and second metatarsals. The deep plantar branch arises from this vessel and contributes to the plantar arterial arch, whereas the dorsal branch continues distally and divides into branches that supply the hallux and second toe.1-3
Surgical procedures involving the region between the first and second metatarsals distal to the first and second tarsometatarsal (TMT) joints are commonly performed. These include Lisfranc joint fixation, first TMT joint arthrodesis (modified Lapidus procedure), first metatarsal osteotomy for hallux valgus, and second metatarsal shortening osteotomy.4-7 During these procedures, instrumentation use, including screw fixation and osteotomies, is frequently performed across or adjacent to the intermetatarsal space, where the dorsalis pedis artery and its branches are located.
Although this artery is part of a well-developed collateral network, its anatomical course in relation to commonly used surgical trajectories may be relevant when considering hardware placement. Previous studies have described the proximity of neurovascular structures to intermetatarsal screw fixation. However, detailed quantitative information regarding the plantar-dorsal depth of the dorsalis pedis artery distal to the TMT joints remains limited.
The purpose of this study was to characterize the depth of the dorsalis pedis artery (including the first dorsal metatarsal artery), relative to metatarsal height at defined intervals distal to the first and second TMT joints and provide quantitative anatomical data that may assist in understanding its spatial relationship with common surgical approaches.
Materials and Methods
Twelve fresh frozen human cadavers were obtained from an accredited anatomical donation program. A total of 19 feet (7 male and 5 female specimens) were included, with a mean age of 74.2 years (range, 57-92 years). All cadavers were thawed overnight at room temperature for 1 day prior to dissection. Lower limbs were sectioned below the knees for analysis.
Dissection
A 14-G needle was inserted into the femoral artery and the proximal portion of the puncture site was ligated. Thirty milliliters of MICROFIL silicone rubber compound (Flow Tech Inc, Carver, CA; comprising 12 mL of compound, 15 mL of diluent, and 3 mL of curing agent) was injected into the femoral artery to visualize the vessels. 8 One hour after injection, dissection was performed to expose the Lisfranc joint, including the first and second TMT joints, confirming the courses of the neurovascular structures of interest. Their distances from the TMT joints were also measured.
Measurements
The following parameters were recorded: (1) length of the first and second metatarsals, (2) distance from the TMT joint to the branching point of the plantar artery, and (3) depth of the first dorsal metatarsal artery. The first and second metatarsals were marked at 10-mm intervals from their respective TMT joints for depth measurements. The arterial depth was measured at each point using a caliper, with the dorsal cortical surface of the metatarsal defined as 0%. At each measurement point, the caliper was positioned perpendicular to the dorsal cortical surface and centered over the arterial lumen to ensure consistent measurements. The depth ratio was then calculated as the measured depth (a) divided by the total vertical height of the metatarsal (b), and expressed as a percentage using the following equation: a/b × 100 (Figure 1).

(A) The first and second metatarsals were marked at 10-mm intervals distal to each tarsometatarsal joint. Solid lines indicate the TMT joints, whereas dotted lines indicate the 10-mm measurement intervals. (B) At each measurement point, the dorsal cortical surface was defined as 0%, and the arterial depth (a) was measured perpendicular to this surface. The depth ratio was calculated as a percentage of the metatarsal height (a/b × 100). The branching point of the deep plantar branch is indicated by the arrow.
Results
The mean lengths of the first and second metatarsals were 61.2 ± 3.1 mm and 74.5 ± 3.7 mm, respectively. The branching point of the deep plantar branch from the dorsalis pedis artery was located 11.0 ± 3.5 mm distal to the first TMT joint and 22.3 ± 4.5 mm distal to the second TMT joint.
The mean depths of the dorsalis pedis artery at each measurement point are presented in Table 1, including absolute depth values (mm) expressed as mean ± SD. The absolute depth values demonstrated a consistent trend with the artery located progressively deeper distally before returning dorsally.
Measured Arterial Depth at Each Point, Expressed as an Absolute Value and as a Percentage of the Metatarsal Height Over the First and Second Metatarsals. a
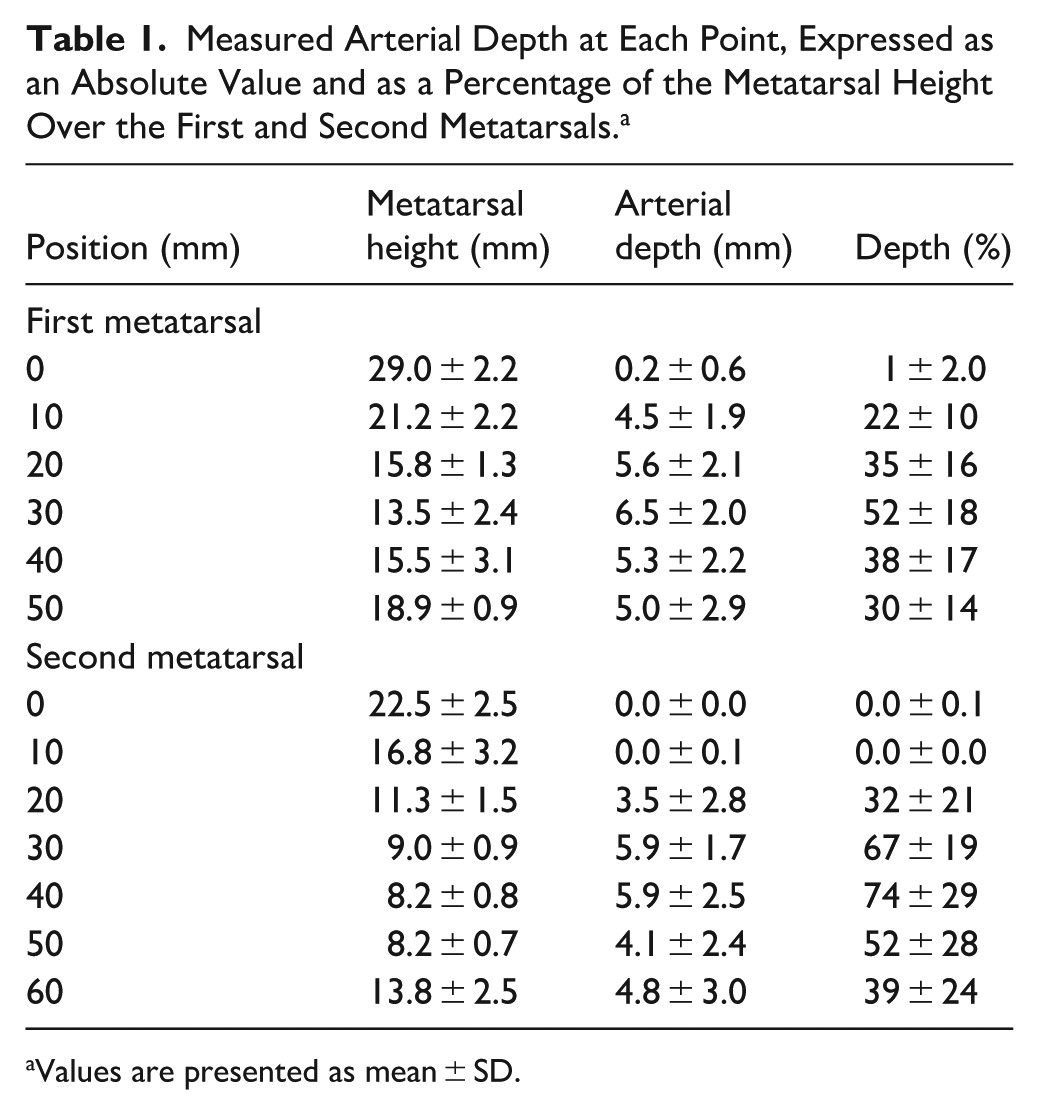
Values are presented as mean ± SD.
When expressed as percentages of the metatarsal height, these depths corresponded to 1% ± 2.0%, 22% ± 10%, 35% ± 16%, 52% ± 18%, 38% ± 17%, and 30% ± 14%, respectively, in the first metatarsal; and 0.0% ± 0.1%, 0.0% ± 0.0%, 32% ± 21%, 67% ± 19%, 74% ± 29%, 52% ± 28%, and 39% ± 24%, respectively, in the second (Table 1).
Variability in arterial depth across specimens was observed at all measured levels.
Discussion
The first dorsal metatarsal artery initially courses deeper and gradually returns dorsally. Beyond 20 mm distal to the TMT joints, the artery was located deeper than approximately 30% of the metatarsal height; at 30 mm, it reached 52% in the first metatarsal and 67% in the second metatarsal. The deep plantar branch originated approximately 10 mm distal to the first TMT joint, where the arterial course tended to be transverse.
These findings are relevant because many surgical procedures, including first metatarsal osteotomy, TMT joint arthrodesis, Lisfranc procedures, and second metatarsal shortening osteotomy require instrumentation in proximity to the intermetatarsal space. Rather than implying that the artery must be avoided entirely, our results provide quantitative information regarding its depth trajectory, which may assist surgeons in understanding its spatial relationship with commonly used screw paths. These findings may also be relevant to other procedures involving the intermetatarsal region, including Lisfranc debridement, second-metatarsal shortening osteotomy, and percutaneous forefoot surgeries. These considerations may be most relevant in patients with a compromised vascular status, such as those with peripheral vascular disease, or in revision settings where collateral circulation may be reduced.
A previous cadaveric study by So et al 9 demonstrated that more distal screw placement increases the likelihood of neurovascular contact during Lapidus procedures. Our findings complement these observations by providing depth-based data, showing that the artery occupies a relatively deeper position beyond 20 to 30 mm distal to the TMT joints. This information may be particularly relevant when considering screw trajectories that traverse the intermetatarsal space (Figure 2).
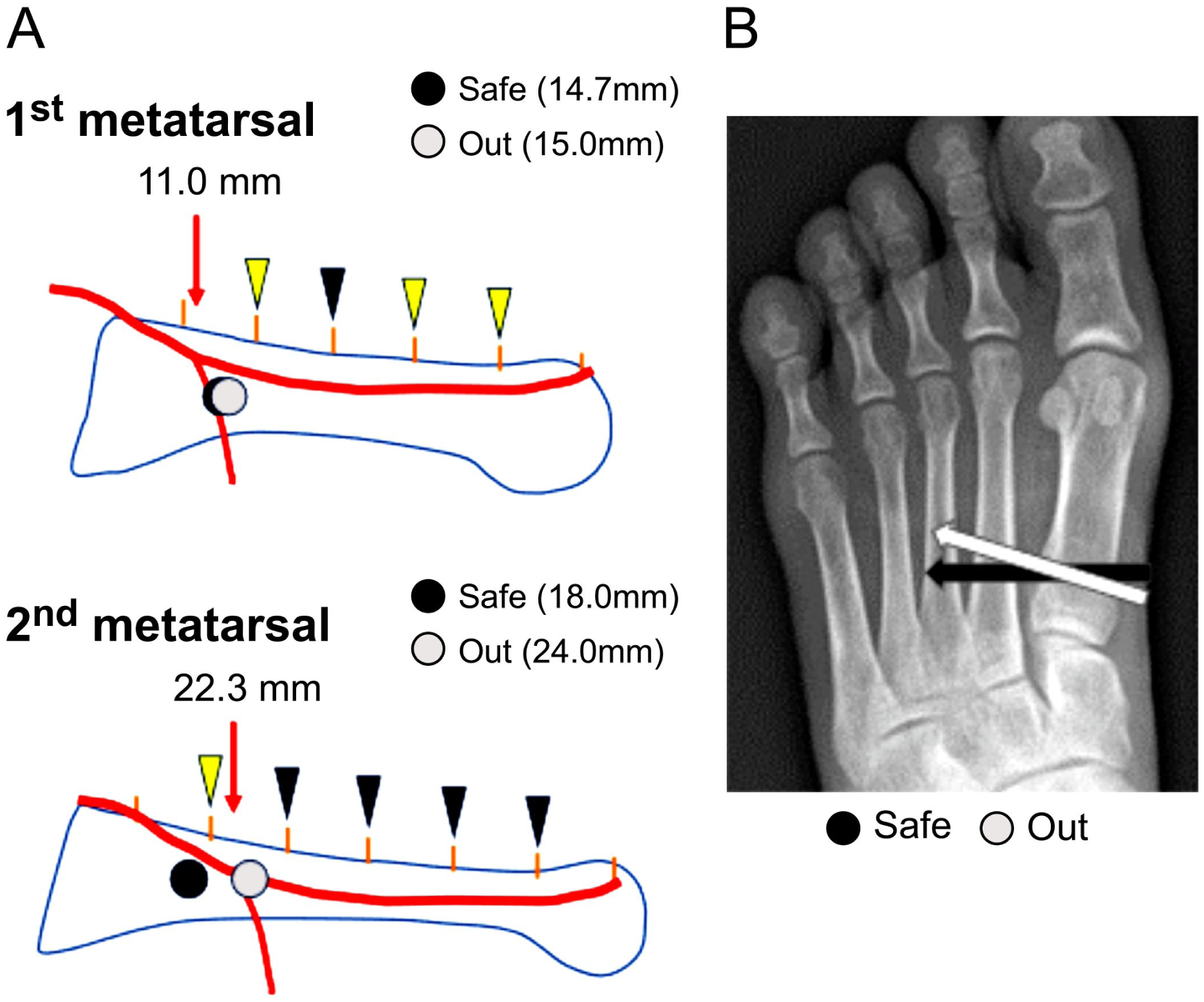
Relative positional relationship between our findings and those reported by So et al. 9 (A) In the first metatarsal, a representative screw insertion point is distal to the bifurcation of the deep plantar artery. In the second metatarsal, a more distal screw insertion may increase the risk of arterial contact. Yellow arrowheads indicate depths of ≥30%, whereas black ones indicate depths of ≥50%. (B) Schematic radiographic illustration showing that more distal screw trajectories predict higher likelihoods of arterial contact.
Importantly, the dorsalis pedis artery is part of a well-developed collateral network via the plantar arch, and an isolated injury may not always result in clinically significant ischemia. Vascular complications following procedures such as Lapidus or Lisfranc fixation appear to be relatively rare, with most reports being limited to isolated case studies. However, complications including pseudoaneurysm formation, arteriovenous fistula, and other vascular injuries have been described and are often attributed to mechanical irritation or compression by the surgical hardware. These complications are thought to arise not only from direct penetration of the vessel, but also from repeated mechanical contact between the surgical hardware and the artery, which may lead to progressive vessel wall damage over time. For example, Kvas and Jorgensen 10 reported a case of dorsalis pedis artery pseudoaneurysm following fixation, attributed to repeated mechanical irritation of the vessel by the adjacent hardware. Despite this collateral circulation, such injuries may still result in clinically relevant consequences, including persistent pain, swelling, or the need for reoperation.11,12 Therefore, the findings of the present study should be interpreted as providing precautionary anatomical information to improve surgical awareness, rather than addressing a frequently encountered clinical complication. These findings suggest that the clinical relevance of this study lies in improving anatomical awareness rather than defining a strict “high-risk” zone.
We also observed variability in arterial depth and branching patterns among specimens, consistent with previous reports of anatomical variation. 11 Recent anatomical studies have further characterized perforator-based variations of the first dorsal metatarsal artery. 12 Although subgroup analysis by sex or laterality was not performed, this variability suggests that a uniform surgical trajectory may not be appropriate in all cases, highlighting the importance of intraoperative awareness of vascular anatomy.
By quantifying the plantar-dorsal position of the artery relative to metatarsal height, this study provides objective anatomical reference data that may assist in surgical planning.
Limitations
This study has several key limitations. First, the sample size was determined based on cadaver availability, which is a practical limitation. None of the specimens had hallux valgus or claw-toe deformities; therefore, the observed anatomical relationships may differ from those observed in real-world clinical cases that require surgical treatment. Second, all measurements were performed individually for each specimen relative to the first and second metatarsals, without assessing the positional relationship between the 2 metatarsals. Lastly, although all dissections were performed carefully, soft tissue removal to identify the neurovascular structures may have altered their original positions.
Conclusion
The dorsalis pedis artery coursed plantarly after giving rise to the deep plantar branch, and then gradually returned dorsally. At 30 mm distal to the TMT joints, the artery was located at 52% ± 18% of the metatarsal height in the first metatarsal and 67% ± 19% in the second metatarsal, with a more transverse course distally. These findings may assist in understanding the spatial relationship between screw placement and arterial course, particularly with respect to distal positioning and dorsally angulated screw trajectories, and may also be relevant to other procedures involving the intermetatarsal region, including Lisfranc debridement, second metatarsal shortening osteotomy, and percutaneous forefoot procedures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261461267 – Supplemental material for Depth of the Dorsalis Pedis Artery Distal to the First and Second Tarsometatarsal Joints: A Cadaveric Anatomical Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114261461267 for Depth of the Dorsalis Pedis Artery Distal to the First and Second Tarsometatarsal Joints: A Cadaveric Anatomical Study by Taro Fujimaki, Hiroaki Kurokawa, Yuki Ueno, Takahide Sasaki, Kouhei Mitsui, Akira Taniguchi, Hirotaka Haro, Pasuk Mahakkanukrauh and Yasuhito Tanaka in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
This study was conducted in accordance with institutional ethical standards for the use of human cadaveric specimens and the principles of the Declaration of Helsinki. Formal institutional review board approval was waived because this study involved donated cadaveric material.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.