
Abstract
Introduction:
Disparities in medical education are documented across the training continuum, yet little is known about how racial and socioeconomic factors shape disciplinary actions during residency.
Methods:
We conducted a cross-sectional anonymous survey of resident physicians affiliated with the Committee of Interns and Residents. The survey captured demographic characteristics and experiences with negative feedback, remediation, and discipline. We used descriptive statistics and logistic regression.
Results:
We analyzed 1,755 validated responses (9.2% completion). Compared with White participants, Black participants had higher odds of being asked to meet with program leadership (unadjusted odds ratio [OR] = 1.93, 95% confidence interval [CI]: 1.32–2.82), and this association strengthened after adjustment for gender, specialty type, and early-life socioeconomic indicators (adjusted OR [AOR] = 2.24, 95% CI: 1.48–3.38). Black participants were nearly three times as likely to report ever being on remediation (OR = 2.93, 95% CI: 1.51–5.72), although adjusted models were limited by small event counts. When disciplinary outcomes were combined, Black participants were 55% more likely than White participants to experience any disciplinary action in unadjusted analyses (OR = 1.55, 95% CI: 1.10–2.19), and this association strengthened after adjustment (AOR = 1.76, 95% CI: 1.21–2.57). Hispanic and Asian participants did not demonstrate higher odds of disciplinary action compared with White participants.
Conclusion:
Racial and socioeconomic inequities in residency discipline challenge assumptions that discipline reflects merit alone. Programs should implement transparent, uniform disciplinary processes and create supportive training environments for all trainees.
Keywords
Introduction
The underrepresentation of Black physicians in the U.S. workforce is longstanding. Although Black Americans make up 13% of the U.S. population, they comprise only 5% of medical residents and 4% of practicing physicians. 1
Structural barriers in medical education are well documented across all stages of training, including disparities in evaluation, grading, and access to mentorship. However, disproportionate discipline during residency has received comparatively limited empirical attention and is frequently discussed through anecdotal accounts or framed as reflecting individual performance deficits rather than systemic conditions. These narratives overlook the fact that all residents, regardless of race, have met standardized academic and professional criteria for entry into training. What is often characterized as individual failure may instead reflect bias embedded within residency program structures.
Calls for robust empirical data to substantiate or refute concerns about racial bias in resident discipline have intensified, particularly as Black residents report differential treatment, limited access to mentorship, and disciplinary processes that lack transparency or due process.2–5 Although the field of medical education has acknowledged disparities in performance evaluations,6–9 few studies have focused specifically on remediation and dismissal—high-stakes processes that can abruptly end a physician’s career.10,11
This study aims to fill a critical knowledge gap by presenting survey data on racial disparities in disciplinary actions during residency, based on the experiences of resident physician members of the Committee of Interns and Residents (CIR), the largest house staff union in the United States. 12
Methods
Study design and oversight
This cross-sectional survey study was conducted by Black Doc Village, Inc., in collaboration with the CIR and EVITARUS, an independent research firm. Black Doc Village, Inc. is a 501(c) 3 nonprofit organization dedicated to raising awareness about the disproportionate dismissal of Black resident physicians and leveraging research to inform policy change. CIR represents roughly one-third of resident physicians in the United States, primarily from residency programs in the western and northeast regions of the country. 12 We partnered with the CIR to distribute the survey through a trusted and established communication channel. At present, the Accreditation Council for Graduate Medical Education (ACGME) is the only entity that maintains a comprehensive national roster of residents with contact information, and these data are not publicly accessible for independent research. Collaborating with CIR therefore allowed us to reach a large, geographically diverse, multispecialty cohort of trainees in a feasible manner. The study aimed to examine racial disparities in negative disciplinary experiences among resident physician members of CIR. It was reviewed and approved by the PEARL institutional review board (IRB ID: 2024-0134) on April 24, 2024.
Participant recruitment
Eligible participants were resident physicians affiliated with CIR. CIR distributed study invitations to 26,148 email accounts, representing ∼19,600 resident members. The initial email yielded a 37.46% open rate. To improve participation, the following recruitment strategies were implemented:
A reminder email was sent to the same distribution list, achieving a 35% open rate. CIR featured two pop-out survey reminders on its homepage. CIR promoted the survey through its social media accounts—X (formerly Twitter; 8,684 followers), Facebook (12,000 followers), and Instagram (15,600 followers). CIR’s 12 regional Diversity Affinity Groups were provided with a branded social media toolkit to share study information with their members. A follow-up message from EVITARUS was emailed to respondents who completed the survey, encouraging peer outreach.
All recruitment materials directed participants to a survey landing page that included an online consent form. Proceeding to the survey required active acknowledgment of consent. Upon completion of the survey, participants were offered a $10 e-gift card to a major retailer of their choosing (e.g., Amazon or Target).
Survey instrument
The survey instrument was developed through a structured, multi-step process. An advisory committee of 13 members was convened specifically for this study. The committee included representatives from key national organizations (American Medical Association, Association of American Medical Colleges, National Medical Association, and ACGME), as well as individuals across the medical education continuum (program director, attending physician, fellow, resident, and medical student) and subject-matter experts in research and policy. Members were intentionally diverse with respect to race/ethnicity, gender, and specialty.
An initial draft of the survey was developed by the lead investigator based on prior literature, existing frameworks on disciplinary processes in graduate medical education, and documented resident narratives. The draft instrument was reviewed during two structured virtual advisory committee meetings composed of subject-matter experts in Graduate Medical Education (GME), equity research, and resident advocacy. Iterative revisions were made between sessions, and survey items were finalized by consensus to ensure alignment with predefined domains of interest.
The instrument subsequently underwent external review by EVITARUS to assess clarity, readability, length, and usability, with additional refinements made to minimize respondent burden. This structured expert review and iterative refinement process was designed to support content validity. Formal psychometric validation (e.g., factor analysis or reliability testing) was not conducted prior to administration.
The survey consisted of structured, closed-ended questions designed to gather quantitative data in the following domains:
Demographics: Race/ethnicity, gender identity, citizenship status, first-generation college or doctoral status, and childhood background (early-life circumstances, including household income during upbringing, biological parents’ birthplaces, and selected formative life events). Residency characteristics: Specialty, postgraduate year, U.S. region of training, and perceived diversity within the program (i.e., how many peers in their residency program shared their race/ethnicity or gender). Disciplinary experiences: Encounters with negative feedback, informal or formal remediation, documentation practices, escalation to leadership, and perceptions of due process. Remediation and probation: Types of competencies cited, clarity of goals, availability of legal or institutional support, and perceptions of justification and fairness. ACGME core competencies: If respondents reported being placed on remediation or probation, they were asked to identify the specific ACGME competencies cited. The ACGME established six core competencies in 1999 as the standardized framework for resident evaluation across all U.S. residency programs.
13
These competencies are intended to define the fundamental skills and attributes of physicians and include the following:
Practice-based learning and improvement: Engaging in self-evaluation and continuous learning to improve patient care. Patient care and procedural skills: Delivering compassionate, appropriate, and effective patient care. Systems-based practice: Understanding and navigating the health care system to optimize care delivery. Medical knowledge: Applying biomedical, clinical, and social sciences to patient care. Interpersonal and communication skills: Communicating effectively with patients, families, and colleagues. Professionalism: Adhering to ethical principles and demonstrating responsibility and integrity in medical practice. Respondents could select one or more competencies as the stated reason for their remediation or probation.
The final survey was administered only between April 29 and August 5, 2024. The estimated survey completion time was 10–15 min. Responses were anonymous. The survey was conducted as part of a larger mixed-methods study that also included semi-structured interviews; qualitative findings are reported separately due to word count limitations. The full survey instrument is included in Supplementary Data.
Data analysis
Data were analyzed using Stata v. 19 (StataCorp, College Station, TX). Descriptive statistics were used to characterize the sample and examine the frequency and distribution of disciplinary actions across demographic subgroups. Bivariate comparisons were conducted using chi-square and Fisher’s exact tests, as appropriate.
Participants self-identified race and ethnicity and could select multiple categories. Respondents selecting “Mixed/Other” also selected either White or Asian; no respondents identifying as Black or Hispanic selected “Mixed/Other.” For analytic clarity, individuals selecting White and Mixed/Other were classified as White, and those selecting Asian and Mixed/Other were classified as Asian. Final analytic categories were Black, White, Asian, Hispanic, and Other (including Pacific Islander, Native American, and Middle Eastern). These “Other” groups were combined to protect against potential identification of participants due to small numbers.
To explore how disciplinary disparities may be shaped by both structural and cultural factors, we conducted subgroup analyses by ethnicity (American Descendants of Slavery [ADOS] vs. African immigrant), specialty type (medical vs. surgical), and gender identity. Differences between Black participants identifying as ADOS and those who are African immigrants or children of immigrants have been described in prior literature, reflecting distinct historical, cultural, and socioeconomic contexts. ADOS individuals are more likely to have ancestral and lived experiences of U.S. structural racism across generations, which may contribute to differential treatment and vulnerability within academic institutions, including graduate medical education.14,15
We also examined differences by specialty type, as surgical residencies often involve smaller training teams, hierarchical cultures, and high-stakes procedural performance that may intensify evaluation-related power dynamics. 16 Medical specialties included dermatology, emergency medicine, family medicine, internal medicine, internal medicine–pediatrics, neurology, pathology, pediatrics, physical medicine and rehabilitation, podiatry, psychiatry, radiation oncology, and radiology. Surgical specialties included anesthesiology, dentistry, general surgery, neurological surgery, oral and maxillofacial surgery, obstetrics and gynecology, ophthalmology, orthopedic surgery, otolaryngology, plastic surgery, and urology.
Gender was included due to well-documented differences in how men and women are evaluated during training, particularly in subjective domains such as communication and professionalism. 17 Multivariable logistic regression models were constructed to evaluate associations between race and disciplinary outcomes, adjusting for gender, specialty type (surgical vs. medical), and indicators of early-life social position (childhood poverty, first-generation college status, and first-generation doctorate status). Covariates were selected a priori based on conceptual relevance. For rare disciplinary outcomes, exact logistic regression methods were used in crude analyses. Multivariable models were restricted to covariates supported by available event counts to reduce the risk of overfitting.
Results
Participant characteristics
Of the 19,300 emails sent to resident physician members inviting study participation, we obtained 1,755 validated survey responses, representing a 9.2% completion rate. Participant characteristics by race/ethnicity are shown in Table 1. In keeping with the location of CIR membership, most participants were from residency programs in the Northeast (n = 810, 46.3%) and West (n = 696, 39.8%). More than half identified their gender as cisgender female (n = 954, 56.2%). Roughly two-thirds of study participants identified as Asian (n = 652, 38.2%) or White (n = 556, 32.6%), while the remaining one-third identified as Hispanic (n = 216, 12.7%), Black (n = 191, 11.2%), or other groups (Pacific Islander, Native American, or Middle Eastern) (n = 91, 5.2%). Among participants identifying as Black, approximately one-fourth (n = 50, 26.2%) were ADOS. The largest number of participants were in their first year of training (n = 510, 29.2%), followed by those in their second year of training (n = 462, 26.5%). The majority of participants were in medical specialties (n = 1,346, 80.5%), with internal medicine being the most common specialty (n = 363, 21.7%).
Characteristics of Study Population, Overall and by Race/Ethnicity

an = 46 missing race information.
bChi-square or Fisher’s exact, as appropriate.
cFor cis-male vs. cis-female only.
dn = 82 were excluded due to nonresidency (cardiology, nephrology, heme/onc) or responses of “prefer not to answer,” “transitional year,” or “other.”
eOther includes: Anesthesiology (n = 82), Dentistry (n = 12), Dermatology (n = 26), Internal Medicine/Pediatrics (n = 78), Neurology (n = 43), Neurological Surgery (n = 4), Obstetrics/Gynecology (n = 68), Ophthalmology (n = 29), Otolaryngology (n = 18), Oral And Maxillofacial Surgery (n = 13), Orthopedic Surgery (n = 24), Pathology (n = 36), Physical Medicine and Rehabilitation (n = 21), Plastic Surgery (n = 7), Podiatry (n = 12), Radiation Oncology n = 4), Radiology (n = 57), Urology (n = 20).
ADOS, American Descendants of Slavery; SDOS, Social Determinants of Success (childhood poverty, first-generation college, first-generation doctorate).
Black and Hispanic participants were more likely than participants from other racial/ethnic groups to be the first in their family to attend college or to earn any doctorate degree. These participants were also more likely to have been raised in poverty (childhood income <$50,000 annually). Overall, 19.9% of all study participants were first-generation college graduates compared to 27.5% and 35.2% of Black and Hispanic participants, respectively. Similarly, 59.9% of all study participants were first-generation doctorates, compared with 68.8% and 69.0% of Black and Hispanic participants, respectively. While 27.5% of all study participants were raised in poverty, 39.9% and 44.9% of Black and Hispanic participants met this criteria, compared with only 13.2% of White participants.
Black and Hispanic participants were more commonly “the only one” in their residency program. When asked how many of their peers (residents in same program specialty) were of the same race or ethnicity, 27.2% and 29.3% of Black and Hispanic participants, respectively, reported that there was no or only one other peer, compared to 9.1% and 20.9% of White and Asian participants.
Negative disciplinary actions
Frequencies of participants reporting negative disciplinary actions by race/ethnicity are shown in Figure 1. Overall, one-fifth of participants (n = 343, 20.4%) reported having to meet with their program director or other faculty leadership because of negative comments made by a peer/other resident, attending physician, other staff member (e.g., nurse or clerk), or patient/family member. Black participants more often reported such comments (29.5%) than White (17.8%), Hispanic (20.5%), Asian (19.1%), or Other (24.4%) participants (p = 0.009). Negative comments most often came from attending physicians (46.5%), peers (37.1%), and other staff members (35.7%), but rarely from patients/family members (9.4%). Black participants reported that peers were the source of negative comments (57.1%) more frequently than White (33.7%), Hispanic (27.3%), Asian (34.2%), or Other (50.0%) participants (p = 0.008). Most participants felt this action was unwarranted because they had done nothing wrong (n = 175, 49.6%) or excessive in that the same disciplinary action would not have happened to anyone else who made a similar mistake (n = 120, 34.0%). Black participants more frequently reported excessive disciplinary action (44.6%), compared with White (32.7%), Hispanic (22.7%), Asian (38.2%), or Other (18.2%) participants, although this difference was not statistically significant (p = 0.10). More than half of Black participants (60.8%) felt their race factored into these matters “a lot,” compared with White (2.3%), Hispanic (23.5%), Asian (13.6%), or Other (13.6%) participants (p < 0.001). Two-thirds of these participants (n = 220, 66.7%) reported the individual(s) making negative comments about them had never attempted to discuss the matter with them first, regardless of participant race (p = 0.9).

Frequencies of participants reporting negative disciplinary actions by race/ethnicity.
More than a quarter of participants (n = 484, 29.3%) reported receiving a negative written evaluation that was not discussed with them beforehand. Among those reporting such an evaluation, only 9.6% (n = 45) reported being allowed to submit a written rebuttal, whereas 43.5% reported that they had not asked to submit a written rebuttal. These responses did not vary by race (p = 0.5).
Few participants overall reported disciplinary actions defined as current remediation, probation, or facing dismissal (n = 44, 2.5%); however, this status was more commonly reported by Black participants (n = 11, 5.8%) than White (n = 11, 2.0%), Hispanic (n = 5, 2.4%), Asian (n = 12, 1.9%), and Other (n = 4, 4.5%) participants, p = 0.03. Deficiencies in “medical knowledge” (47.7%) and “interpersonal and communication skills” (47.7%) were the most common core competencies cited for these disciplinary actions, whereas “professionalism” was infrequently cited (9.1%). These responses did not vary by race (p > 0.2). Regardless of race, most participants did not feel that the cited reasons justified the disciplinary action (n = 33, 82.5%), that the goals to be reinstated to good standing were clear and achievable (n = 22, 59.6%), or that the program was following its due process policy (n = 23, 71.9%). Notably, nearly one-quarter (23.8%) of all study participants disagreed with the statement: “I believe the core competencies by which I am being evaluated are sufficiently objective.”
Being a first-generation college graduate was associated with an increased likelihood of being asked to meet with program leadership (odds ratio [OR] = 1.61, 95% confidence interval [CI]: 1.22–2.12) and of being on remediation, either currently (OR = 2.25, 95% CI: 1.19–4.25) or ever (OR = 2.88, 95% CI: 1.83–4.55). Neither being the first doctorate holder in one’s family nor experiencing childhood poverty were associated with negative disciplinary actions.
Overall, participants in surgical specialties were more likely than those in medical specialties to be asked to meet with program leadership (OR = 1.54, 95% CI: 1.16–2.04). When stratified by race, this association appeared stronger among Black participants (OR = 3.26, 95% CI: 1.47–7.20) than White participants (OR = 1.68, 95% CI: 1.02–2.77); however, the race-by-specialty interaction did not reach statistical significance (p = 0.054), indicating that differences in effect size should be interpreted cautiously. Similarly, women in surgical specialties were more likely than women in medical specialties to report ever receiving a negative written evaluation (OR = 1.73, 95% CI: 1.19–2.50). This association did not differ significantly by race (p = 0.288 for interaction). There were no other statistically significant differences in negative disciplinary experiences among resident physicians in surgical specialties versus medical specialties.
Associations between disciplinary actions and race/ethnicity are shown in Table 2. Compared with White participants, Black participants were nearly twofold more likely to report having to meet with program leadership (unadjusted OR = 1.93, 95% CI: 1.32–2.82). Adjustment for gender, residency type (surgical vs. medical), and social determinants of success strengthened the association for Black and Other participants (adjusted OR [AOR] = 2.24, 95% CI: 1.48–3.38 and AOR = 1.89, 95% CI: 1.07–3.35, respectively). Compared with White participants, there was no difference in Hispanic and Asian participants’ likelihood of being asked to meet with program leadership in unadjusted or adjusted models. Compared with White participants, Hispanic and Asian were less likely to report ever having a negative written evaluation (unadjusted OR = 0.66, 95% CI: 0.46–0.96 and unadjusted OR = 0.75, 95% CI: 0.58–0.97, respectively). While Black participants had a 55% higher likelihood of reporting to ever have a negative written evaluation after adjustment (AOR = 1.55, 95% CI: 1.05–2.27), the association attenuated after adjustment for Hispanic and Asian participants. Compared with White participants, Black participants were threefold more likely to report being currently on remediation (unadjusted OR = 3.02, 95% CI: 1.17–7.83), remediation in the past (unadjusted OR = 3.01, 95% CI = 1.16–7.80), or ever being on remediation combined (OR = 2.93, 95% CI = 1.51–5.72); however, statistical adjustment was not possible due to the small number of outcomes. There was no statistically significant difference for these outcomes for Hispanic and Asian participants compared with White participants. Compared with White participants, Black participants were 55% more likely to have any disciplinary action (asked to meet with leadership, negative written evaluation, ever remediation) (unadjusted OR = 1.55, 95% CI: 1.10–2.19), and this association strengthened after adjustment (AOR = 1.76, 95% CI: 1.21–2.57). There was no statistical difference in the likelihood of the combined outcome for Hispanic or Asian participants compared with White participants. Among Black participants, point estimates suggested that ADOS were twofold more likely to be asked to meet with leadership and have any negative disciplinary action (OR = 2.17, 95% CI: 1.10–4.29 and OR = 1.90, 95% CI = 0.96–3.77, respectively) than Black participants who were immigrants or children of immigrants, although the latter association was not statistically significant.
Associations of Disciplinary Actions by Race/Ethnicity
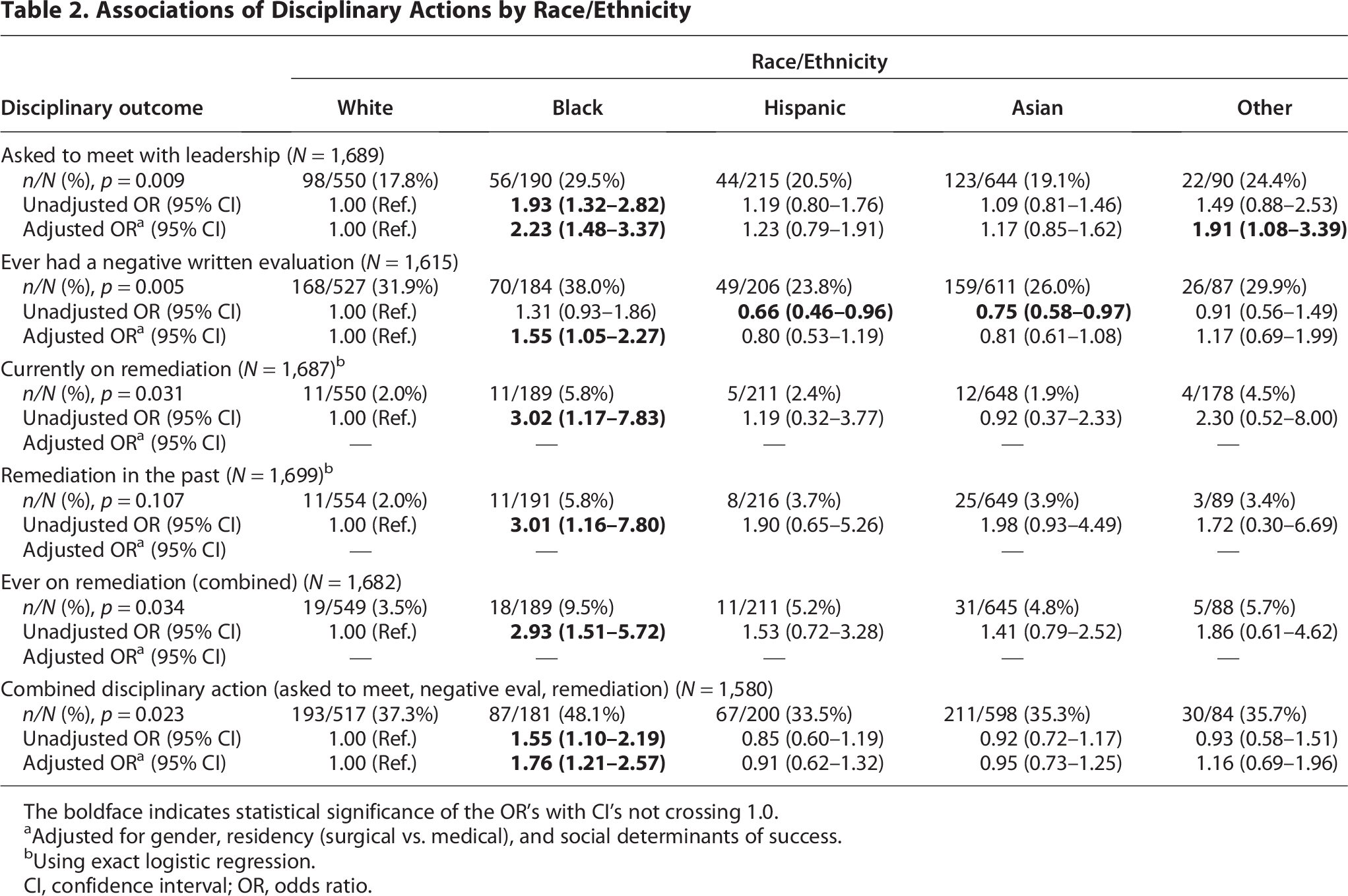
The boldface indicates statistical significance of the OR's with CI's not crossing 1.0.
aAdjusted for gender, residency (surgical vs. medical), and social determinants of success.
bUsing exact logistic regression.
CI, confidence interval; OR, odds ratio.
Discussion
To the best of our knowledge, this is the first national survey to examine resident disciplinary experiences alongside detailed demographic and socioeconomic characteristics across specialties. Existing GME datasets typically report race/ethnicity and gender without incorporating intersecting factors such as socioeconomic background or first-generation status, 18 and large-scale resident surveys often emphasize program-level or clinical metrics rather than disciplinary processes.4,19,20 By intentionally collecting granular demographic data and focusing on remediation and disciplinary action, this study extends the current evidence base and contributes new insight into how structural inequities may manifest during residency training.
Black participants had significantly higher odds of experiencing negative disciplinary action compared with their White peers, even after adjustment for gender, specialty type, and social determinants of success. Notably, adjustment did not attenuate this association and, in some models, strengthened it. In contrast, most comparisons involving Hispanic and Asian participants were not statistically different from those involving White participants. This pattern suggests that disparities were not diffuse across all racial and ethnic groups but were concentrated among Black participants.
Black and Hispanic participants were more likely to report markers of educational disadvantage, including being the first in their families to attend college or earn a doctoral degree and growing up in lower-income households. However, among these factors, only first-generation college status was independently associated with increased odds of leadership meetings and remediation. Neither childhood poverty nor first-generation doctorate status explained the observed racial disparities. Taken together, these findings narrow alternative explanations and suggest that socioeconomic background alone does not account for the disproportionate disciplinary experiences reported by Black participants.
Residents from historically excluded backgrounds may be less privy to the “hidden curriculum” of medical training: the unspoken expectations, informal codes, and institutional power dynamics that influence evaluation and advancement. 21 These dynamics may be compounded by what has been described as the “haunted curriculum,” in which learners of color are disproportionately subject to negative evaluations shaped by unacknowledged bias, often without transparency or recourse. 22 Such frameworks provide a conceptual lens through which disparities in disciplinary processes may emerge even when formal policies appear uniform.
Although differences in perceived excessiveness of disciplinary responses did not reach statistical significance, Black participants were markedly more likely to report that race played a substantial role in how disciplinary matters were handled. This distinction underscores that the occurrence of disciplinary action and the experience of that action are not interchangeable constructs. Similar event counts do not preclude differences in tone, scrutiny, expectations, or perceived fairness. Perceptions of racialized treatment may reflect qualitative differences in process that are not fully captured by binary measures of disciplinary occurrence.
Our findings also reveal important distinctions within the Black resident population. Participants who identified as ADOS were approximately twice as likely to report disciplinary encounters compared with Black participants who were African immigrants or children of immigrants. Although often grouped together under the category of “Black,” these subgroups may experience residency training differently. ADOS residents carry a distinct historical legacy shaped by U.S. slavery, Jim Crow, and intergenerational structural exclusion from wealth-building and educational opportunity.14,15 In contrast, African and Afro-Caribbean immigrant physicians may arrive with different forms of educational or social capital and may be perceived differently within institutional hierarchies. This dynamic, sometimes described as the “immigrant advantage,” may obscure subgroup-specific vulnerabilities even within racial diversity initiatives. 23
Faculty and leadership demographics may further shape disciplinary environments. National database studies document persistent underrepresentation of Black faculty and program leaders across specialties 24 and demonstrate racial disparities in surgical residency attrition and advancement.10,11 In contexts where evaluative authority is disproportionately concentrated among majority-group faculty, unconscious bias, differential mentorship access, and cultural incongruence may influence both the likelihood and interpretation of performance concerns. Although this study did not capture faculty demographic composition, these broader workforce patterns provide important structural context for understanding how disciplinary disparities may persist within GME systems.
Our findings are unlikely to be explained by differences in academic performance alone. Prior research demonstrates that racial gaps in standardized metrics narrow or abate during training, 25 and entrance examination scores have limited predictive value for long-term clinical competence. 26 The persistence of disciplinary disparities at this advanced stage suggests that institutional processes, rather than baseline qualifications, warrant closer examination.
We also observed concerning patterns regarding procedural fairness. Participants across racial groups reported receiving negative evaluations without prior discussion and being afforded limited opportunity to submit rebuttals. Among those placed on remediation or probation, many did not feel the reasons were justified or that expectations for returning to good standing were clearly defined. Such practices undermine the principle that GME should provide consistent and transparent developmental support, even when performance concerns arise.
Disciplinary disparities carry implications beyond individual career trajectories. Physician–patient racial concordance has been associated with improved communication, patient trust, and health outcomes.27–29 Disproportionate attrition of Black residents may, therefore, undermine efforts to build a physician workforce capable of delivering equitable care.
These findings have important implications for GME policy and oversight. Residency programs receive more than $16 billion annually in federal GME funding through the CMS. 30 As publicly supported institutions, they bear responsibility for ensuring equitable training environments. Accreditation bodies such as the ACGME should consider requiring routine reporting of remediation and dismissal data disaggregated by race, gender, and first-generation status. Standardized training in equitable evaluation practices, due process procedures, and mentorship may further strengthen accountability. Residents should also have access to independent ombuds services and peer advocacy networks to safely raise concerns without fear of retaliation.
Limitations
This study has several limitations. First, the overall response rate was 9.2%. Although this is comparable to other voluntary national physician surveys,31,32 nonresponse bias cannot be excluded. Residents with particularly strong or negative experiences may have been more likely to participate, potentially influencing the observed associations. Second, the sample included only resident physicians affiliated with CIR, which may constrain generalizability to nonunionized programs or geographic regions underrepresented in CIR membership. Third, disciplinary experiences and perceptions of fairness were self-reported and are therefore subject to recall bias and subjective interpretation. However, perceptions of racial influence and procedural fairness are themselves meaningful indicators of institutional climate. Fourth, the survey instrument did not undergo formal psychometric validation (e.g., factor analysis or internal consistency reliability testing). The instrument was developed through multidisciplinary expert review and external assessment to establish content validity and alignment with the study’s research questions, as it was designed to capture discrete experiential and demographic variables rather than latent constructs. Nevertheless, the absence of formal psychometric testing may limit assessment of construct reliability. Fifth, some subgroup analyses involved relatively small sample sizes, particularly within intersectional categories, which may increase statistical uncertainty and limit the stability of adjusted models. These findings should therefore be interpreted cautiously. This survey was conducted as part of a broader mixed-methods study that included semi-structured interviews with a subset of participants; those qualitative findings are reported separately due to word count limitations. Although the present analysis focuses on survey data, the larger study design allows for triangulation of themes across methodologies. Finally, because the sample included only current residents, the prevalence of disciplinary experiences may be underestimated, as individuals who had been dismissed from training were not captured.
Conclusion
Graduate medical education represents the final gateway to independent medical practice. In this national sample, Black residents, particularly those who were first-generation college graduates, experienced higher odds of disciplinary action and reported substantial concerns regarding racial influence and procedural fairness. These patterns suggest that disciplinary processes within GME warrant closer examination as potential sites of structural bias.
As stewards of public funding and the physician workforce, residency programs must ensure that evaluation and remediation processes are transparent, consistent, and equitable. Fairness in training is foundational to institutional integrity and to the development of a diverse, effective physician workforce.
Footnotes
Acknowledgments
The author is deeply grateful to the resident physicians who participated in this study and shared their experiences with honesty and courage; to the CIR for granting access to its resident physician members, which made this research possible; to Stacey Senat, MPH, Program Manager at Black Doc Village; to Laura Plantinga, PhD, for her statistical analyses; and to EVITARUS, the independent research firm that managed survey distribution and data logistics. Finally, the author acknowledges the contributions of our advisory committee members, including Naomi Nkinsi, MD, MPH; Khadijah Lane, MD; Monique Hedmann, MD, MPH; Adaira Landry, MD, MEd; Kimberly Ramseur, JD, MPH; and Karen A. Scott, MD, MPH, FACOG, whose insight and commitment helped shape every phase of this work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by the California Health Care Foundation (grant number: G-33407) and The Commonwealth Fund (grant number: 23-23804).
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.