
Abstract
Introduction:
Longstanding racial inequities in maternal mortality require tailored approaches to improving outcomes for Black birthing people. Doulas provide continuous emotional, physical, and informational support and have been shown to improve perinatal outcomes, particularly for Black birthing people. In response, some states have implemented Medicaid doula benefits. In January 2025, Pennsylvania—where ∼35% of births are Medicaid-covered—launched such a policy, allowing certified doulas to enroll as Medicaid providers.
Methods:
As part of a larger mixed-methods study on the effects of Medicaid policies on maternal and child health, the study team examined doulas’ experiences participating in Pennsylvania Medicaid. Semi-structured interviews were conducted with 30 doulas statewide from December 2023 to March 2025 to examine the policy’s implications for doulas and Black birthing people. Transcripts were analyzed using latent content analysis, applying inductive and deductive coding.
Results:
Doulas reported persistent racial inequities in health care, including delayed pain management and pressure on Black birthing people to accept unwanted interventions. They described advocating within a system marked by clinician bias and profit-driven hospital models. While some doulas viewed the Medicaid policy as improving credibility and expanding access for Medicaid recipients, concerns emerged regarding administrative burdens, credentialing, enrollment, and scale-up, especially for Black doulas, who play a central role in supporting Black birthing people.
Discussion:
This study highlights the need to support doulas in navigating Medicaid processes while also addressing structural barriers within the health care system. Insights from other states can inform implementation efforts in Pennsylvania.
Health Equity Implications:
These findings underscore that Medicaid doula policy must go beyond reimbursement alone to ensure that community doulas can connect with clients and provide continuous, holistic support both within and outside the health care system—unencumbered by credentialing requirements, enrollment barriers, or payment structures that constrain the scope and reach of their work. Reimagining such policy to center the experiences of both Black doulas and Black birthing people is a necessary step toward dismantling the systemic conditions that drive racial inequities in maternal mortality.
Introduction
There are longstanding racial inequities in maternal and infant mortality and morbidity in the United States.1–3 Black birthing people are three times more likely to experience maternal mortality than White birthing people, with most deaths being preventable.2–4 (Language note: “birthing people” is meant to include all genders with the ability to give birth.) Perinatal inequities are driven by complex factors, including structural oppression and inequitable health care, social, and economic systems. 5 The perinatal period generally refers to the time including pregnancy and the postpartum phase (often up to 1 year after birth). 6 Structural factors that influence social determinants of health include access to quality health care, safe housing, healthy food, and community support, all of which are linked to perinatal outcomes.5,7–13
In 2003, the Institute of Medicine published a report that set a precedent for future studies to examine prevalence, diagnosis, and treatment of disease regarding racial and ethnic minority groups and provided guidance regarding how these disparities must be addressed. 14 This report highlighted examples of harmful stereotypes, microaggressions, and medical racism, including documenting clinician beliefs around Black people having a higher pain tolerances and reports that doctors disproportionately dismiss Black patients’ needs. 14 Systematic oppression and racism lead to mistreatment by clinicians within health care settings. 15 For example, a 2016 study reported that 41% of first- and second-year medical students believed that Black people have thicker skin than White people. 16 The findings of this report remain relevant today, reflecting persistent medical racism and violence perpetrated against Black birthing people within obstetrics and gynecology.17,18
Previous literature notes an association between respectful, attuned care and improved health outcomes and equity, with evidence showing that when birthing people are supported and heard during labor and delivery, they experience more positive birth outcomes.19–22 Doula support, which provides continuous emotional, physical, and informational care throughout the perinatal period, is associated with improved birth experiences and outcomes.23–29 Evidence indicates that doula care increases vaginal birth rates and reduces rates of preterm birth, low birth weight, and postpartum depression and anxiety. 30 Doulas also support health care navigation and facilitate open communication between birthing people and clinicians. However, studies report that clinicians often underestimate doulas’ essential emotional support and perceive them as lacking clinical training. 31
Specific interventions, approaches, and research that center the lived experiences and voices of Black birthing people are critical to addressing perinatal inequities.32,33 Doula care can be tailored to center the unique needs of birthing people who have historically been excluded from equitable health care.34,35 To promote the advancement of positive maternal and child health (MCH) outcomes in the United States for low-income communities, 24 states, including California, Florida, Minnesota, and New Mexico, have implemented policies to reimburse doulas through Medicaid.36–39 Medicaid covers a large percentage of births in the United States every year. As of 2023, Medicaid covered over 50% of births in 4 states, 42–49% in 18 states, 35–41% in 18 states, and fewer than 35% in 10 states. 40 To date, 21 states cover doula services through Medicaid, with several states working to implement similar policies.38,41–44
In Pennsylvania, ∼35% of births are covered by Medicaid. 45 In February 2024, Pennsylvania doulas began negotiating reimbursement rates with each managed care organization (MCO), allowing payment to state-certified perinatal doulas.36,46 Beginning January 1, 2025, Pennsylvania Medicaid, also known as the Medical Assistance (MA) Program, required coverage of doula services for its beneficiaries, allowing certified doulas to enroll in the MA Program and serve MA beneficiaries in both fee-for-service and managed care systems. 47
The Pennsylvania Doula Commission (PADC), a nonprofit advocacy group, was formed to ensure equitable processes when developing and implementing the Medicaid doula reimbursement policy. PADC worked with our study team to provide scholarships to doulas to offset certification costs and to develop an educational toolkit. 48
Few studies examining the effects of Medicaid reimbursement for doula care on health outcomes among Black birthing people and Medicaid populations have centered the voices of doulas.49,50 Drawing on Dr. Camara Jones’ definition of health equity as “the assurance of the conditions for optimal health for all people,” this article examines racial health equity as operationalized through doulas’ experiences navigating Medicaid policy and the constraints and opportunities it creates. Specifically, we explore how these experiences shape doulas’ capacity to support Black birthing people in accessing equitable, high-quality perinatal care. 51 We describe Pennsylvania doulas’ experiences serving birthing people, particularly Black individuals, and their perspectives on the effects of the Medicaid doula benefit on racial health equity.
Methods
As part of a larger mixed-methods study focused on Medicaid policy and MCH outcomes, the research team conducted semi-structured interviews on Zoom with doulas across Pennsylvania between December 2023 and March 2025. 52 The University of Pittsburgh Human Research Ethics Board approved this work under STUDY21080072.
We developed a semi-structured interview guide to learn about: (1) doulas’ backgrounds and experiences, (2) medical racism and birthing people’s and their families’ experiences within the health care systems, (3) doulas’ impressions of the Medicaid policy and its impact on their practice, and (4) implications of the Medicaid policy for population health. The guide was structured to ascertain how the doulas’ identities and experiences informed their perspectives on the policy (see Supplementary Data). Domain titles in the interview guide (e.g., “medical racism”) were used as analytic labels rather than participants’ own language. Questions explored participants’ observations of racism and inequitable treatment across the health care system, including among clinicians, nursing staff, and institutional practices, in relation to racial health equity. Interviews that were conducted after January 2025, when the policy was fully implemented, included questions about the policy as current rather than forthcoming. The two doulas interviewed after that date had not yet enrolled as Medicaid providers.
Participant recruitment and selection
Doulas who had provided pregnancy or postpartum care within the state of Pennsylvania in the last year were recruited in partnership with the PADC via word-of-mouth, social media, and paper flyers shared at Healthy Start, Inc.-sponsored activities; and electronically via email to organizations across the state of Pennsylvania, doula agencies, and county health agencies. Snowball sampling was used to recruit additional participants. The QR code on the flyers led interested participants to an intake form that collected their name, phone number, email address, and general availability for an interview. Doula participants received $50 in compensation.
Positionality statement
The research team included community health workers and public health professionals with master’s-, bachelor’s-, and doctoral-level training, most of whom identified as women, with one coauthor identifying as genderfluid. Several team members have direct experience in doula or community-based perinatal care, bringing experiential knowledge to the study design and analysis.
The primary authors responsible for study design, qualitative methodology, and analysis are a team of doctoral-prepared public health researchers, five of whom are birthing people themselves (A.D.C., M.J., C.M., C.L.S., and D.D.M.). Two are Black women whose scholarship is grounded in Black feminist theory, reproductive justice, and the intersectional experiences of Black women (D.D.M. and C.M.). One is a Hispanic woman with extensive experience in community-engaged maternal health research (A.D.C.). Three are White women whose research focuses on Medicaid policy (M.J.), community-based perinatal care, including direct prior experience leading a community-based doula program (C.L.S.), and strategies to expand access to midwifery and community birth (S.A.S.).
Interviews were conducted by 14 team members, including six Black women and eight White women, with at least one Black interviewer present in 28 of 30 interviews. Community health workers received qualitative interview training prior to participation. The intentional inclusion of Black interviewers—who share key characteristics with the majority of study participants—was central to establishing trust and creating conditions for open dialogue, particularly around experiences of racial bias and inequitable care, which strengthens the trustworthiness of the analysis.
Throughout the research process, the team engaged in ongoing reflection—informed by Black feminist theory and reproductive justice frameworks—regarding how their racial identities, professional backgrounds, and lived experiences might shape interpretation of both Black and White doulas’ experiences, and we incorporated this reflexivity into our analytic process.
Analytic approach
Interview audio recordings were transcribed verbatim via Transcribe Me!, a professional transcription service. 53 Ten coders, faculty or staff who also interviewed participants, used latent content analysis to deductively code doulas’ professional backgrounds and their reactions to the Medicaid policy, and to inductively analyze how doulas’ personal and/or witnessed experiences with structural racism impacted their professional approaches and opinions regarding the policy. Latent content analysis is an immersive form of analysis intended to interpret the deeper meaning of the text.54,55 Transcripts were coded using NVivo 14 software. 56 Eight transcripts were coded twice to assess intercoder reliability. Differences were resolved through discussion among the interviewers and coding team. The Consolidated Criteria for Reporting Qualitative Research framework guided the reporting of the results (see Appendix). 57
Results
Participant descriptive data
Thirty-four eligible doulas expressed interest in being interviewed, and 30 completed interviews lasting ∼60 min each. Figure 1 shows the MCO regions across Pennsylvania, with pins representing the counties served by doulas. Fifteen doulas served more than one county. The majority (14) of the doulas interviewed served the southeast region of the state, including Philadelphia, while eight doulas served in the southwestern region. The remaining eight doulas served the northwest and central regions of the state.

Overlay of MCO regions on Pennsylvania counties. (Pin indicates number of doulas stating that they served that county.) MCO, managed care organization.
Table 1 shows the demographics of the doulas interviewed, as well as details of their practice. Approximately half of the participants were between ages 25 and 35 (n = 14, 46.7%), while 53.3% were 35 years or older. Most doulas were Black (n = 17, 56.7%). More than half of doulas (n = 17, 56.7%) attended nine or fewer births per year. Most doulas were certified by their training organizations (n = 22, 73.3%), with two stating they were certified through the state of Pennsylvania. Half of the doulas (n = 15, 50%) practiced in a combination of private, community, and other settings, including contracted roles with doula agencies or as leaders of doula organizations. Participants’ experience ranged from <1 year to 27 years, although most were relatively new to the profession, with a median of 3 years of experience.
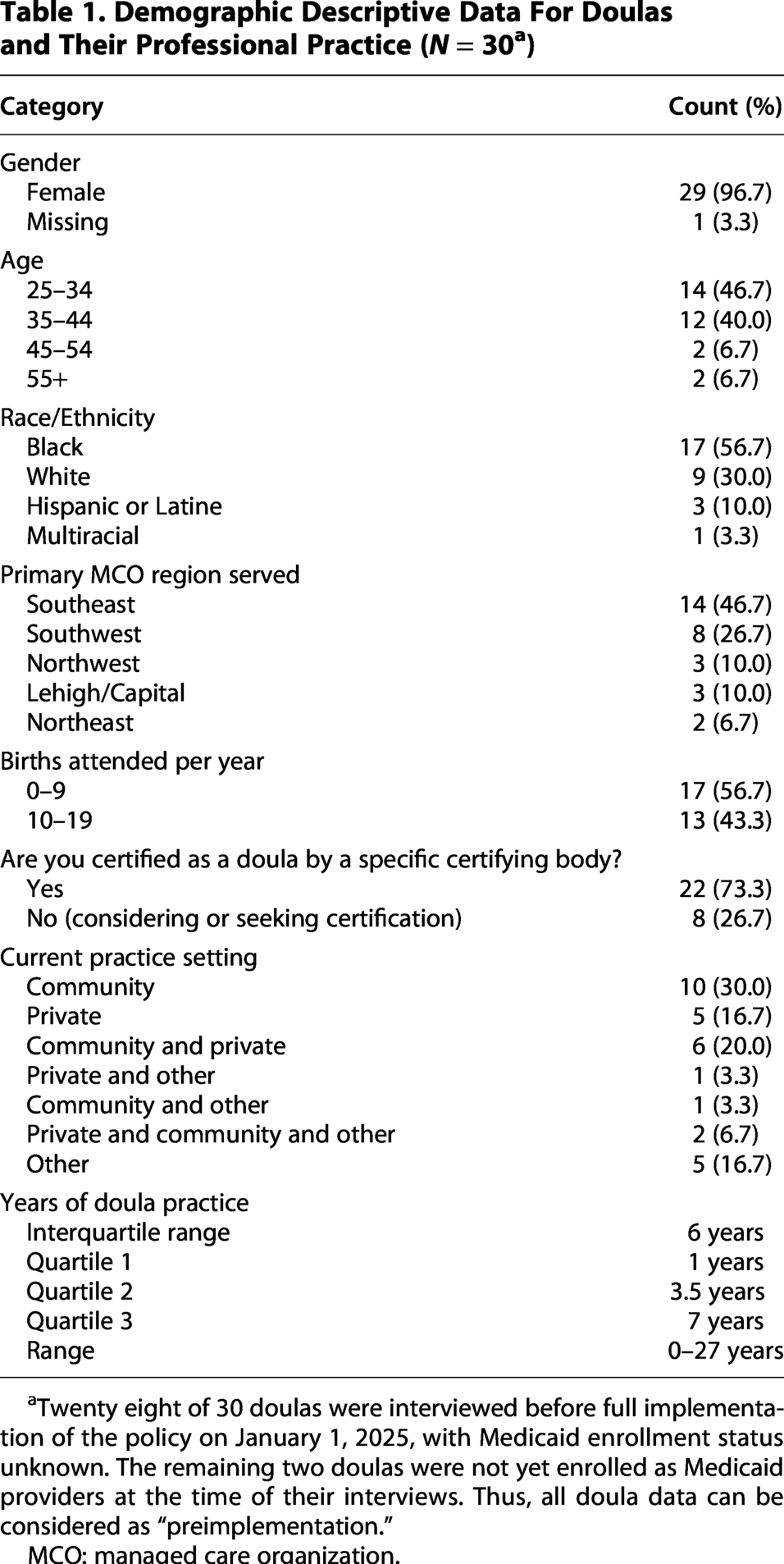
Twenty eight of 30 doulas were interviewed before full implementation of the policy on January 1, 2025, with Medicaid enrollment status unknown. The remaining two doulas were not yet enrolled as Medicaid providers at the time of their interviews. Thus, all doula data can be considered as “preimplementation.”
MCO: managed care organization.
During the interviews, doulas described the populations they served, including individuals from various racial/ethnic groups, income levels, and age groups, as well as people in military families, individuals recovering from opioid addiction, and those involved in the carceral system (Table 2).
Populations Served by Doulas
Consolidated Criteria for Reporting Qualitative Research Checklist
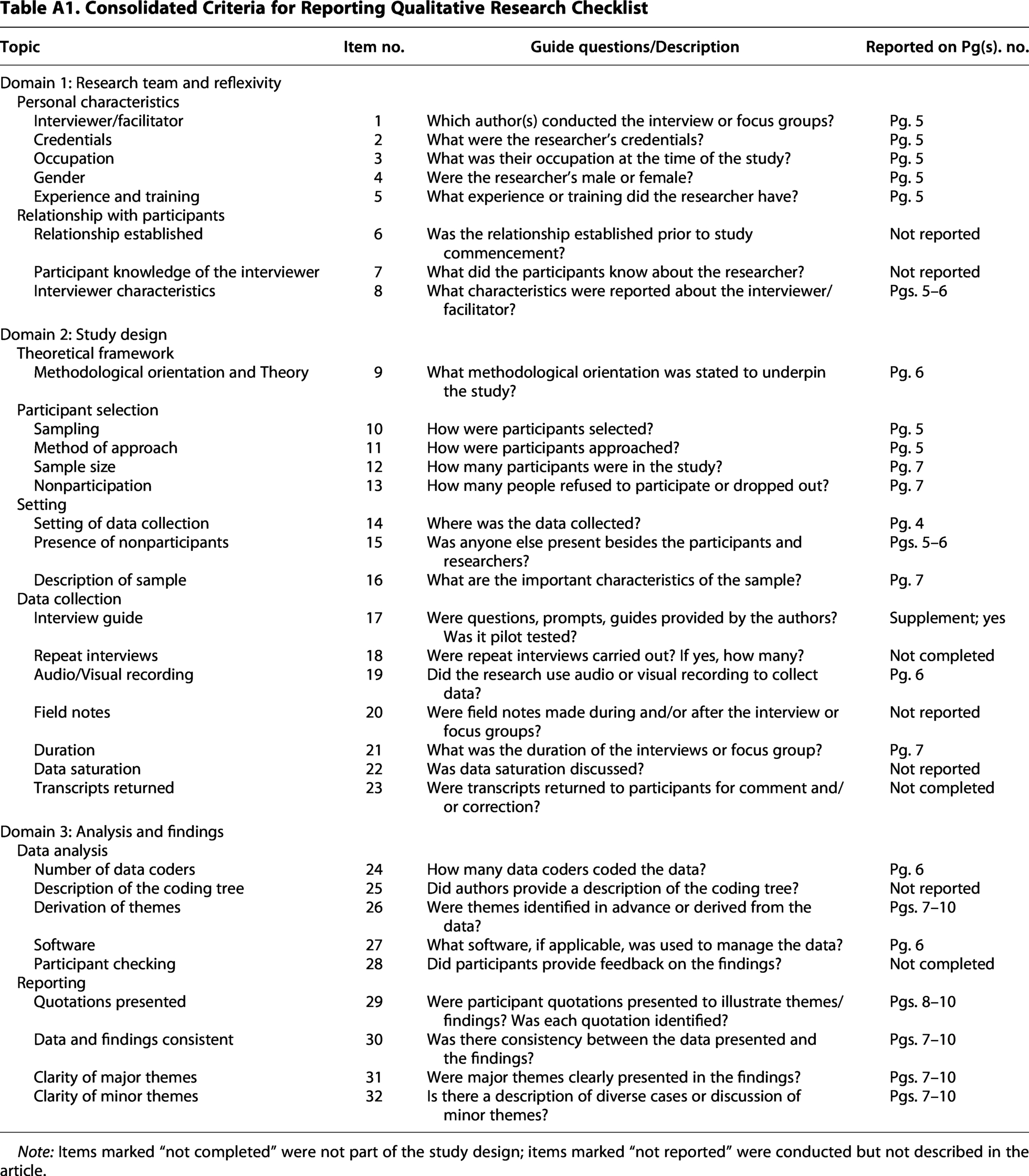
Note: Items marked “not completed” were not part of the study design; items marked “not reported” were conducted but not described in the article.
Qualitative data
Pennsylvania doulas’ comments about their experiences, particularly in serving Black birthing people, and their perspectives on how the new state Medicaid benefit covering doula services will affect racial health equity focused on three major themes:
Theme 1: How doulas create systemic change for racial justice for birthing people in the context of Medicaid populations.
Theme 2: Limitations in their ability to address inequitable care.
Theme 3: Leading up to full implementation of the policy on January 1, 2025, doulas’ perspectives on the barriers and facilitators presented by the Medicaid policy for birthing people and for their work as doulas.
Theme 1: What doulas can do to advance racial justice
Doulas see themselves as part of—but not the entire—solution to advancing racial justice for Black birthing people. First, in their professional approach, many Black doulas can empathize with Black birthing people’s experiences of racial injustice because they or their loved ones have also experienced it. For some, “being a birthing person and feeling discriminated against” was the “main reason” they became doulas [Doula 1].
Others viewed their role as being the person they wished had been there to advocate for them during their own birth experience—someone who could have prevented the mistreatment they faced—so that others might avoid similar suffering. “[There is an assumption] that always black women are strong…we can tolerate different pain levels. And I…experienced that. And that’s another reason why I wanted to become a doula… the one nurse never came back with my pain medication…I tell my clients, I often see a lot with us, the Black women, they’ll stay in pain for a while. And I’m like, ‘Are you in pain?’ They’re like, ‘Yeah, yeah.’ And I’m like, ‘Well, if you’re in pain, let your nurse know. Don’t just suffer.’” [Doula 2] “I do know racism is real, but I also believe that you can influence people and influence scenarios, even if it’s just for that moment. So…you might not be able to change the belief system of the service provider, but you can change the experience that…birthing person has with that provider.” [Doula 3]
These statements demonstrate how doulas can influence Black birthing people’s perceptions of safety and comfort and help mitigate clinicians’ racial biases.
Theme 2: Limitations to what doulas can do about inequitable care
Factors that may limit the overall impact of doulas on health outcomes include biases among health care providers and the profit-driven priorities of hospital systems, which can lead providers to overlook patients’ preferences in order to expedite labor.
Doulas described experiencing opposition from providers whose professional biases led them to misunderstand the doula’s role: “They’re…hesitant only because we’re not a part of a hospital family. We are our own entity and…we’re coming into the hospital. So sometimes we get rejection. Sometimes we get people like, ‘You’re not allowed in the [operating room].’…we get the pushback from the hospitals.” [Doula 4]
Racial bias among providers can also limit doulas’ ability to do their jobs. “Black doulas are constantly met with, ‘Is that your cousin, your sister, your aunt?’, not in a respect of us being a professional in that space or an expert in our profession.” [Doula 5]
Additionally, doulas observed that client characteristics such as race or income impacted the likelihood of receiving medical interventions intended to hasten active labor progress, regardless of client preferences. “…clients from a certain demographic, especially Black or Hispanic from low-income communities who are on Medicaid or don’t have private insurance, essentially, or good private insurance get treated very differently than other clients have. I’ve seen how they’ve rushed people, how they have not used a lot of informed consent when treating clients…I see a lot of pushes for epidurals with clients, very forceful pushes, especially for my Black clients.” [Doula 6]
Such biases toward patients, juxtaposed with biases toward doulas, can lead to disempowerment of the doula to advocate when a client’s pain is ignored or when the doctor is pushing the birthing person to deviate from their birth plan.
Additionally, because doulas cannot change the profit-driven priorities of hospitals, which shape how clinicians manage births, these systemic pressures compound the racial biases already present in maternal care. “I feel like no matter what the race is, many times hospitals are to benefit themselves.…as a business, not nurturing a mother as she has a child…[I]f they need a procedure done or the woman wants to have a natural birth, but it’s just going a little bit too slow and the hospital’s busy, they start Pitocin or they’ll do something to speed things along.” [Doula 7]
Theme 3: Facilitators and barriers presented to birthing people and doulas by the new Medicaid policy
When asked about the positive changes the Medicaid policy could facilitate, doulas felt encouraged that the Medicaid policy could lead hospitals to better recognize them as part of their clients’ care teams, making it easier for them to support the families they serve. “Even though I know I’m allowed in the [operating room] with my [client], we get…pushback from the hospitals. And I think that…with this policy coming into play, we won’t get that pushback anymore…with…us getting that recommendation and us being there, it’ll…help me and my job will be a little bit easier when I’m coming into the hospital… Other than just my certificate and my experience, we got the whole government backing us up now.” [Doula 4]
By extension, a more supportive context would also benefit the birthing person. Additionally, the policy could enable more Black birthing people to access doula care. “I think it will help…I don’t think the end-all-be-all, but I don’t think it’ll hurt…I…think that more Brown clients will be served by doulas with the reimbursement. Because …if you’re unable to afford it, you might not…get the doula care that you need….” [Doula 8]
Conversely, doulas expressed concern that the policy could limit doulas desiring to enroll as Medicaid providers from doing so. “Who are we targeting in terms of this certification process? How are we credentialing people? Are we really making efforts to credential Black doulas to really have access to the resources to be able to be reimbursed through Medicaid coverage?” [Doula 9]
This response highlights the need to support Black doulas pursuing credentials and/or registration as Medicaid providers to prevent disparities in who can participate. Credentialing and billing processes can be confusing, and doulas, who are also often business owners, would take on additional, time-consuming administrative tasks.
Furthermore, increased demand for doulas among Medicaid recipients might necessitate that doula agencies would need to expand their teams to address the growing need for doula support, an expansion that might require time that lags behind the demand. “…my company…just switched over to everybody being full spectrum doulas…[I]f they were to do the Medicaid and all these women are afforded doulas, we would need a bigger doula program. We would need way more doulas than just the 5 or 6 that we…have …We would need…10 or 20….I think that would be, I guess, a good issue to have.” [Doula 4]
Discussion
Doulas interviewed described a range of experiences in their practice as advocates for birthing people navigating complex, often inequitable medical systems. Many observed persistent racial inequities in care, especially among Black birthing people, who were often pressured into labor-accelerating medical interventions and frequently endured prolonged, unnecessary pain due to clinicians delaying or denying medications. These findings echo previous research documenting systemic bias and structural racism in maternal health care, which continue to contribute to poorer outcomes for Black birthing people.1,2,49,50,58
Doulas prioritized helping birthing people advocate for themselves to improve their birth experiences and outcomes; however, their efforts were often constrained by clinician bias and hospital business models that prioritized efficiency over individualized care. This reflects broader research showing how institutional priorities and implicit biases can undermine equitable treatment.30,31,49,59 Black doulas, especially, draw on lived experience to promote autonomy for Black clients, yet they must do so within health care systems that constrain their efforts.
Ahead of Pennsylvania Medicaid doula benefit implementation, doulas expressed optimism and concern. Some believed the policy could enhance professional credibility and expand culturally concordant care, especially for Black birthing people. Others noted credentialing, enrollment, billing, and upscaling capacity challenges—issues documented in similar efforts in other states.36,43,44 In response, the Pennsylvania’s Doula Commission partnered with researchers to create a doula toolkit to support Medicaid system navigation. 48 Similar initiatives, including technical assistance hubs, have been launched in states such as California, Florida, and New Jersey.38,41
Importantly, the barriers doulas described reveal a systemic disconnect: health care systems often recruit doulas to address disparities they did not create. Expecting doulas to resolve entrenched inequities without institutional change is unrealistic and risks blaming doulas if outcomes fall short; however, the policy holds potential to improve outcomes, reflecting articulated policy goals.50,59
The study has several strengths. The interviews captured the expertise of doulas across Pennsylvania, whose insights helped shape early policy implementation, including a statewide survey and doula toolkit. 48 The research team included members of impacted communities and practicing doulas, enhancing study relevance. One limitation was the low representation from northeastern Pennsylvania due to the smaller number of practicing doulas in that region at the time of recruitment, resulting in fewer eligible participants and lower regional representation in the sample.58,60–62 Future research should prioritize rural areas and include clinician perspectives that deepen understanding of care disparities.
In summary, doulas serve as critical advocates amid systemic inequities in maternal care. Medicaid coverage offers a promising path toward improved outcomes, but its lasting impact depends on removing institutional barriers and ensuring ongoing support for doulas.
Implications for perinatal health equity
Imagine a perinatal care landscape in which every pregnant person receives respectful, continuous support from trusted, knowledgeable care workers embedded in their own communities, and in which the health system is readily available when needed rather than serving as the default setting for all care. In this reimagined system, doulas are not a supplemental service navigating a broken infrastructure but essential members of a health-focused care ecosystem—one organized around positive health outcomes rather than process measures or budget constraints. Doulas would have the time, training, and cultural proximity to meet the specific needs of each birthing person, and the health system would function as a partner rather than a barrier.
Doulas can support pregnant and birthing people within health systems that often fail to meet their needs, but evidence shows that doula care alone will not eliminate structural inequities. 36 Reimagining Medicaid doula policy means moving beyond benefit design as a technical exercise toward a transformative framework co-created with community doulas—particularly Black doulas—who hold both the expertise and the lived proximity to define what equitable perinatal care requires. This means moving beyond reimbursement alone to ensure that community doulas can connect with clients and provide continuous, holistic support both within and outside the health system—unencumbered by credentialing requirements, enrollment barriers, or payment structures that constrain the scope and reach of their work. States that have centered community doulas in benefit design offer an early blueprint. 36 If these lessons were applied more widely, a reimagined model would treat doula care not as a supplemental service but as a structural intervention—one that realigns perinatal care around the needs and wisdom of birthing people themselves and measures success by whether racial gaps in maternal and infant health outcomes are meaningfully reduced. 37
Authors’ Contributions
A.D.C.: Conceptualization, data curation, formal analysis, investigation, methodology, software, validation, visualization, and writing—original draft and review and editing. A.K.: Investigation, validation, and writing—original draft and review and editing. I.R.O.: Visualization and writing—original draft and review and editing. M.J.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, resources, supervision, and writing—review and editing. E.M.: Conceptualization, validation, and writing—review and editing. C.M. and C.L.S.: Conceptualization, data curation, formal analysis, investigation, methodology, software, and writing—review and editing. L.A. and M.S.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, and writing—review and editing. C.L.: Conceptualization, data curation, formal analysis, investigation, methodology, software, visualization, and writing—review and editing. H.D.: Writing—review and editing. S.S.: Conceptualization, data curation, formal analysis, investigation, methodology, and writing—review and editing. E.L.: Project administration and writing—review and editing. S.A.S.: Conceptualization, data curation, formal analysis, investigation, and methodology. D.D.M.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, resources, supervision, and writing—review and editing.
Footnotes
Acknowledgments
The authors thank our community partners, Healthy Start Pittsburgh, Inc. (HSI), the HSI Community Health Advocates, the Pennsylvania Doula Commission, and Kiana Hacker for their valuable contributions to interview guide development and data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by a grant from the
Supplemental Material
Appendix
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.