
Abstract
Purpose:
To describe circumscribed choroidal hemangioma (CCH) management in the era of intravitreal anti-vascular endothelial growth factor.
Methods:
Retrospective chart review of 11 patients (4 men and 7 women; mean age: 47 years) who were treated at University of Wisconsin for CCH between January 1, 2009 and June 1, 2015, using photodynamic therapy (PDT), intravitreal bevacizumab, or a combination of both PDT and bevacizumab. We define change in visual acuity with each treatment as change in Snellen visual acuity from the day of treatment compared to the follow-up appointment closest to the 3-month posttreatment time point. We report visual acuity score (VAS) by converting Snellen visual acuity using the formula, VAS = 100 − 50 × logarithm of the minimum angle of resolution.
Results:
We treated 7 eyes with PDT only, 1 eye with bevacizumab only, and 4 eyes with combined PDT and bevacizumab. In the PDT-only group, visual acuity improved in 4 eyes, stabilized in 2 eyes, and worsened in 1 eye (average +7.8 letters by VAS). In the 1 eye treated with bevacizumab alone, visual acuity improved by 2.6 letters by VAS. In the combined group, visual acuity improved in 3 eyes and stabilized in 1 eye (average +6.2 letters by VAS).
Conclusion:
Our study supports the effectiveness and safety of PDT as a primary treatment modality. In addition, our study suggests the independent efficacy of bevacizumab monotherapy in select patients, the synergistic response to bevacizumab with repeated PDT, and potentially reduction of PDT treatments by adding bevacizumab to the treatment protocol.
Keywords
Introduction
Circumscribed choroidal hemangiomas (CCHs) are rare, solitary vascular hamartomas of the choroid with characteristic diffuse hyperfluorescence on fluorescein angiography and high reflectivity on ultrasound (Figure 1A and B). 1 Vision loss from CCH is primarily caused by subretinal fluid exudation from the tumor (Figure 1F). 1 Treatment modalities, including laser photocoagulation, radiation therapy, and transpupillary thermotherapy, have focused on obliteration of the tumor. 2 Long-term visual outcomes from these therapies have been poor due to adverse side effects and tissue damage from their administration. 1 –5
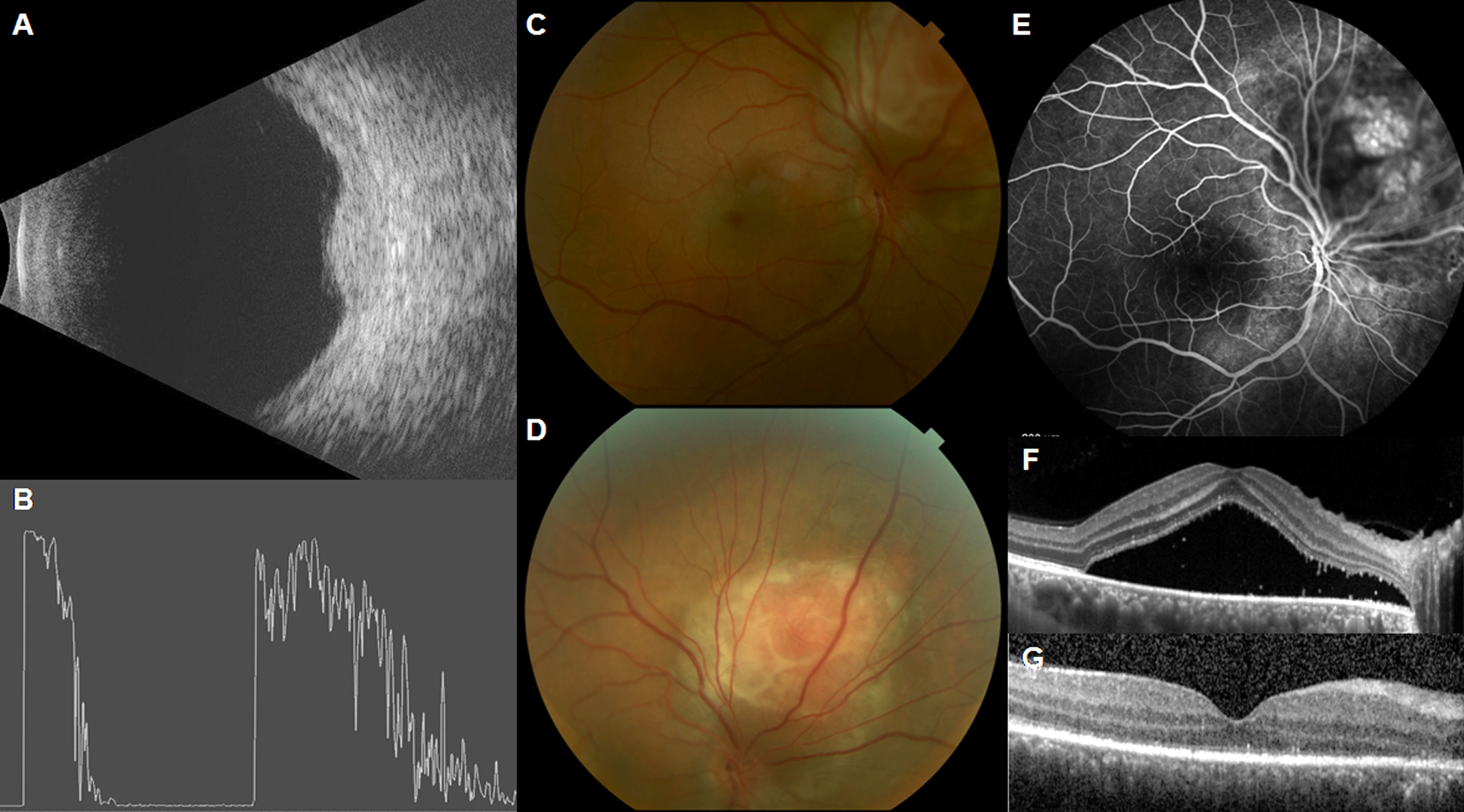
A 40-year-old man with a history of choroidal hemangioma in the right eye status posttreatment with intravitreal bevacizumab and photodynamic therapy presents with decreased vision in the right eye. Ultrasonography demonstrates the presence of a choroidal mass (A) with low internal reflectivity (B). Funduscopic examination reveals a large orange-red choroidal lesion superior nasal to the optic disc with fluid tracking to the macula (C and D). Fluorescein angiography shows hyperfluorescence and leakage nasal to the optic disc (E). Macula optical coherence tomography shows recurrent subretinal fluid (F). The patient was treated with 9 intravitreal bevacizumab injections and 4 sessions of photodynamic therapy with resolution of subretinal fluid (G).
Recent evidence has strongly supported photodynamic therapy (PDT) as first-line treatment for exudative detachments from CCH with multiple case series reporting tumor regression and visual improvement or stabilization. 5 –11 However, there remain cases where CCH may become refractory to PDT or repeated PDT treatments may risk chorioretinal ischemia; this is especially concerning if the treatment area involves the macula or the optic nerve. In an era where anti-vascular endothelial growth factor (VEGF) has shown broad efficacy in resolving macular edema associated with a multitude of etiologies, this case series explores anti-VEGF therapy in comparison to and in combination with PDT.
Methods
Institutional review board/ethics committee approval was obtained. The study protocol and the investigators were Health Insurance Portability and Accountability Act–compliant and adhered to the tenets of the Declaration of Helsinki.
Patients of University of Wisconsin Department of Ophthalmology and Visual Sciences were searched. Inclusion criteria were International Classification of Diseases, Ninth Revision, code for choroidal or retinal hemangioma (228.09 and 228.03), loss of vision due to subretinal fluid exudation, treatment at University of Wisconsin Department of Ophthalmology and Visual Sciences between January 1, 2009 and June 1, 2015, availability of visual acuity at time of treatment and 3 months posttreatment for all treatments. Exclusion criteria were any diagnosis outside of CCH and lack of treatment with PDT or intravitreal bevacizumab. A total of 11 patients (4 men and 7 women; mean age: 47 years, 21-85 years old at initial diagnosis) met the inclusion and exclusion criteria. We retrospectively reviewed the medical records of these 11 patients (12 eyes). The chart review extended retrospectively to any prior visits and management of these same patients. Some records were unable to be reviewed in their entirety from diagnosis due to discontinuity of care.
The primary end point was change in visual acuity from treatment time to 3-month follow-up (mean: 98.4 days). For patients receiving multiple treatments, the average change in visual acuity at 3 months after each treatment was reported. All visual acuity was measured as Snellen visual acuity, which was converted into visual acuity score (VAS), the equivalent of Early Treatment Diabetic Retinopathy Study letters, using the formula: VAS = 100 − 50 × logarithm of the minimum angle of resolution.
Results
Of the 11 patients (12 eyes) included in this study, 9 patients (10 eyes) have contiguous records dating back to their initial diagnosis and treatment. Two patients (2 eyes) were diagnosed and treated prior to their establishment of care with the University of Wisconsin Department of Ophthalmology and Visual Sciences. The oldest medical record reviewed is from 1993, and the average total follow-up time was 87.5 months (7.3 years).
The eyes with CCH were treated with PDT, intravitreal bevacizumab, or a combination of both PDT and bevacizumab. Specifically, 7 eyes received PDT only, 1 eye received bevacizumab only, and 4 eyes received combined PDT and bevacizumab. In the PDT-only group, visual acuity improved in 4 eyes, stabilized in 2 eyes, and worsened in 1 eye (overall average +7.8 letters by VAS). In the 1 eye treated with bevacizumab alone, visual acuity improved by 2.6 letters by VAS. In the combined group, visual acuity improved in 3 eyes and stabilized in 1 eye (average +6.2 letters by VAS). These average visual acuity changes are plotted in Figure 2 revealing a relatively large case-by-case variability in treatment response.
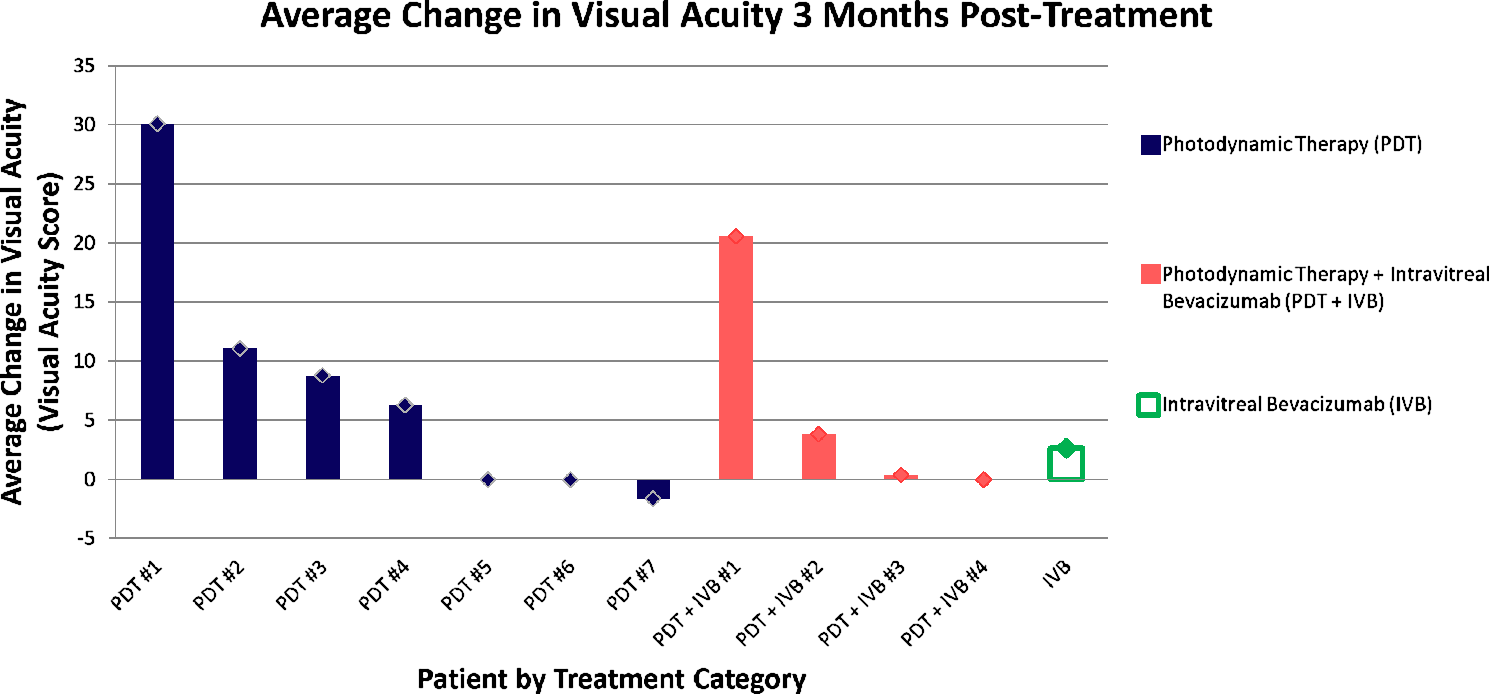
Each patient’s change in visual acuity from treatment date to approximately 3 months after treatment is shown here (averaged across all treatments received). Photodynamic therapy (PDT) is shown in blue, combined photodynamic therapy + intravitreal bevacizumab (IVB) is shown in red, and intravitreal bevacizumab only (IVB) is shown in green. There is significant variability across patients, but overall visual acuity either improved or remained stable across all groups.
Chronological treatment responses in 2 patients who received combined PDT + bevacizumab are highlighted (Figures 3 and 4). In these plots, the combined marker (green triangle) indicates simultaneous treatment with PDT + bevacizumab. The patient in Figure 3 requires increasingly frequent PDT treatments for recurrent exudation over a 5-year period. By the eighth PDT session, the patient’s vision has a significant decline but is able to recover with a change to adjuvant bevacizumab treatment. This patient demonstrates both the potential of multiple PDT sessions targeting the same lesion and the efficacy of bevacizumab to synergize and supplement the role of PDT in visual recovery. The patient in Figure 4 is a contrasting case where adjuvant bevacizumab is used early to successfully stabilize vision instead of utilizing repeated PDT. There is a 3-year period during which bevacizumab is used for recurrences, while the patient is spared PDT. Interestingly, though there is a decline in response to bevacizumab therapy alone, subsequent combination of PDT simultaneously with bevacizumab yields visual recovery. These 2 cases indicate a synergy in the combination of PDT and bevacizumab.
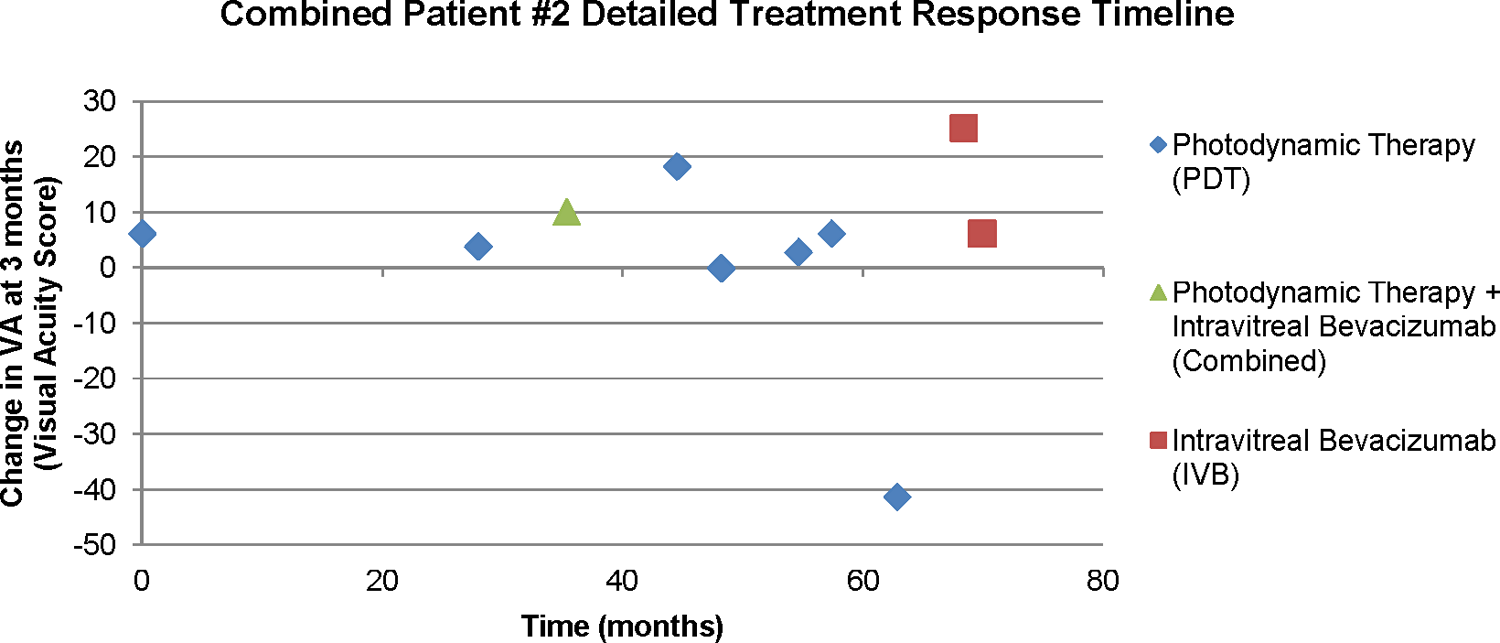
After increasingly frequent photodynamic (PDT) for recurrent exudation over a 5-year period, the eighth PDT results in loss of visual acuity, but is able to recover with a change to adjuvant intravitreal bevacizumab (IVB) treatment. This patient demonstrates both the potential for large numbers of PDT sessions targeting the same lesion and the efficacy of bevacizumab to synergize and supplement PDT’s role in visual recovery.
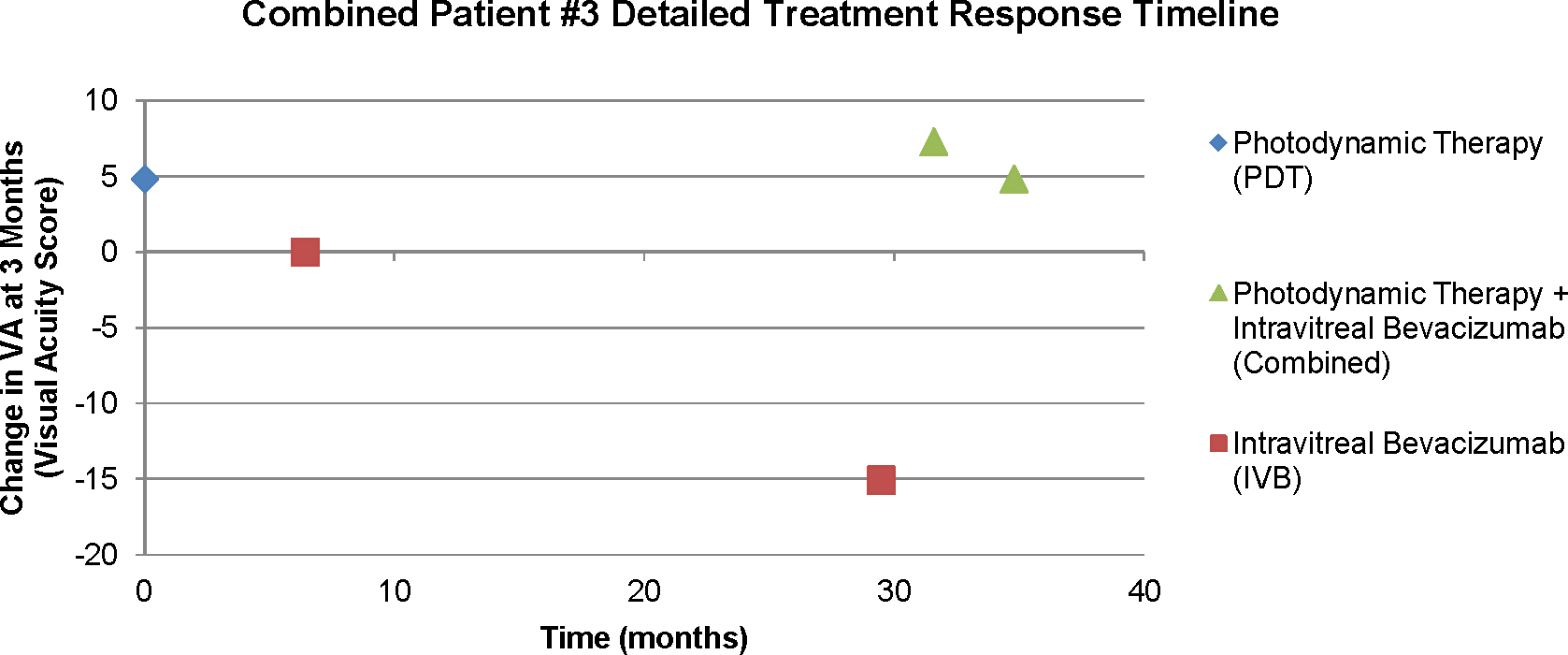
After initial treatment with photodynamic therapy (PDT), adjuvant intravitreal bevacizumab (IVB) is used early to successfully stabilize vision instead of utilizing repeated PDT. There is a 3-year period during which bevacizumab is used for recurrence, but the patient is spared PDT. Interestingly, although there is a decline in response to bevacizumab therapy alone, subsequent combination of PDT simultaneously with bevacizumab yields visual recovery.
Conclusion
The CCH represents a benign vascular hamartoma, with a risk of chronic exudation and severe vision loss. 1 Vision loss occurs through multiple mechanisms, including active exudation, distortion of normal chorioretinal anatomy, and development of associated choroidal neovascular membranes. 1
The PDT with visudyne (Valeant Pharmaceuticals North America LLC; Bridgewater, New Jersey) works by inducing vaso-occlusion of choroidal vessels upon exposure to a laser light beam. 12 Side effects include transient increased exudation, 13 chorioretinal atrophy, 14 chest pain/shortness of breath/syncope, 15 and anaphylactic reaction. 16
In recent years, full-fluence PDT has become the gold standard for the management of CCH. 5 –11 In keeping with this observation, 11 of 12 eyes in this study received PDT without any side effects.
As demonstrated by our series, the use of anti-VEGF can have a synergistic effect in reducing macular edema associated with actively exudative CCH. We hypothesize that the role of anti-VEGF in the management of CCH is multifactorial.
First, it has been shown that there is a transient rise in VEGF levels following PDT. 17 This is thought to be the major mechanism responsible for the transient decline in vision following PDT. Consequently, 1 rationale for anti-VEGF use in CCH is to prevent the visual decline associated with the rising VEGF levels posttreatment. Given the half-life of bevacizumab (4.32 days) 18 and the persistent elevation of VEGF post-PDT for up to 3 months posttreatment, 17 administration of an injection of bevacizumab at the time of treatment or immediately following it has the potential to decrease the VEGF load.
The peripapillary predilection of CCH (38%) has been previously shown. 6 Because of the occlusive nature of the PDT, there is a high risk of vascular damage to the optic nerve when treating lesions close to the optic nerve. In fact, tumors that are abutting the nerve (Figure 1C and D) cannot be fully treated as it is contraindicated for the laser beam to come into contact with the border of the optic nerve. Consequently, a second role for adjuvant anti-VEGF therapy may be to reduce the treatment burden of PDT and, more importantly, minimize the risk of inadvertent, PDT-induced damage to the optic nerve.
Furthermore, the efficacy of PDT can be limited by multiple variables, including media opacities, overlying hemorrhage, or active tumor exudation. Therefore, a third role for the use of anti-VEGF prior to PDT is to debulk exuberant exudation and increase the efficacy of PDT by allowing the laser beam to better focus and penetrate into the deeper choroid, resulting in enhanced effectiveness.
Finally, although rare, choroidal neovascularization in association with CCH is reported as a potential consequence of subtle inflammation and/or chronic ischemia. 19,20 Adding VEGF blockers to PDT can theoretically inhibit or limit the development of such membranes and their associated exudation, and Querques reports successful treatment of such a case with intravitreal ranibizumab, another anti-VEGF agent. 20
In our experience, when using bevacizumab for CCH, monthly follow-up in the acute phase of exudation is recommended for possible repeated bevacizumab treatment until resolution or stabilization, similar to other VEGF-mediated diseases (age-related macular degeneration, vein occlusions) managed with intravitreal agents. Once fluid resolution or a stable state is achieved, follow-up may be lengthened to 3 months, 6 months, and then yearly, provided the exudation remains quiescent. The guidelines for follow-up after PDT are less clear, although most studies describe follow-up at 1 month, 3 months, 6 months, and 12 months. 21 Extrapolating from the age-related macular degeneration literature on PDT, the choroidal vascular occlusive effects seen with treatment may take up to 12 weeks to fully become apparent. 14 In the case of recalcitrant or previously treated lesions, we recommend a more conservative initial follow-up of 6 weeks, followed by 3 month and 6-month intervals, provided there is a positive posttreatment response trend.
To our knowledge, this is the largest series to date evaluating the combination of anti-VEGF and PDT in the treatment of CCH. 22,23 In fact, there are limited data regarding the use of anti-VEGF in any setting for the treatment of CCH. 24 –26 We report no adverse effects of combined use of these 2 therapeutic modalities in the management of CCH as well as promising outcomes when combination treatment is used for recalcitrant lesions.
This armamentarium of bevacizumab and PDT allows for treatment to be tailored to individual patients’ unique characteristics. In our experience, examples of factors that warrant consideration for the use of bevacizumab include peripapillary or macular tumor location, extensive leakage requiring debulking, or a history of prior PDT sessions with little improvement of exudation.
Future case–control studies are needed to explore synergies between intravitreal agents and laser therapies and to better delineate the role and timing of anti-VEGF administration when managing CCH. Additionally, based on both our experience and the literature on other exudative conditions such as Coats disease, 27 we believe that newer anti-VEGF agents such as ranibizumab and aflibercept also have the potential to improve vision and exudation in CCH, and their use as monotherapy and in combination with PDT merits further investigation.
In summary, our study supports the effectiveness and safety of PDT as a primary treatment modality. In addition, our study suggests the independent efficacy of bevacizumab monotherapy in select patients, the synergistic response to bevacizumab with repeated PDT, and the potential reduced requirement for PDT treatments by adding bevacizumab to the treatment protocol.
Footnotes
Acknowledgments
The authors would like to acknowledge Research to Prevent Blindness (RPB) for their funding support of this manuscript.
Authors’ Note
Previously presented at the American Academy of Ophthalmology Annual Meeting, Las Vegas, NV, November 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research to Prevent Blindness