
Abstract
Purpose:
A small subset of patients with neovascular age-related macular degeneration (AMD) can have relentless progression of choroidal neovascularization (CNV) and subsequent disciform scarring (DS) with extension beyond the vascular arcades to the equator. We present the clinical courses of this severe phenotype of progressive massive CNV (PM-CNV).
Methods:
Retrospective case series of 14 eyes of 8 patients who presented with (1) massive DS encompassing the posterior pole and extending to the equator and (2) progressive DS expansion despite treatment between 2004 and 2015 at a tertiary referral center. Demographics, clinical and ocular characteristics, fluorescein angiographic findings, and treatment regimens were reviewed.
Results:
Baseline characteristics included a mean age of 73.0 years (range, 65.- 86.9 years) with 7 (87.5%) women. Six (75%) patients had bilateral PM-CNV. Mean follow-up was 10.5 years (range, 0.5-18.2 years). Ten (71.4%) eyes underwent intravitreal anti-vascular endothelial growth factor therapy, 3 (21.4%) intravitreal corticosteroid injections, and 3 photodynamic therapy. Most eyes (92.9%) demonstrated subretinal hemorrhage at the edge of the DS prior to DS expansion during treatment. Of the 6 patients with bilateral PM-CNV, 5 developed DS in 1 eye earlier than the subsequent eye (mean time, 63.6 months). Final visual acuity was ≤20/400 in all eyes (20/400 [n = 1]), count fingers (n = 5), hand motions (n = 5), and no light perception (n = 3).
Conclusion:
Progressive massive CNV is a profound reactivation of DS in some AMD eyes and is associated with severe, often bilateral, vision loss.
Introduction
Age-related macular degeneration (AMD) is the leading cause of irreversible vision loss in those over 50 years of age. 1 -3 The neovascular form of AMD can cause rapid progression of central vision loss when left untreated. Serous fluid, lipid, and blood can leak from friable, fenestrated vessels from the choriocapillaris and subsequently lead to fibrous scarring. 4 Fibrotic disciform scarring (DS) typically represents the quiescent end-stage finding of advanced neovascular AMD 5,6 ; however, a small subset of patients can have profound reactivation of these lesions with extension beyond the vascular arcades to the equator and associated hemorrhage and vision loss. 5,7,8 The clinical features and course of these patients are not well described. Herein, we describe the clinical course of a series of patients who developed a severe phenotype of neovascular AMD with massive expansion of DS, refractory to treatment, that we term progressive massive choroidal neovascularization (PM-CNV).
Methods
We conducted a retrospective chart review of all patients with neovascular AMD treated at our single tertiary referral practice (Associated Retinal Consultants, PC, Royal Oak, Michigan) from March 2004 to November 2015. Inclusion criteria for this study were those who presented with, or later developed, (1) a massive DS that involved the entire posterior pole and extended to at least the equator and (2) progressive DS expansion despite treatment.
We collected demographic and clinical characteristics including age, gender, eye, ocular and medical history, and initial and final Snellen best corrected visual acuity (BCVA). Baseline and follow-up AMD features, including the presence of drusen, retinal pigment epithelial (RPE) changes, pigment epithelial detachment (PED), CNV, subretinal hemorrhage (SRH), and DS, were identified based on a combination of clinical examination and review of fundus photography and fluorescein angiography (FA). We also recorded treatment regimens, including the use and number of photodynamic therapy (PDT) sessions, intravitreal anti-vascular endothelial growth factor (anti-VEGF), and intravitreal corticosteroid injections.
This study was approved by the Western Institutional Review Board. The protocol and methods utilized also complied with the standards set forth by the Declaration of Helsinki.
Results
Fourteen eyes from 8 patients met the inclusion criteria. Baseline characteristics and clinical features are listed in Table 1. Mean patient age at presentation was 73.0 years (range, 65.5-86.9 years), and our mean follow-up was 10.5 years (range, 0.5-18.2 years). Of these patients, 7 (87.5%) were female and all were Caucasian. Six (75%) patients had bilateral disease and 2 (25%) had unilateral disease.
Patient Characteristics and Clinical Features of Progressive Massive Choroidal Neovascularization (PM-CNV) in Neovascular Age-Related Macular Degeneration.
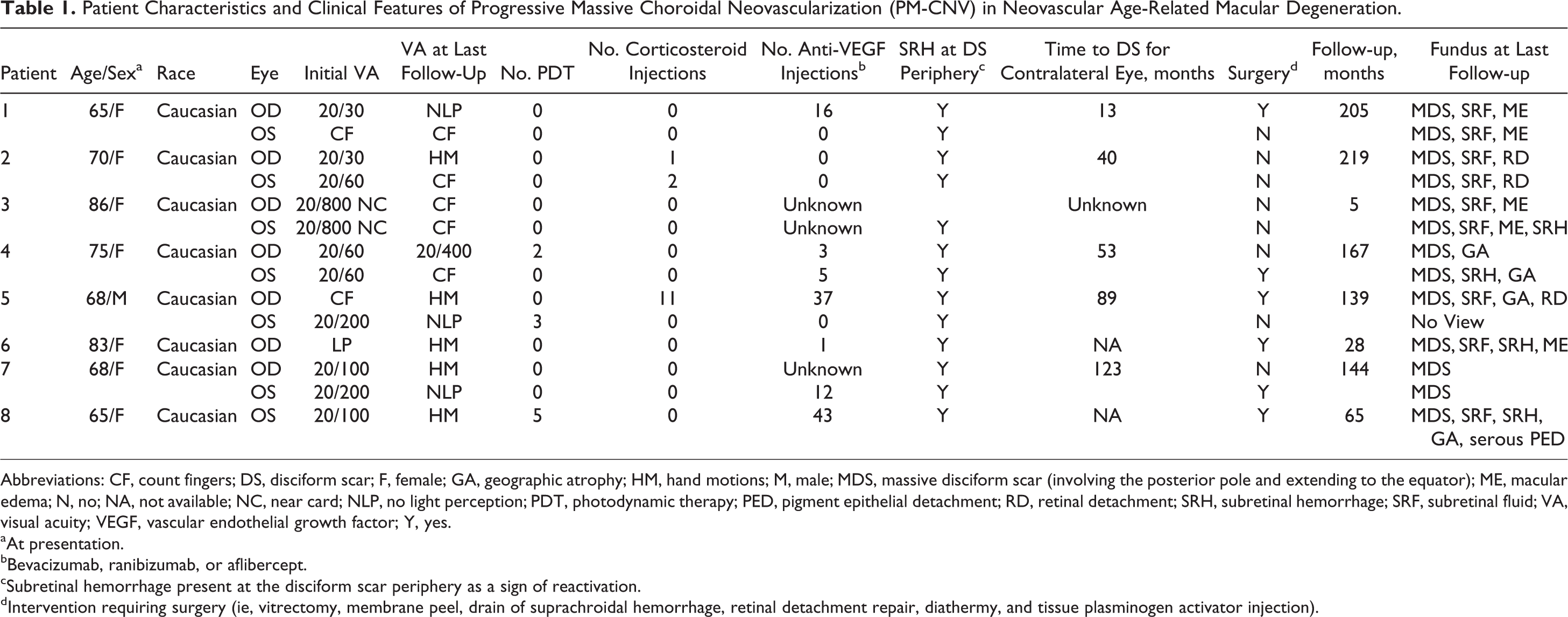
Abbreviations: CF, count fingers; DS, disciform scar; F, female; GA, geographic atrophy; HM, hand motions; M, male; MDS, massive disciform scar (involving the posterior pole and extending to the equator); ME, macular edema; N, no; NA, not available; NC, near card; NLP, no light perception; PDT, photodynamic therapy; PED, pigment epithelial detachment; RD, retinal detachment; SRH, subretinal hemorrhage; SRF, subretinal fluid; VA, visual acuity; VEGF, vascular endothelial growth factor; Y, yes.
aAt presentation.
bBevacizumab, ranibizumab, or aflibercept.
cSubretinal hemorrhage present at the disciform scar periphery as a sign of reactivation.
dIntervention requiring surgery (ie, vitrectomy, membrane peel, drain of suprachroidal hemorrhage, retinal detachment repair, diathermy, and tissue plasminogen activator injection).
Four (28.6%) eyes had concurrent primary open angle glaucoma (POAG). Systemically, 5 (62.5%) of the 8 patients had a history of hyperlipidemia, 2 (25%) patients exhibited type 2 diabetes mellitus, and all 8 (100%) patients had hypertension.
Baseline BCVA at the initial examination ranged from ≥20/60 (n = 5), 20/100 to 20/800 (n = 6), count fingers (CFs; n = 2), and light perception (n = 1). Final BCVAs were 20/400 (n = 1), CFs (n = 5), hand motion (n = 5), and no light perception (NLP; n = 3).
At the initial examination, 4 (28.6%) eyes exhibited drusen and RPE changes; 6 (42.9%) eyes had a PED and/or CNV, and 4 (28.6%) eyes already demonstrated a DS. One eye presented with massive CNV (patient 3, eye 5), and all others subsequently developed PM-CNV (Figure 1).
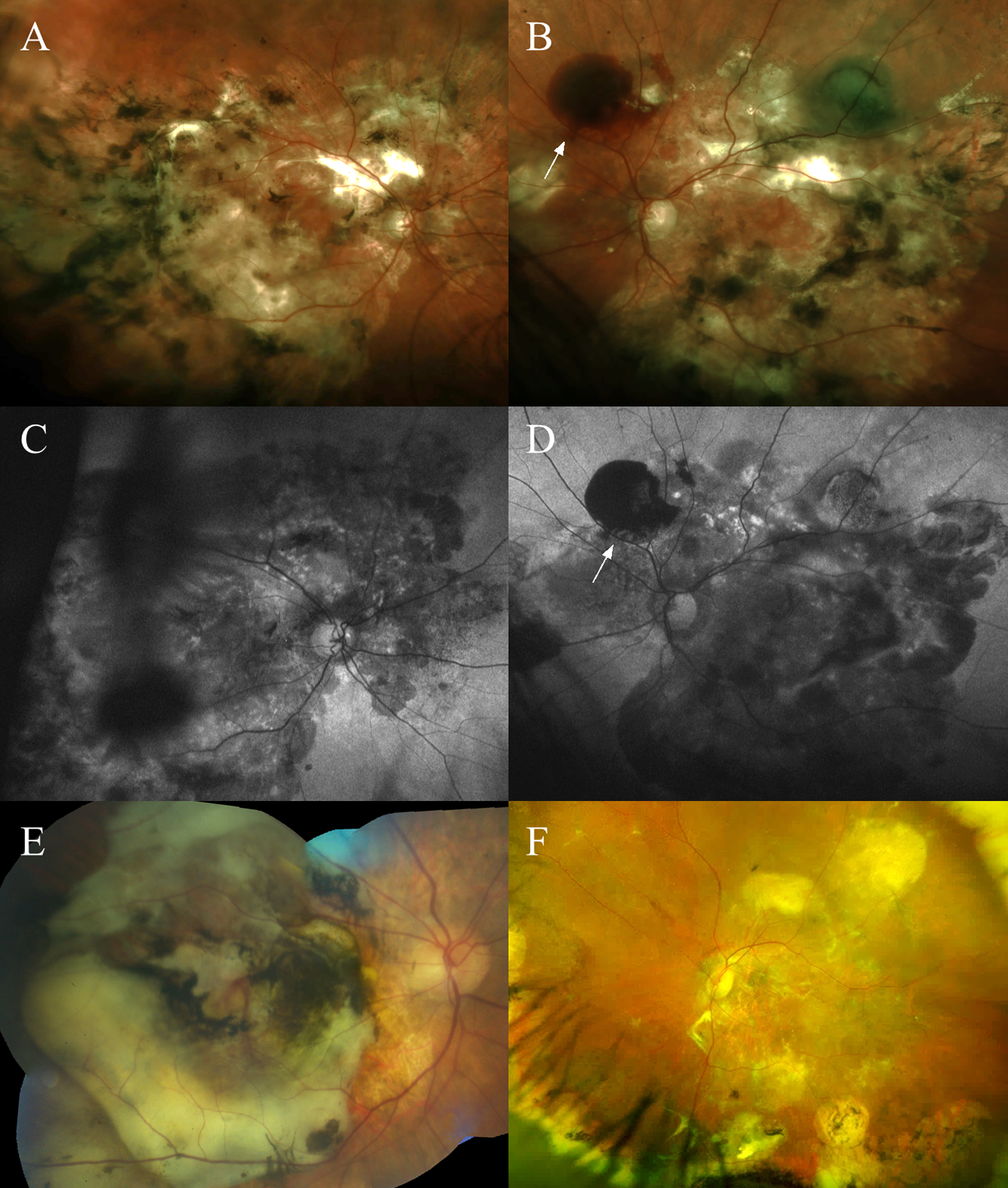
Widefield color fundus photograph and fundus autofluorescence demonstrating massive disciform scarring (DS) and subretinal fluid of the right (A, C) and left eye (B, D) in patient 3. Note the subretinal hemorrhage (SRH; white arrow) at the superonasal scar periphery in the left eye (B, D). Color photograph montage of the right eye from patient 4 with massive DS, geographic atrophy, and SRH (E). Widefield color fundus photograph of the left eye from patient 8 with massive DS, geographic atrophy, and subretinal fluid (F).
Of the patients who developed PM-CNV, SRH at the border of the DS lesion preceded lesion expansion in all eyes (100.0%). Six (42.9%) eyes developed vitreous hemorrhage (VH) from breakthrough of the SRH.
Regarding treatment, 10 (71.4%) eyes underwent intravitreal anti-VEGF therapy (1-43 injections), 3 (21.4%) eyes intravitreal corticosteroid injections (1-11 injections), and 3 (21.4%) eyes PDT (1-5 sessions); none of these modalities halted DS progression.
Vitreoretinal surgery was performed most commonly for VH. Pars plana vitrectomy was required for 4 (66.7%) of the 6 eyes with VH; 1 eye required multiple vitrectomies. Five (35.7%) eyes developed rhegmatogenous retinal detachments. All 5 eyes underwent either pars plana vitrectomy or scleral buckling. Additionally, 1 eye received an intravitreal C3F8 injection for a large macular SRH, 1 eye underwent hyaloid membrane stripping and diathermy to the CNV with a chorioretinal anastomosis, and 1 eye underwent a vitrectomy and subretinal injection of tissue plasminogen activator for a large SRH. Reactivation of CNV activity occurred in 5 eyes after vitrectomy and in 1 eye following the development of endophthalmitis.
The PM-CNV lesions were bilateral in 6 (75%) of the 8 patients; however, they developed asymmetrically. The mean time to contralateral development of PM-CNV was 63.6 months (range, 16-132 months). In the 2 patients (patients 6 and 8) with unilateral lesions, the unaffected eyes maintained good vision at last follow-up with BCVA of 20/25 at 2.4 years and 20/30 at 8.2 years, respectively. The fellow eye of patient 6 demonstrated CNV with a PED, trace edema, and early geographic atrophy on last fundus examination. This eye responded to intravitreal anti-VEGF therapy with 24 injections at increasingly extended intervals. The fellow eye of patient 8 exhibited an inactive CNV with a PED on last examination with a total of 3 intravitreal anti-VEGF injections and 1 session of PDT therapy.
Progressive massive CNV was associated with NLP vision in 3 eyes. The mean time from development of neovascular AMD to NLP vision was 51.2 months (range, 36-72 months). Two of the eyes (patient 1 right eye, patient 7 left eye) exhibited optic nerve pallor at the final visit. These 2 eyes also underwent pars plana vitrectomy during their course for breakthrough VH (Patient 1, right eye) and subretinal tissue plasminogen activator injection for SRH (patient 7, left eye). Of note, patient 7 was lost to follow-up for 6 years, during which his eye went from LP to NLP vision. Only one had baseline POAG and exhibited optic nerve cupping (patient 1, right eye). Two eyes received multiple anti-VEGF injections without any PDT, while the third eye received PDT treatments only (patient 5, left eye).
Sample Cases
Patient 1
A 65-year-old Caucasian woman with a history of hypertension and hyperlipidemia presented with decreased vision in her left eye in 1998 and was followed for 18 years. Ocular history was significant for POAG and epithelial basement membrane dystrophy.
At initial presentation, BCVA was 20/30 and CFs in the right and left eye, respectively. The right eye had only drusen, while the left eye exhibited active CNV that was treated with focal laser. After 7 months, the left eye developed a sub-RPE hemorrhage. A DS then appeared 1 year later (2 years from initial presentation).
Over the next 5 years, the left eye sustained 5 additional episodes of SRH along the DS periphery that extended the lesion past the arcade vessels (2000-2004) and then 2 additional episodes accompanied by breakthrough VH in 2006. The massive DS remained quiescent for 7 years until it reactivated again in 2013 with an isolated episode of SRH; the scar remained quiet for 3 more years until the last follow-up in late 2016.
While the right eye exhibited drusen at initial presentation in 1998, it developed cystoid macular edema (CME) without CNV on FA and responded well to topical medications. Over time, there was gradual enlargement of the drusen and a PED developed 2 years later. In 2007, FA demonstrated an active CNV, and the patient was started on monthly intravitreal ranibizumab injections. She received a total of 16 intravitreal injections at 4- to 5-week intervals. In late 2008, the eye developed a retinal detachment with proliferative vitreoretinopathy that required a scleral buckle and pars plana vitrectomy.
A DS developed in February 2009, approximately 11 years after initial presentation. Intravitreal injections were continued until the patient sustained a large 6 clock hour temporal sub-RPE/SRH with subsequent breakthrough VH 5 months later (May 2009) and another VH with hyphema and suprachoroidal hemorrhage 1.5 years later, which required vitrectomy, suprachoroidal drainage, and silicone oil.
On final examination, the right eye’s optic nerve was pale and cupped. Both eyes demonstrated massive disciform scars extending well past the arcade vessels toward the equator. Visual acuity was NLP and CF in the right and left eye, respectively.
Patient 2
A 70-year-old Caucasian woman with a history of hypertension, diabetes mellitus, hyperlipidemia, and breast cancer was referred for AMD management in 1994 and followed for 18 years. She has had POAG treated with trabeculoplasty bilaterally and multiple iridectomies. On initial examination, BCVA was 20/30 and 20/60 in the right and left eye, respectively. The right eye had drusen and RPE changes, while the left eye demonstrated CME, drusen, RPE changes, and a large PED that extended from the fovea to the inferotemporal arcade vessel without frank evidence of CNV on FA.
Over the next 7 months, the left eye developed ill-defined CNV with a subsequent large SRH (greater than 8 disc diameters) in the middle of the PED. Because this exceeded the size recommended by the Macular Photocoagulation Study for treatment, the hemorrhage was observed. By 1995, the left eye developed additional SRHs at the border of the PED as the large CNV extended outside the arcade vessels. From 1999 to 2000, the eye developed increasing amounts of SRH along the border of the DS. For increasing loss of peripheral vision at a time with no available anti-VEGF agents, a trial of intravitreal triamcinolone (IVK) was given to the left eye, with subsequent subretinal fluid (SRF) improvement. However, additional treatments were halted due to steroid-related intraocular pressure (IOP) rises.
In 1997 (3 years after initial presentation), the right eye progressed to develop multiple PEDs, including one that extended from the fovea to the inferotemporal arcade vessel. There was no hemorrhage or leakage on FA, but 3 months later, the large area of CNV fully encompassed the macula. Given its size, no treatment was recommended. Three years later, the CNV extended past the temporal arcade vessels as well as far nasally with subsequent DS. Nine years after initial presentation, the CNV rapidly progressed developing extensive SRH at the border of the lesion and accompanying leakage on FA. A trial of IVK was administered. However, due to an IOP response, no additional IVK injections were performed. She was observed until her final visit in 2012 with HM vision in the right eye and CF vision in the left eye. At the time of her passing, both eyes revealed PM-CNV and DS extending to the equator with large areas of SRF but no hemorrhage.
Discussion
Disciform scars are a known sequela of progressive neovascular AMD. As the angiogenic stimulus declines, DS becomes less vascular and more fibrotic. 9 We present the clinical course of a rare phenotype of neovascular AMD with massive PM-CNV and DS that progressively extends toward the equator despite treatment.
Pathophysiologically, DS may be preceded by either serous or hemorrhagic detachment of the RPE and sensory retina. 10 -12 Chandra et al demonstrated that over an average period of 22 months (up to 4 years), 45% of serous detachments progressed to scar formation, while 78% of eyes with hemorrhagic detachment progressed to scar formation. 10 They also observed that the amount of SRF tends to fluctuate in the short term, but over the long term, gradually increases the macular detachment and leads to subsequent fibrovascular scar formation. 10,13 -15 Teeters and Bird suspected that the gradual organization and increase in fibrous content that occurs after the resolution of exudate and hemorrhage promoted expansion of the scars into the periphery as inactive and active borders coalesce. They demonstrated that the amount of serous, hemorrhagic, and exudative material in the subretinal and RPE spaces correlated with the degree of fibrous content in the disciform lesion. 14
More rapid progression to scarring from blood may occur because whole blood is a more potent stimulus of fibrous proliferation than serum. 10 This cyclical mechanism of SRH followed by DS formation in an expanding pattern explains the proliferative nature we observed in our cohort. Scar formation and expansion may also be a function of CNV type. Recent optical coherence tomography angiographic findings 16 and multimodal imaging suggest that type 1 CNV 17 lesions may be protective against geographic atrophy formation, as opposed to type 2 CNV.
As expected, we observed a decline in vision after scar formation and expansion. Green and Enger correlated photoreceptor loss with the thickness of the disciform scar. 13 Scars thicker than 0.2 mm were associated with severe photoreceptor loss, whereas thinner scars were associated with lower levels of damage. The dysfunction and death of photoreceptors is certainly a major contributor to vision loss in AMD, 18,19 and this would explain the poor visual acuity of CF to HM in 10 (71.4%) of the 14 eyes. Additionally, we noted NLP vision in a subset of eyes (3 of the 14 eyes, 21.4%), which is generally unusual in AMD due to macular pathology. This finding may be attributed to peripapillary subretinal fibrosis and damage leading to chronic ischemic optic neuropathy. 20 The study by Brown et al of AMD eyes with NLP vision included 1 patient with subretinal fibrovascular tissue proliferation throughout the entire fundus. 20 There may be an overlap of the phenotype between the NLP eyes with 360° peripapillary subretinal fibrosis and our eyes with massive DS lesions.
Additionally, we noted that 5 (35%) eyes developed rhegmatogenous retinal detachments, which may have also contributed to the poor visual results. The exact pathophysiology or correlation is unknown. One possibility is that the extensive retinal thinning and/or recurrent hemorrhages at the border of the PM-CNV lesions may predispose to retinal tears. However, further studies are needed to confirm this hypothesis. Of note, 2 of the 3 eyes with NLP vision at the final visit underwent previous vitrectomy for breakthrough VH and/or SRH.
Primary open angle glaucoma was present in 4 (28.6%) eyes. Of the 3 eyes with optic nerve pallor in our cohort, only 1 eye had concurrent glaucoma. Although glaucoma may be a potential confounder in the poor visual outcomes, it may not entirely explain the NLP vision in 2 of the 3 eyes.
Disciform degeneration is reported to develop in the fellow eye in 14% to 34% of patients with AMD having CNV. 10,14,21 In our cohort, the majority of patients (75%) demonstrated bilateral (often sequential) expression of large DS lesions with a mean of 64 months prior to contralateral involvement. Only 2 patients exhibited a unilateral massive DS lesion. It may be that these patients have not yet manifested a massive DS lesion in the fellow eye. Lavin et al found a relationship between the CNV scar size of 1 eye and the size of the scar in the fellow eye, implying that certain factors inherent to an individual may have an important role in determining how advanced the process of CNV and fibrosis become. 22 They observed that the degree of concordance between scar size among the eyes increased with time, suggesting that variation between eyes at a single time point could be attributed to slowly evolving lesions that have not reached their final scar size. Although patients with a small macular scar had a ∼16% risk of developing a large macular scar in the remaining eye, 50% of patients with a large established scar developed large scars in the fellow eye. 22
Although disciform scars typically remain stable over time, signs of activity such as hemorrhage on examination, fluorescein angiographic leakage, and fluid on optical coherence tomography suggest that even chronic CNV can grow and cause further visual impairment. 23 An indocyanine green (ICG) angiogram can be considered if there is new hemorrhage, exudate PED, or serous PED at the margin of the disciform scar. 5 According to Coco and Sala-Puigdollers, if a “hot spot” is seen on ICG, patients may potentially benefit from focal laser photocoagulation as this helps to stabilize the disease and possibly avoid additional complications such as massive hemorrhage. 5 In a randomized clinical trial, Parodi et al demonstrated that intravitreal bevacizumab for advanced stage neovascular AMD did not provide benefit. 6 They hypothesized that the lack of response to anti-VEGF may be due to the advanced stage with irreversible photoreceptor–RPE cell damage. 6 It is not surprising that our patients’ lesions, each with very large portions of subretinal fibrosis, were unresponsive to all anti-VEGF treatments and even PDT.
We acknowledge that some eyes, as in our vignettes, were initially observed as their original presentation and course occurred during the pre-anti-VEGF era and may reflect the natural history of expanding DS. However, the contralateral eye DS in our patients expanded despite anti-VEGF therapy. Therefore, the role of anti-VEGF medications in these cases of PM-CNV remains unclear, either the reactivation and expansion of these scars is refractory to treatment and/or anti-VEGF agents play a role in DS formation by initiating a fibrotic response in these very active lesions. 24
There are several limitations to our trial including its retrospective nature and the fact that it was compiled from a patient population at our tertiary care retina referral practice which may introduce some referral bias. Data were incomplete for periods of time for 2 patients due to loss of follow-up. One eye was part of the MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular AMD) trial so its treatment regimen was unavailable during the study period. Although the long-term follow-up is a strength of this study, some patients initially presented during the pre-anti-VEGF era and were initially managed with observation based on Macular Photocoagulation Study (MPS) criteria. Currently, this would not be the management course for such eyes. Lastly, while massive DS was identified as the main source of vision loss, vitrectomy for SRH, retinal detachment repair surgery, glaucoma, and endophthalmitis may be confounding factors for vision loss as well, which could not be controlled or further separated given the small sample size.
In summary, we present a rare phenotype of neovascular AMD with massive CNV that extends toward the equator. The finding is often bilateral and invariably causes profound visual loss. Progression is noted to occur as relentless reactivation of the border of these DS lesions and in some cases may not be controlled with anti-VEGF therapy, particularly when it is initiated late.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Yoshihiro Yonekawa (Allergan), Antonio Capone, Jr (Alcon, Aura Biosciences, FocusROP, Novartis Pharmaceuticals Corporation, Ohr Pharmaceuticals, Spark Therapeutics, ThromboGenics, Inc, Retinal Solutions, Otsuka Pharmaceutical Co, GENENTECH, Iconic Therapeutics), Tarek Hassan (Alcon, Allergan, Arctic Dx, Genentech, Novartis, Regeneron, Roche).