
Abstract
A 70-year-old Caucasian gentleman presented with decreased vision in the left eye and a subtle whitish macular plaque in the left eye and pigment mottling bilaterally. Indocyanine green angiography (ICGA) and optical coherence tomography angiography (OCTA) revealed left macular hypoperfusion. Systemic evaluation was negative for infectious or inflammatory disorder. A diagnosis of persistent placoid maculopathy was made and systemic immunosuppression was initiated. A marked improvement in macular perfusion was noted on ICGA and OCTA following 1 week of immunosuppression, providing additional evidence of an inflammatory rather than ischemic etiology.
Introduction
Persistent placoid maculopathy (PPM) was initially described by Golchet et al as a typically bilateral condition featuring well-delineated whitish plaque-like lesions in the macula. 1 Progression to macular atrophy and choroidal neovascularization can limit visual potential. Choroidal hypoperfusion on indocyanine green angiography (ICGA) is a hallmark feature of this condition, the cause of which is unknown. Inflammatory and/or ischemic factors are potential etiologies. The author describes a case of PPM treated with prednisone and imaged with ICGA and optical coherence tomography angiography (OCTA) before and after initiation of treatment.
Case Report
A 70-year-old Caucasian gentleman with a history of hypertension and psoriatic arthritis controlled with low-dose etanercept presented with decreased vision for 2 weeks in the left eye. His visual acuity was 20/30 OD (right eye) and 20/250 OS (left eye). Intraocular pressure was normal OU (both eyes), and there was no relative afferent pupillary defect. Anterior segment examination was significant for nuclear sclerotic cataracts OU. There was no anterior chamber or vitreous inflammation. Fundus examination revealed pigment mottling in the right macula and a subtle whitish plaque and pigment mottling in the left macula. Spectral domain optical coherence tomography (SD-OCT) revealed a thin fovea OU with disruption of the external limiting membrane (ELM) and ellipsoid layers with thickened and disrupted retinal pigment epithelium (RPE) OU, more prominent in the left eye (Figure 1B). Indocyanine green angiography revealed well-defined choroidal hypofluorescence in the center of the left macula (Figure 1C). Optical coherence tomography angiography showed an area of low choriocapillaris flow slightly larger in area and less well-defined compared to the ICGA image (Figure 1A). Systemic workup included erythrocyte sedimentation rate, C-reactive protein, CMV IgM, ANCA, lysozyme, angiotensin-converting enzyme, RPR, FTA-Abs, ANA, and HIV, which were all negative. Platelet levels were within normal range but low. Carotid ultrasound and echocardiogram were unremarkable. Systemic immunosuppression with oral prednisone at 60 mg/d was initiated. After 1 week of treatment with prednisone, the patient reported a subjective visual acuity improvement. Snellen visual acuity was stable in both eyes. Fundus examination remained stable, and persistent RPE disruption was noted on SD-OCT of the left macula (Figure 2B). Indocyanine green angiography revealed a smaller area of choroidal hypofluorescence, and choriocapillaris flow had improved on OCTA (Figure 2A and C).
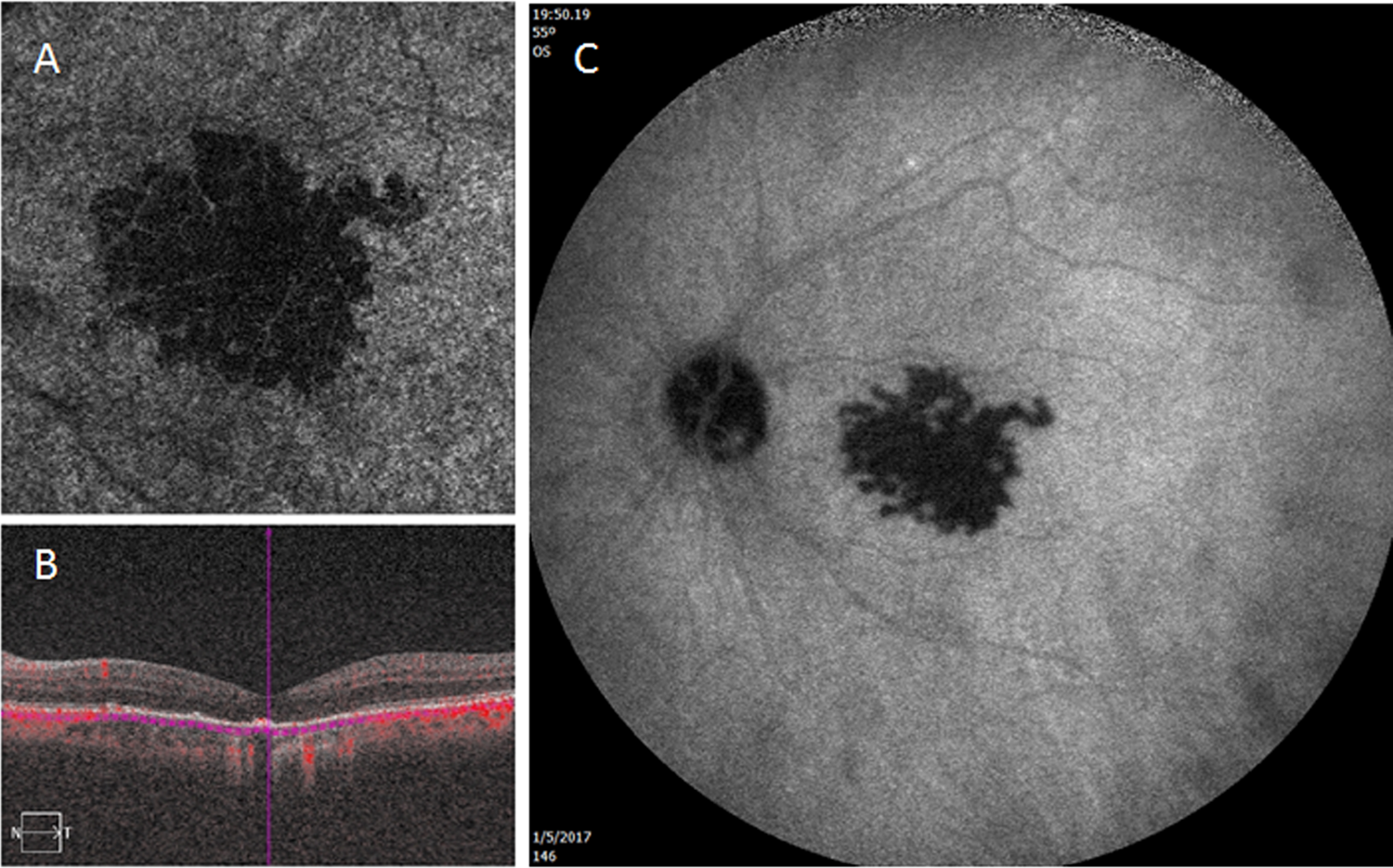
(A) Zeiss angioplex OCTA demonstrates low flow in the choriocapillaris in the central left macula. (B) Outer retinal disruption in the left macula on Heidelberg Spectralis SD-OCT. (C) Late-phase ICGA shows choroidal hypofluorescence in the left macula. ICGA, indocyanine green angiography; OCTA, optical coherence tomography angiography; SD-OCT, spectral domain optical coherence tomography.
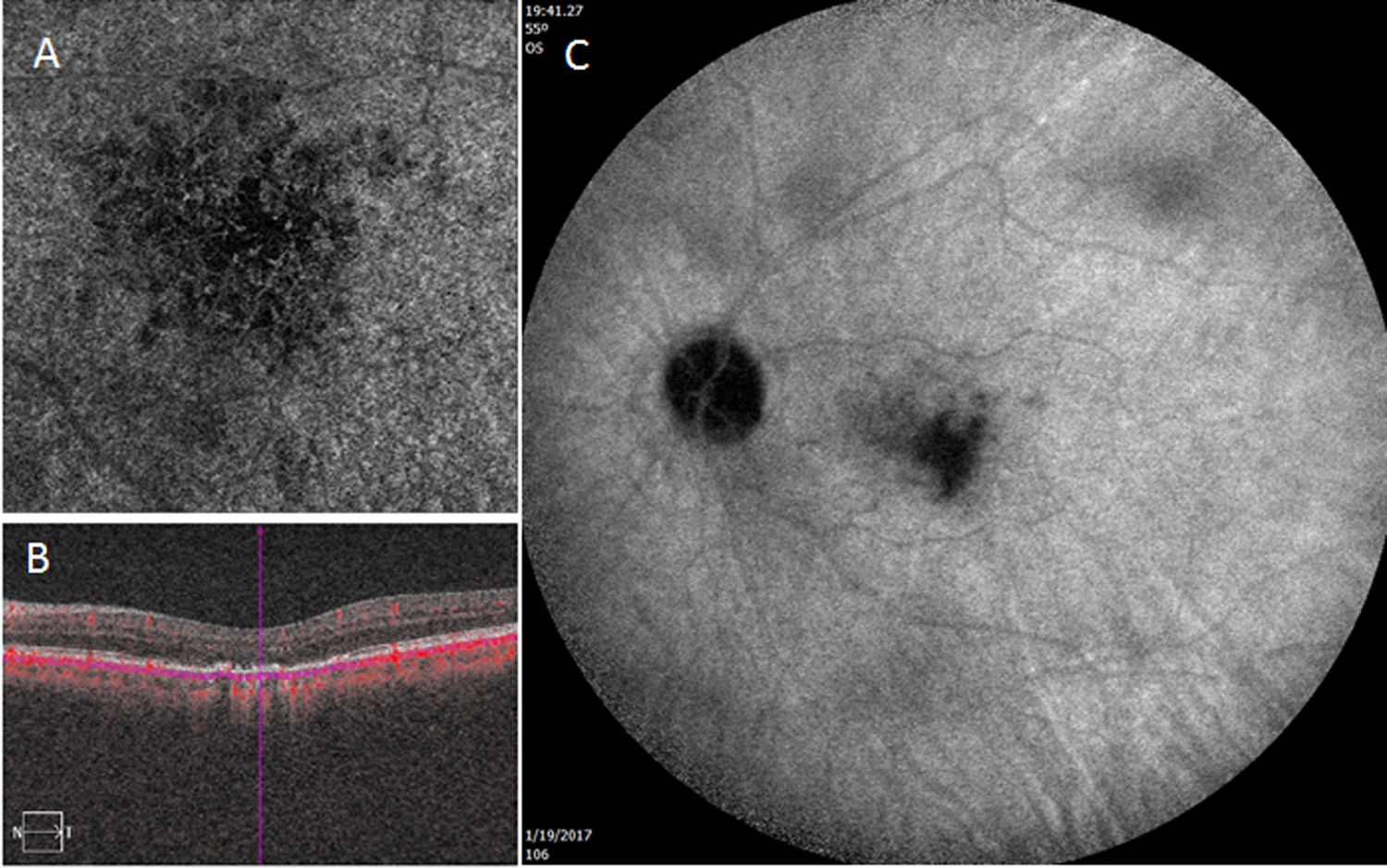
(A) Zeiss angioplex OCTA shows improved flow in the choriocapillaris after 1 week of prednisone therapy. (B) Persistent outer retinal disruption with Heidelberg Spectralis SD-OCT. (C) Late-phase ICGA reveals improved choroidal perfusion. ICGA, indocyanine green angiography; OCTA, optical coherence tomography angiography; SD-OCT, spectral domain optical coherence tomography.
Discussion
Persistent placoid maculopathy is defined clinically by the hallmark features of typically bilateral whitish plaques in the deep macula that correspond to areas of choroidal hypofluorescence on ICGA. Spectral domain optical coherence tomography findings include outer retinal abnormalities such as disruption of the ELM, ellipsoid zone, and RPE. These changes lead to central vision compromise that can worsen as atrophy and choroidal neovascularization develop.
Optical coherence tomography angiography is a new imaging modality that allows visualization of vessels in the retina and choroid based on flow characteristics. 2 Because the area of low flow in the choriocapillaris is slightly larger than that noted on ICGA pretreatment and posttreatment, OCTA may offer improved visualization of the extent of vascular compromise that defines PPM. 3 The fact that marked improvement in choroidal perfusion is achieved with even short-term immunosuppression provides additional evidence that PPM is likely an inflammatory condition. 4 Maximization of visual potential requires early diagnosis and urgent initiation of long-term immunosuppression to avoid progression to atrophy and CNVM formation and permanent central vision compromise. 5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by NIH center grant P30-EY014801 and by an unrestricted grant to the University of Miami from Research to Prevent Blindness, New York, NY.