
Abstract
Purpose:
To investigate the clinical characteristics of central serous chorioretinopathy (CSCR) in the setting of exogenous testosterone use.
Methods:
Retrospective chart review of patients with a history of exogenous testosterone use and a diagnosis of CSCR at a large retina practice. Patient charts were reviewed for vision, clinical examination, and optical coherence tomography (OCT) results at each visit.
Results:
Four hundred eighty patients with a diagnosis of CSCR were identified, of which 7 patients had a history of exogenous testosterone use (1.46%). Of all, 0 of 7 patients reported any other steroid use. Ages ranged from 36 to 55 (mean, 46.57), and all were male. Only the right eye was involved in all 7 patients. Testosterone was discontinued in only 1 of the 7 patients. Six of the 7 patients had a visual acuity of 20/40 or better at last follow-up (range, 20/20-4/200). Three (43%) of the 7 had resolution of subretinal fluid at their last visit. The most common formulation of testosterone was for intramuscular injection.
Conclusions:
Exogenous testosterone use was reported in 1.46% of patients with CSCR compared to 0.8% in the general male population. The majority of patients in this study recovered 20/40 or better vision and 43% had resolution of subretinal fluid on OCT, suggesting a generally favorable prognosis for CSCR in the setting of testosterone supplementation.
Keywords
Introduction
The etiology of central serous chorioretinopathy (CSCR) is not fully understood, despite the prevalence of the disease. 1 It has been associated with several risk factors such as age (mean age, 40-45), male sex, smoking, type A personality, corticosteroid treatment, Cushing syndrome, infection, and emotional stress. 1 –3
Although the association between cortisol and CSCR has been well established, the effect of testosterone on CSCR is not as well delineated. Serum levels of testosterone have not been shown to be elevated in CSCR. 4 –6 However, there are case reports of exogenous testosterone use in association with CSCR in men and women. 7 –10 Testosterone supplementation has become increasingly popular, despite some controversy regarding the risks and benefits. 11 –13 Thus, the incidence of patients who develop CSCR while on testosterone supplementation may increase in the future. Here, we investigate the association between exogenous testosterone use and development of CSCR.
Methods
The study identified patients via International Classification of Diseases, Ninth Revision codes from a large retina center who were seen between January 1, 2013, and November 10, 2015, and carried a diagnosis of CSCR. The diagnosis was made based on history, clinical examination, and optical coherence tomography (OCT) and fluorescein angiogram findings. Within this patient population, those who reported a history of exogenous testosterone use but no corticosteroid use on their medication lists were identified. Patient charts were reviewed, and information on gender, age, visual acuity, medications, examination findings, OCT results, treatment course, and duration of follow-up were collected going back from the patients’ first documented visit to the patients’ last visit.
Institutional review board approval for data collection and study was granted by IRBNet. The study was conducted in a HIPAA (Health Insurance Portability and Accountability Act) complaint fashion, and research adhered to the tenets of the Declaration of Helsinki.
Results
A total of 480 patients with a diagnosis of CSCR were identified. Seven (1.46%) of the patients had a documented history of exogenous testosterone use at the time of presentation. Of all, 0 of 7 patients reported any other steroid use. The ages of the patients ranged from 36 to 55 (mean, 46.57), and all were male. Only the right eye was involved in all 7 patients. The average follow-up time was 854 days, with a range of 14 to 4383 days.
Initial vision was 20/50 or better in all patients and remained 20/40 or better through 6 months. Testosterone was discontinued in only 1 of 7 patients. Six of 7 patients had a visual acuity of 20/40 or better at last follow-up (range, 20/20-20/40). The remaining patient developed subfoveal choroidal neovascularization which limited his final acuity to 4/200. Three (43%) of 7 patients had resolution of subretinal fluid at their last visit (Table 1).
Patient Clinical Characteristics.
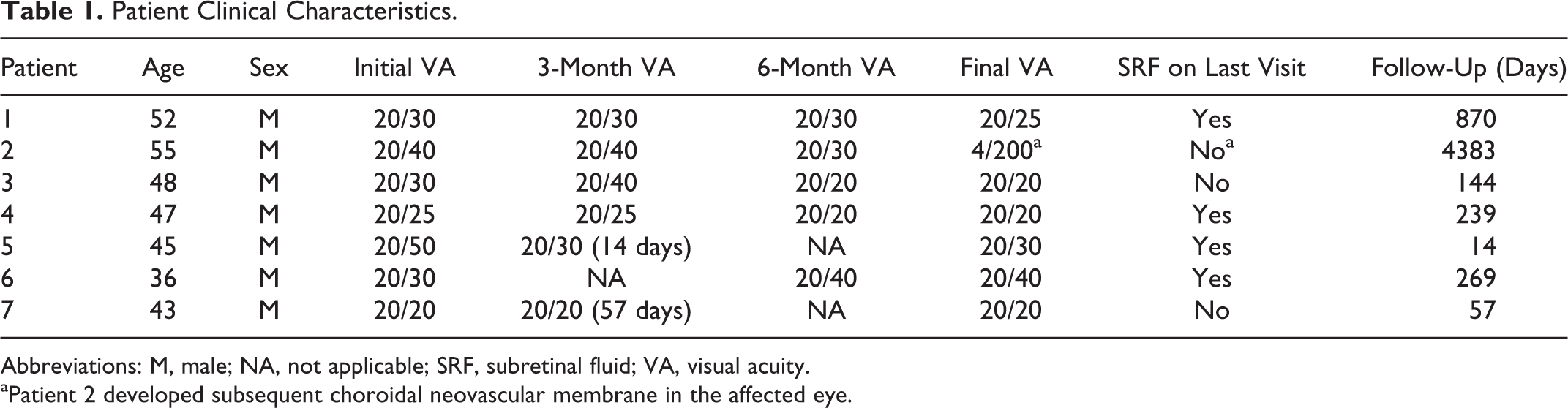
Abbreviations: M, male; NA, not applicable; SRF, subretinal fluid; VA, visual acuity.
aPatient 2 developed subsequent choroidal neovascular membrane in the affected eye.
Testosterone cypionate intramuscular injection was the most common formulation of testosterone among the study patients, with at least 5 of the 7 patients having used testosterone cypionate (Table 2). However, other formulations such as cream, pellet, and transdermal patch were also used by the patients.
Testosterone Formulations.
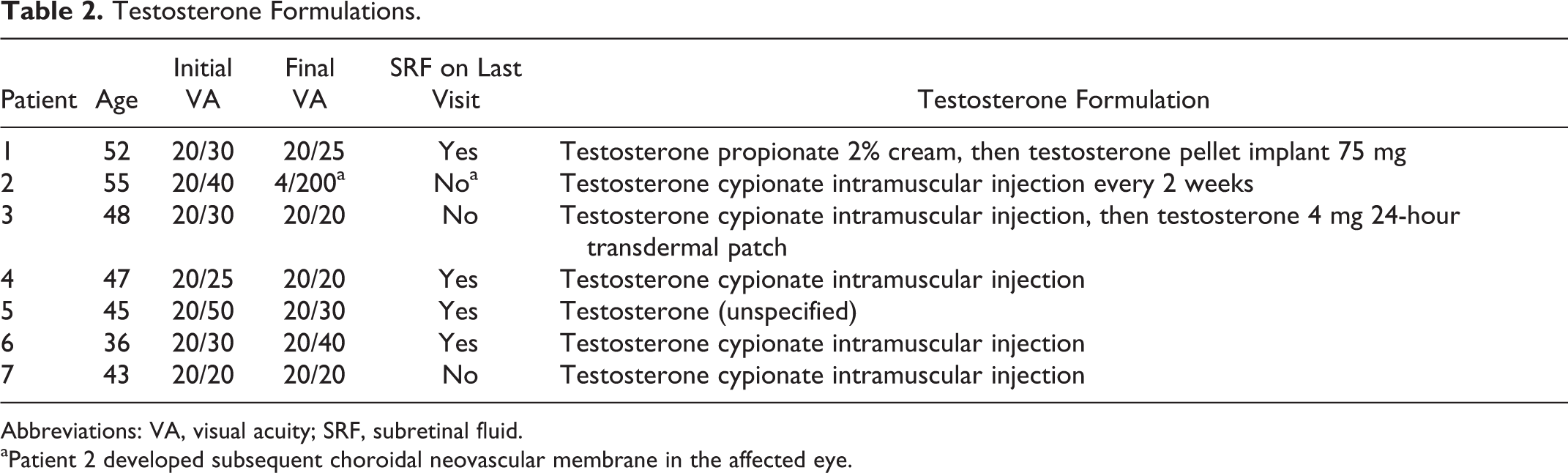
Abbreviations: VA, visual acuity; SRF, subretinal fluid.
aPatient 2 developed subsequent choroidal neovascular membrane in the affected eye.
Conclusion
We present 7 cases of CSCR associated with exogenous testosterone use. Patients with CSCR with a history of exogenous testosterone use accounted for a small percentage of all patients with CSCR in the study (1.46%). The majority of patients in this study recovered 20/40 or better vision and 43% had resolution of subretinal fluid on OCT, suggesting a generally favorable prognosis for CSCR in the setting of testosterone supplementation, even without discontinuation of testosterone.
One other case series in the literature describing exogenous testosterone use associated with CSCR found the mean age to be 51 years old, similar to the mean age of 46.57 in our current study, 7 which is close to the 41 to 45 mean age reported in the literature for all patients with CSCR. 1,2,3,14 This study and other case reports have shown an association between testosterone use and CSCR. 7 –10 In our current study, the prevalence of exogenous testosterone use among our patients with CSCR is 1.46%, which is 83% higher than the 0.8% prevalence of testosterone supplementation in the general male population in the literature. 13 However, due to the small sample size, it is not clear whether these CSCR cases reported here and elsewhere in the literature are merely unrelated coincidences of exogenous testosterone use or the direct result of testosterone supplementation. At the very least, the higher prevalence of testosterone supplementation may represent a possible risk factor or additional marker for patients already at risk for the development of CSCR.
Testosterone intramuscular injection was the most common formulation of testosterone supplementation in the current study in contrast to the report by Nudleman et al, in which testosterone gel was the most common formulation. 7 The route of administration may have an effect on the pharmacology of testosterone as evidenced by the varying cardiovascular risk associated with different routes of administration. 15,16 However, it is not clear whether the formulation of testosterone contributes to the risk of CSCR or whether the proportion of each formulation is due to prescriber and patient preference.
There are multiple hypotheses as to why testosterone supplementation may be related to the development of CSCR. Testosterone has been reported to cause vasodilation of the retinal microvasculature. 17 It is possible that supplemental testosterone may also cause vasodilation of choroidal vessels. A thickened choroid has been well documented in patients with CSCR utilizing OCT with enhanced depth imaging. 18,19 It is unclear what role a thickened choroid plays in the pathogenesis of CSCR, but it is possible that testosterone may contribute in part to this finding. Two studies evaluating treatment of CSCR with finasteride, an antiandrogenic agent, have shown promising results which support the theory of testosterone having a direct effect on the development of CSCR. 20,21
Conversely, low baseline testosterone levels may be a risk factor for CSCR and the use of supplements may simply be a marker for patients having low baseline testosterone. Androgens are involved in the regulation of tight junctions in the prostate and testis and may also play a role in regulation of tight junctions of the retinal pigment epithelium. 22,23 A reduction in androgen levels may contribute to loss of integrity of the blood–retina barrier, leading to transudation of fluid into the subretinal space and a neurosensory detachment as seen in patients with CSCR. More study is needed to elucidate the exact physiology predisposing these patients to CSCR.
Finally, low testosterone may play a role in dysregulation of glucocorticoid and mineralocorticoid pathways. It is well known that upregulation of corticosteroids from exogenous or endogenous sources is a risk factor for the development of CSCR. 24 –29 The mechanism by which this occurs has been previously described. 30 –32 Testosterone may actually have an antagonistic effect on mineralocorticoid receptors. 33 Thus, low testosterone levels may result in lack of inhibition of mineralocorticoid activity and increase the risk of CSCR in those predisposed to development of this condition. Low testosterone levels have also been associated with psychological stress and anxiety, which are also thought to be risk factors for CSCR. 34 –37 There is evidence that glucocorticoid activity has a direct inhibitory effect on testosterone production in Leydig cells. 38 –40 Whether low testosterone levels result in an increase in mineralocorticoid activity or whether increased glucocorticoid activity during stress simultaneously cross activates mineralocorticoid receptors while reducing testosterone levels requires further investigation.
The current study is a retrospective series susceptible to recall bias. Patients may not report use of testosterone for a variety of reasons such as simple forgetfulness, embarrassment, or nonmedical use (body building, etc), so the percentage of patients with CSCR using testosterone supplements may be higher than reported here. In addition, some patients may forget to report concurrent corticosteroid use along with testosterone supplementation which may confound the results. The study is also limited by the small sample size. The low incidence of CSCR (10 per 100 000 men) 2 coupled with the low prevalence of testosterone use makes assembling a large sample population that overlaps these 2 conditions challenging.
Although testosterone-associated CSCR makes up only a small proportion of all CSCR cases, the increasing popularity of testosterone supplementation may increase the role of exogenous testosterone as a cause of CSCR. At the very least, the use of testosterone supplements in a demographic that is susceptible to this disease may be considered a marker for potential CSCR or perhaps an additional characteristic. Additional larger scale studies are warranted to further elucidate the mechanism by which testosterone possibly contributes to CSCR. Low testosterone levels may increase mineralocorticoid activity, low testosterone may be merely a consequence of endogenous upregulation of glucocorticoid and mineralocorticoid activity, supplemental testosterone may be acting upon the choroidal vasculature to increase the risk of CSCR, or there may another mechanism. Currently, providers who are prescribing testosterone supplements should be aware of the potential risk or at least the possible association of CSCR in patients who fit this demographic. A review of systems with particular attention to vision problems should be included for patients being followed while on testosterone supplementation.
Footnotes
Authors’ Note
Material from this article has been presented at the Association for Research in Vision and Ophthalmology meeting in Seattle 2016.
Ethical Approval
Institutional review board approval for data collection and study was granted by IRBNet. The study was conducted in an HIPAA complaint fashion, and research adhered to the tenets of the Declaration of Helsinki.
Statement of Informed Consent
Informed consent was not sought for the present study because no identifiable images or data were used.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.