
Abstract
Purpose:
To describe a surgical technique and report visual and anatomical outcomes after primary combined pars plana vitrectomy (PPV) and phacoemulsification in patients with posterior segment intraocular foreign bodies (IOFBs) removed via the anterior chamber without enlarging preexisting sclerotomies. Posterior IOFBs are generally managed in a stepwise surgery consisting of phacoemulsification/lensectomy for traumatic cataract removal then PPV and removal of IOFB through enlarged sclerotomies. Enlarged sclerotomies may carry a significant risk of hypotony, vitreous hemorrhage, vitreous and retinal incarceration, and rhegmatogenous retinal detachment with proliferative vitreoretinopathy. Limited studies exist on long-term results of primary anterior segment removal of posterior IOFB combined with primary phacoemulsification.
Methods:
Medical records of consecutive patients who had ocular lacerations and posterior segment IOFB between October 2003 and June 2017 in a university hospital were reviewed. Patients who received a combined primary IOFB removal and phacoemulsification were included in the study. The postoperative evolution including visual acuity and complications were all recorded.
Results:
Thirteen patients (13 eyes) were included in the study. All patients were men, and the average age at presentation was 38 years. All IOFB were metallic, and their size ranged from 2 to 7 mm. All patients were operated within 24 hours of presentation. Six (46%) of the 13 lacerations were corneal, and 7 (54%) were scleral. Overall, 9 of 13 (69%) had a final postoperative best-corrected visual acuity equal to or better than 20 of 25. There were 3 (23%) postoperative complications of recurrent rhegmatogenous retinal detachment that occurred within the first postoperative year.
Conclusion:
Primary combined PPV and phacoemulsification with the removal of IOFB via the anterior segment is a safe and promising approach for repairing open globe injuries. Our results demonstrate the favorable prognostic benefit of this technique, which is recommended in cases with small corneal laceration and posterior segment pathology resulting from IOFB.
Keywords
Introduction
Worldwide, the incidence of open globe injury (OGI) is estimated to be 3.5 per 100 000 individuals, with a total of 203 000 cases per year. 1,2 In the United States, the incidence of open globe injury is estimated to be 3.8 per 100 000 individuals. 3 Men are 6 times more likely to have an open globe injury when compared to women. Specifically, men between the ages of 10 and 30 years old represent about 80% of cases. 4
According to the Birmingham Eye Trauma Terminology system, ocular injury is classified as closed or open globe injury. 5 Open globe injuries are further divided into lacerations and ruptures. Open globe injury with intraocular foreign body (IOFB) represents a subtype of open globe lacerations. 5 Intraocular foreign body injuries account for about 18% to 41% of all open globe injuries 6 –10 , and are, in 90% of cases, caused by small projectiles resulting from metal–metal, explosions, and/or motor vehicle accidents. 11 A large review of ocular trauma showed that 70% and 25% of patients who sustained IOFB injuries had final visual acuities (VAs) less than 20 of 70 and 20 of 200, respectively. 12,13 Following the removal of the IOFB, 40% and 8% of patients with IOFB injuries required additional interventions and enucleation, respectively. 14 Thus, there is a significant burden associated with IOFB injuries on patients’ quality of life; and this then highlights the importance of maximizing the anatomic and functional outcomes in IOFB injuries by revisiting preoperative, intraoperative, and postoperative management measures.
Previous studies have reported a variety of ocular pathologies following IOFB injuries including corneal wounds, iris damage, hyphema, lenticular damage, vitreous hemorrhage, and retinal detachment. 15 Cataract formation is a common complication of IOFB that could result from capsular breach by direct IOFB penetration or by action of shear forces on the globe. The prevalence of traumatic cataract in IOFB penetrating trauma was estimated to range between 27% and 65%. 15 –17 Often, cataract formation will interfere retinal visualization and will, thus, require eventual removal. The management of posterior segment IOFBs requires vitrectomy combined with foreign body (FB) removal using forceps or magnet to prevent scarring and proliferative vitreoretinopathy (PVR). 18
Intraocular foreign bodies are generally removed through enlarged sclerotomies due to ease of access. This technique carries, however, significant intraoperative risks of vitreous incarceration and hemorrhage, hypotony as well as the postoperative risk of retinal tear and detachment. To avoid such complications, FB removal can be achieved through vitrectomy ports or sclerocorneal tunnels depending on its size. 19,20
Limited studies exist on the prognostic advantages of primary anterior segment removal of posterior IOFB combined with primary phacoemulsification. In this study, we report the postoperative visual outcomes and ocular complications after primary PPV and phacoemulsification in patients with posterior segment IOFB removed via the anterior chamber without enlarging preexisting sclerotomies.
Method
Medical records of consecutive patients who had ocular lacerations and posterior segment foreign bodies between October 2003 and June 2017 in a university hospital were reviewed. The local research department confirmed that no ethical approval was required given the retrospective nature of the study, as there was no deviation from the usual standard of care. Direct written patient consent was not obtained for data collection and analysis, as such nonidentifying information has been included. Patients who received a combined primary PPV for posterior segment IOFB removal and phacoemulsification were included in the study. All surgeries were done by the same surgeon (G.C.) at the same institution. All patients underwent a complete ophthalmological examination and were operated within 24 hours of presentation. All patients were followed for a minimum period of 6 months postoperatively. All postoperative complications were recorded and treated adequately.
Eyes were excluded from the study based on the following criteria: severe uveal prolapse through entrance wound, severe iris dialysis and giant tears, significant globe disorganization, signs of intraocular infection, and evidence of retinal detachment on computed tomography scan or ultrasonography.
Pre- and postoperative VAs were recorded using a Snellen chart and were converted, for statistical purposes, to logarithm of minimum angle of resolution (logMAR) units. Counting fingers (CFs) and hand motion (HM) VA were recorded as 1.85 and 2.3 logMAR units, respectively. 21 Data collection was carried out using Excel software (Microsoft Excel for Mac 2011, Microsoft, Redmond, Washington), and statistical analysis was done using SPSS (SPSS version 20.0, Chicago, Illinois). Wilcoxon rank test was used for comparison of pre- and postoperative VA. A P value <.05 was considered statistically significant.
We classified the ocular lacerations based on their anatomical location according to the Ocular Trauma Classification Group 22 : zone I injuries were limited to the cornea, zone II injuries extended 5 mm posteriorly from the limbus into the sclera, and zone III injuries involved the sclera more posterior than the first 5 mm from the limbus. Postoperative evolution including visual acuity (VA) and complications was recorded. We used the standardized classification of Machemer et al to diagnose PVR. 23 In this study, any patient with grade B or C PVR over any clock hour was considered sufficient for making the diagnosis of PVR postoperatively.
Surgical Technique
Preoperative examination is very important to identify the site of entry of the FB and evaluate for the capsular and zonular integrity, and retinal detachment. Computed tomography (CT) scan of the orbits and ultrasound B-Scan were performed in all patients to locate and evaluate the IOFB. Keratometry and biometry of both eyes were done. When the measurements from then injured eye were not possible or inaccurate, the fellow eye measurements were used for the intraocular lens (IOL) calculations.
In all cases, we started by placing an inferotemporal transconjunctival 23- or 25-gauge trocar. The site of entry of the FB is identified, and if not self-sealed a suture was placed (10.0 Nylon for corneal laceration and 7.0 Vicryl for scleral laceration). For IOFB with a diameter less than 2.5 mm, a 2.75 mm clear corneal incision (CCI) was used for both cataract and IOFB extractions. For IOFB with a diameter larger than 2.5 mm, a superior conjunctival peritomy and a sclerocorneal tunnel (2.75 mm) were made. When possible, we performed a continuous curvilinear capsulorhexis. The cataract extraction was done in the classic way using a phacoemulsification machine (Constellation Vision System, Alcon Laboratories, Inc, Fort Worth, Texas) before the vitreoretinal procedure. If the posterior capsule remained intact throughout the surgery, we continued aspiration of cortical material in the classic way, and then a posterior capsular opening was made later during the vitrectomy using the vitrector. If a breach in the posterior capsule was encountered, the removal of remaining quadrants and cortical material was done after vitrectomy, using the vitrector. Corneal or sclerocorneal tunnel was temporarily closed with a single 10.0 nylon suture. Standard 3-port pars plana vitrectomy (PPV) was performed with a 23- or 25-gauge vitreous cutter and handheld light source. If absent, posterior vitreous detachment was induced. The IOFB was made free from its attachments, then lifted up to the pupillary plane using an intraocular forceps, and then an Utrata or McPherson forcep was used to grasp the IOFB and gently remove it through the corneal/sclerocorneal tunnel (Figure 1). When needed, the sclerocorneal tunnel was enlarged to match the size of the IOFB. Endolaser and retinal endotamponade were used in cases with identified retinal break(s). Posterior chamber intraocular lens (PCIOLs) was implanted preferably in the bag when possible (single piece IOL) or otherwise in the sulcus over an intact anterior capsular rim (3-piece IOL). Corneal/Sclerocorneal tunnel was closed using 10.0 nylon sutures. The conjunctiva and sclerotomies were closed with 7.0 Vicryl sutures. The choice of primary intraoperative tamponade was made intraoperatively depending on the specific pathology of each case. Tamponade included between air, sulfur hexafluoride (SF6), and octafluoropropane (C3F8). Two milligrams of Dexamethasone and 50 mg of Cefazolin were injected subconjunctivally. Postoperatively, all patients received topical antibiotics and steroids for 4 weeks with gradual tapering. Please refer to the Supplemental Video, available online, for the full surgical procedure.
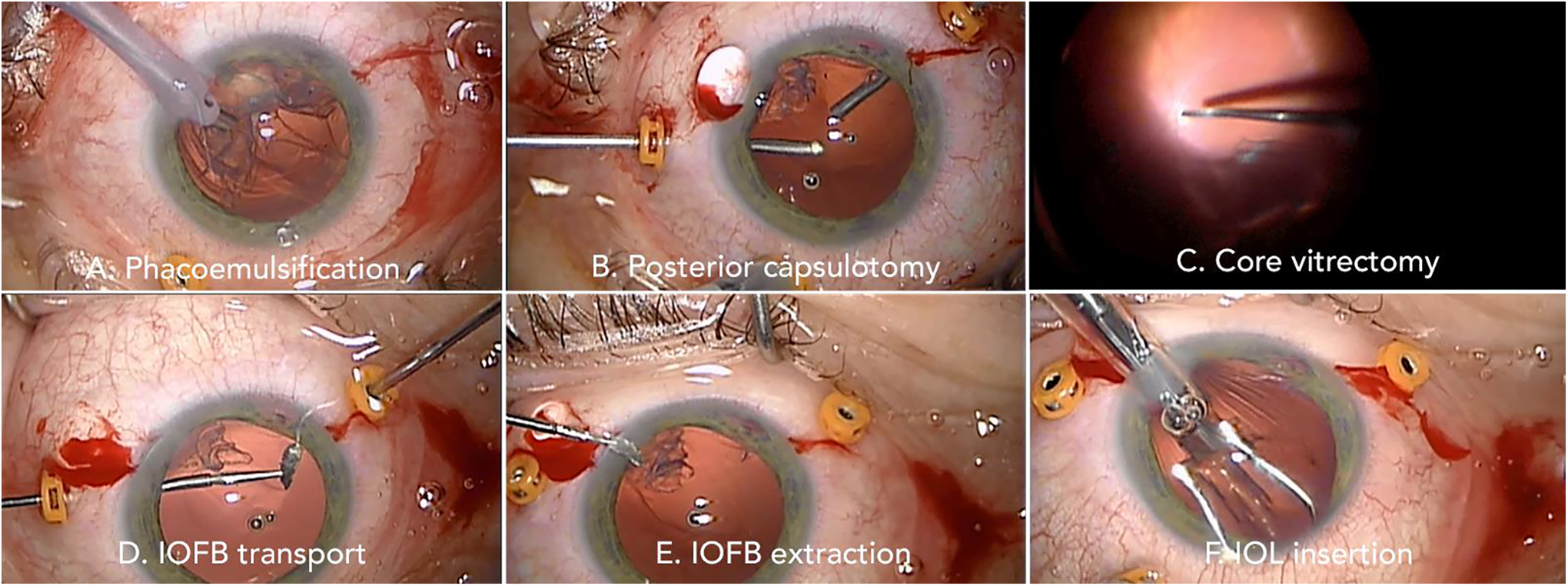
Surgical technique. (A) Phacoemulsification. (B) Vitrector-induced posterior capsulotomy. (C) Core vitrectomy with induced posterior hyaloid detachment. (D) IOFB transport from posterior segment through capsulotomy into anterior chamber. (E) IOFB extraction through the clear corneal incision. (F) Intraocular lens insertion. IOFB indicates intraocular foreign bodies. Images courtesy of G. Cordahi. Please refer to the Supplemental Video, available online, for full surgical procedure.
Results
Thirteen patients (13 eyes) were included in the study. All patients were men (100%), with an average age of 38 ± 10 years old. One patient was 12 years old and was considered pediatric. None of the patients had any relevant past ocular histories. The average follow-up period was 30 months (range, 6-185 months). On the preoperative examination, 6 (46%) of the 13 lacerations were in zone 1, 3 (23%) were in zone 2, and 4 (31%) were in zone 3. All patients with zone 1 lacerations had cataract at presentation (sectorial or total); none of patients with zones 2 or 3 had cataract at presentation. The encountered posterior segment injuries in this series included retinal tears (less than 2 clock hours) mainly in zones 2 and 3 IOFB-penetrating injuries. There were no other major pathologies including retinal detachment and choroidal effusions.
Intraocular foreign bodies were removed successfully in all operated eyes using the abovementioned surgical technique. Importantly, the IOFB was extracted through the corneal or sclerocorneal tunnels without enlarging the sclerotomies. All IOFBs were metallic in nature, and their sizes ranged from 2 to 7 mm. All operated eyes required intraoperative tamponade: 7 (54%), 3 (23%), 2 (15%), and 1 (8%) received air, C3F8, SF6, and silicone oil tamponade, respectively. Posterior chamber IOLs were inserted in the bag or in the sulcus depending on intraoperative findings and surgeon preference. Seven IOLs were inserted in the bag (54%) and 6 (46%) were inserted in the sulcus. There were no intraoperative complications noted.
Postoperative best-corrected visual acuity (BCVA) was recorded at each follow-up visit. In regard to the final BCVA outcomes, 4 (67%) of 6 patients in zone 1 had a BCVA equal to or better than 20 of 25. In zones 2 and 3, 3 (100%) of 3 and 2 (50%) of 4 had a final postoperative BCVA equal to or better than 20 of 25, respectively. In zone 1, when considering all patients, the VA improvement postoperatively was not significant (P = .9), but 4 (67%) of 6 patients gained more than 1 line of BCVA. In zone 2, the VA improvement was significant (P = .04) and 3 (100%) of 3 patients gained at least 1 line of BCVA (average of 5 lines improvement). In zone 3, the VA improvement was not significant (P = .7), but 3 (75%) of 4 patients have gained at least 1 line of BCVA.
During the follow-up period, there were 3 (23%) postoperative complications of recurrent rhegmatogenous retinal detachment (RRD) that occurred within the first postoperative year. One patient developed a macular hole (MH) 2 weeks postoperatively.
Patient 1 was a 12-year-old male who had a zone 1 injury with 20 of 50 vision at presentation. He had a PCIOL implanted in the bag, and silicon oil was used as tamponade. He had a macula ON RRD at 1 week postoperatively. A recurrent RRD with grade C5 PVR occurred 2 years postoperatively. The final VA for this patient was CF.
Patient 2 was a 40-year-old male who also had a zone 1 injury and presented with 20 of 80 vision. He had PCIOL insertion in the bag and C3F8 gas tamponade. Multiple corneal sutures were used to seal the corneal wound. He had a macula off RRD at 1-month postoperatively with grade C1 PVR. A secondary procedure was performed consisting of PPV and silicon oil injection. Three months after the second procedure, the patient developed an epiretinal membrane (ERM). The final BCVA dropped to CF.
The third patient with a recurrent RRD is patient 6, who presented with a zone 3 laceration and preoperative BCVA HM. He received a PCIOL in the sulcus and C3F8 tamponade. Four corneal sutures were placed, and intraoperative examination revealed nasal retinitis sclopetaria. The patient subsequently had a macula off RRD with grade 3 PVR 6 weeks postoperatively. A secondary procedure consisting of PPV with silicon oil tamponade was done. At 6 months postoperatively, silicon oil was removed, and the final outcome was favorable with a BCVA improvement to 20 of 150.
The last postoperative complication was the formation of an MH 2 weeks postoperatively in patient 3. This patient was a 44-year-old man with a laceration in zone 3 and a 20 of 20 BCVA at presentation. He received a PCIOL in the bag and SF6 gas tamponade. Office fluid-SF6 exchange was carried out, and MH was successfully closed after 2 weeks. At 2 years, the patient developed cystoid macular edema and was treated with intravitreal steroid injections. His final BCVA was 20 of 150.
We did not encounter any problem related to IOL insertion intraoperatively including IOL drop or subluxation. This is likely due to the size of the posterior capsulotomy which did not exceed 3 to 4 mm, just enough to allow the passage of IOFB. Additionally, during the follow-up period, no patient presented with a subluxed IOL, thus confirming the adequate adhesion between the IOL and the remaining posterior capsule.
Discussion/Conclusions
In North America, most surgeons perform a single surgical intervention, usually within 24 hours of presentation, to both remove the IOFB and ensure globe integrity. When the access to vitreoretinal surgeon is limited, it is acceptable to use a 2-step approach in which the globe is repaired for structural integrity followed by a delayed PPV to remove the IOFB. In fact, 18% to 41% of open globe injuries due to IOFB require a total of 3 procedures. 6 –10
Currently, there appears to be no consensus on whether primary cataract removal should be performed during the initial wound repair or later as a secondary procedure. Whether primary or secondary cataract removal is performed, concomitant IOL implantation is often performed at the time of surgery should anatomy permit. IOL insertion is usually needed, as aphakia resulting from cataract extraction is often difficult to manage. 24 However, this remains controversial, and secondary IOL implantation could decrease the risk of complicated implantation during an emergency operation. Postoperatively, secondary implantation could reduce the risk of infection after closure of the primary open wound. 16 In fact, Andreoli et al reported a lower rate of endophthalmitis in OGI with secondary IOL implantation. 25 The factors associated with increased risk of endophthalmitis following penetrating trauma are retained IOFB. Delay in wound closure of >24 hours, injury in a rural setting and ruptured lens capsule. 26 However, there seems to be a lower incidence of traumatic endophthalmitis with metallic IOFB compared to vegetable matter for instance. 27 –29 This is likely due to the IOFB relative sterility conferred from the high-speed velocity following metal-on-metal injury and the resulting high impact temperature upon entering the eye. Perhaps primary IOL implantation can be considered in selected cases of metallic IOFB-induced OGI.
Combining cataract extraction with the primary PPV for IOFB removal can be considered in selected cases of IOFB-induced OGI. In this study, we report the postoperative visual outcomes and ocular complications after primary combined PPV and phacoemulsification in patients with posterior segment IOFB removed via the anterior chamber without enlarging preexisting sclerotomies. We believe that a primary combined single procedure allows better retinal visualization and eliminates the need for an additional operation, especially when there is lenticular damage. In fact, cataract formation is a common complication of ocular lacerations due to IOFB. 15 –17 Traumatic cataracts do interfere with retinal visualization during surgery, and therefore a primary combined procedure could be beneficial. In addition, cataract formation remains one of the most common complications of PPV, with cataract progression occurring in 80% to 100% of patients after 2 years. 30 Compared to lensectomy and extracapsular cataract extraction, phacoemulsification is the method of choice for lens removal due to smaller incision size with less induced astigmatism as well as lower risk of hypotony and wound leak. 31,32
Our surgical technique is safe, effective, and with very promising functional prognostic benefits in selected IOFB cases. In our study, VA improved in 10 (77%) of 13 cases over the 30-month follow-up period. Specifically, 69% of patients had a final BCVA equal to or better than 20 of 25 (Figure 2). Interestingly, 67%, 100%, and 50% of patients sustaining penetrating injuries in zones 1, 2, and 3, respectively, had final BCVA of 20 of 25 and better (Table 2). Despite the significant corneal damage in zone 1, good VA outcomes were achieved. Compared to the large reviews of ocular trauma that stated VA outcomes of <20/70 in 70% and <20/200 in 25% of their cases 12,13 , our study yields better results. The risk factors identified by Kuhn et al for poor outcomes following IOFB injury included significant posterior segment pathology, age over 60, and poor VA at presentation. 12 The difference in the results is likely attributed to the extent of injury and baseline factor discrepancies between the studied populations. In our study, patients were selected on the basis of having minimal posterior segment pathology and theoretically a better functional visual prognosis. Another important factor to consider was the phakic status which is generally associated with a younger patient population. The latter was correlated with a better functional visual outcome in IOFB-induced OGI as per Kuhn et al. 12 Other studies looking particularly at the combined procedure also reported superior VA outcomes compared to the 2 abovementioned studies, thereby suggesting an additional potential benefit to the CE/IOL component of the surgery. Lam et al reported a best-corrected VA of 20 of 40 or better in a series of 4 (100%) patients undergoing combined procedure for IOFB removal. 31 Additionally, Batman et al reported 25% of patients with 20 of 30 or better and 76% of patients with a VA of 20 of 200 or better, in a case series of 17 patients also undergoing a combined procedure. 33 In that study, 53% of patients presented with HM vision while in our study only 2 patients had HM vision (15%), a difference in a baseline characteristic that could explain the much better result we obtained with the same technique.
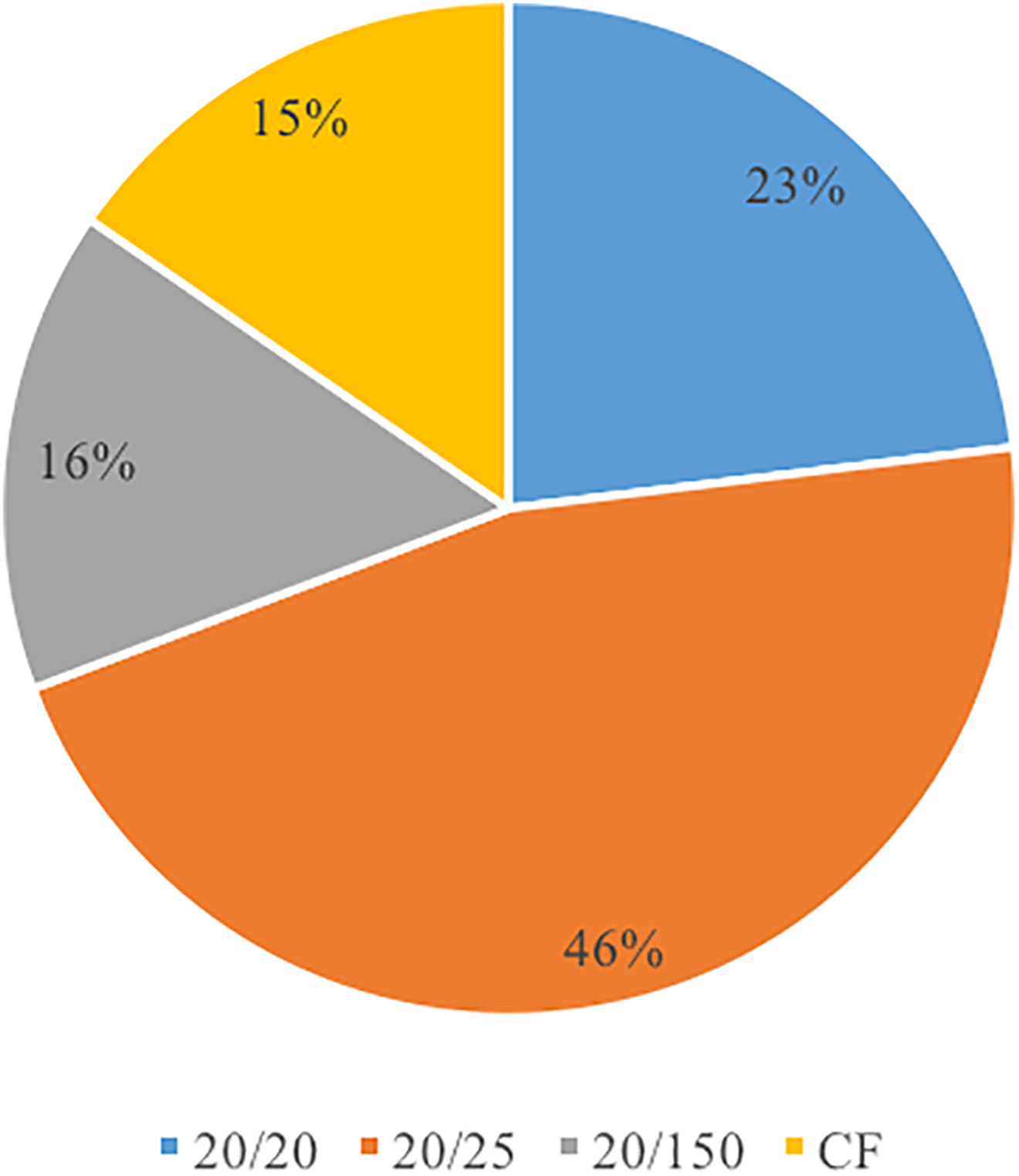
Pie chart of the final BCVA for all zones combined. BCVA indicates best-corrected visual acuity.
Enrolled Patients’ Demographics, Preoperative and Postoperative Clinical Data.
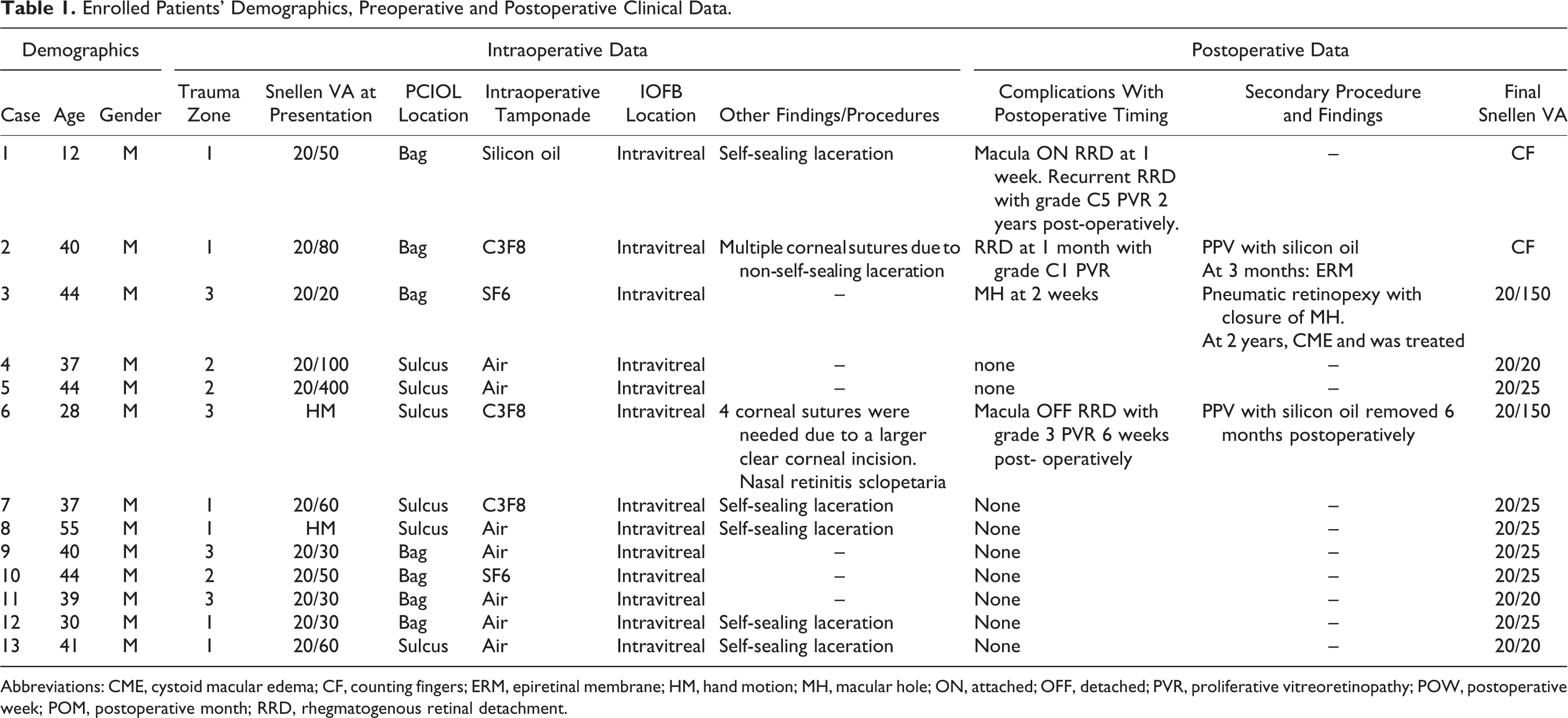
Abbreviations: CME, cystoid macular edema; CF, counting fingers; ERM, epiretinal membrane; HM, hand motion; MH, macular hole; ON, attached; OFF, detached; PVR, proliferative vitreoretinopathy; POW, postoperative week; POM, postoperative month; RRD, rhegmatogenous retinal detachment.
Table Summarizing the Results of the Statistical Analysis.
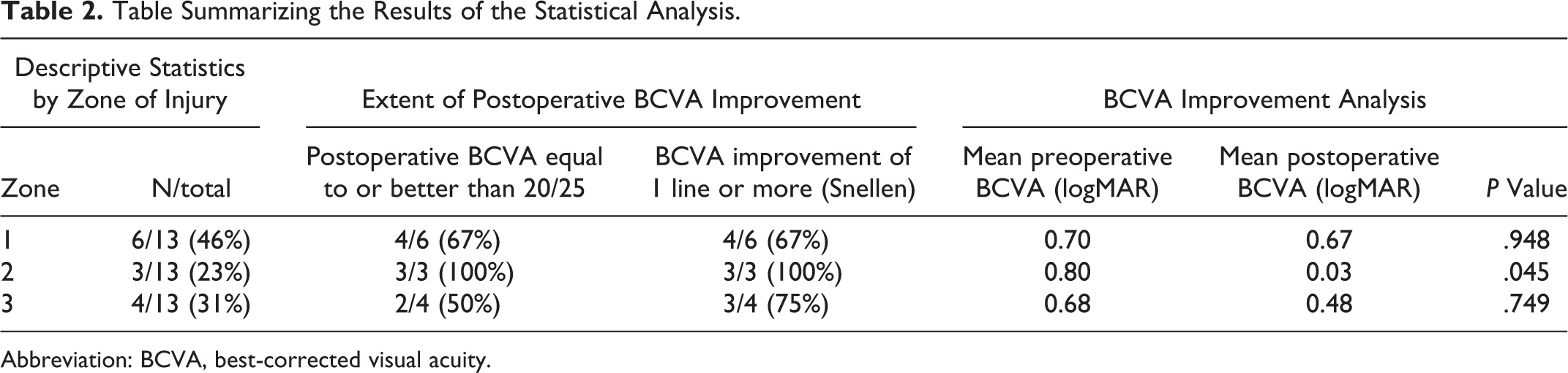
Abbreviation: BCVA, best-corrected visual acuity.
Several case series studied the clinical outcomes following combined procedure which was reported to be safe and effective with good visual outcomes. A combination procedure can prevent the excessive development of inflammatory synechiae resulting from repeated interventions, vascularization, and hyphema from an injured lens/iris and allows earlier rehabilitation and better visual outcomes. 34 It is well-documented that the number of surgical interventions is predictive of visual outcomes. According to Groessl et al, 90% of patients will obtain good ambulatory visual outcomes when only a single procedure is performed. 35 Furthermore, the intraoperative complications noted might be as likely to occur during phacoemulsification or vitrectomy when performed alone. 33,36,37 Due to the real higher rate of postoperative complications with increasing number of interventions, we believe that minimizing these will result in better functional visual outcomes especially in eyes with zones 2 and 3 penetrating injuries. Compared to penetrating injuries in zone 1, those in zone 3 are significantly more prone to poorer VA, developing RRD and phthisis according to studies by Feng et al 38 and Stryjewski et al. 39 Furthermore, compared to a sequential PPV followed by phacoemulsification, Muselier et al showed that primary combination PPV and phacoemulsification and sequential surgery resulted in equivalent functional and anatomic results. 40 Combined surgery was associated with a shorter delay for visual recovery in those same patients operated for ERM/MH. Our cohort of patients is comparable to the one studied by Muselier et al in the sense that the posterior segment pathology is minimal. In view of minimizing postoperative complications including those associated with enlarged sclerotomies for the removal of IOFB, we elected to perform phacoemulsification in order to extrude the IOFB via the posterior capsulotomy.
The development of RRD is associated with scleral entry wound, size of IOFB, location of IOFB, and preoperative detachment. 41 In our study, all eyes had IOFB <7 mm allowing removal from the CCI without enlarging sclerotomies. Hence, the rational for a combined single-step approach included also minimizing the rates of PVR formation and posttraumatic endophtalmitis. Nonetheless, 3 (23%) patients developed recurrent RRD associated with PVR in the first postoperative year. Proliferative vitreoretinopathy–associated recurrent RRD are not uncommon in the context of posterior segment IOFB and post-PPV. Compared to patients with primary RD who develop PVR in 8% to 10% of cases, the rate of PVR formation post open glove injuries can reach 40% to 60%. 42 The higher incidence of PVR post open globe injuries is likely due to a more vigorous inflammatory reaction. Those eyes with PVR postoperatively have worst VAs, primarily due to subsequent recurrent RD and retinal/subretinal fibrosis. 43 In our study, 2 patients with PVR had their BCVA significantly worsened to CF within the first year post primary trauma repair (Table 1). Chiquet et al, who studied the prognostic factors influencing visual outcomes in PPV with FB removal alone, reported 28% incidence of postoperative RRD, with this complication being the largest single cause of blindness. 15 It is worth mentioning, however, that the PVR formation rate in our study is almost half of that reported in open globe injuries; this finding consolidates the prognostic importance of the number of surgical interventions performed to repair open globe injuries.
None of our patients developed hypotony, vitreous hemorrhage, or endophtalmitis postoperatively. However, combined PPV and phacoemulsification for the removal of posterior segment IOFB has been reported to result in other significant complications. Batman et al reported 2 cases of massive retinal fibrosis and hypotony and 1 case of RD in their 17-patient series of similar combined procedures. 33 Similarly, Vatavuk et al reported 2 cases of RD at 1-month as well as 2 separate cases of retinal fibrosis and endophthalmitis in their 16-patient series study. 32
Our study has some limitations. A single surgeon in a tertiary care center operated on all patients. The reproducibility of the surgical technique cannot be generalized to patients in other settings. The study only included consecutive patients in which the surgeon perceived the suitability of this technique, excluding many nonsuitable patients. Furthermore, the small sample size could not identify potentially less common intraoperative and postoperative complications.
We reported the postoperative visual outcomes and ocular complications after primary combined PPV and phacoemulsification for posterior segment IOFB that was removed via the anterior chamber without enlarging preexisting sclerotomies. To our knowledge, this is the first and largest series using this technique. Our technique offers considerable advantages, namely, 1/ a lower risk of retinal complications including hypotony, vitreous incarceration, and retinal tear/detachment as there is no need for enlarging sclerotomy ports, 2/ significant less overall operative times and patient discomfort as it is a 1-step procedure, and 3/ better overall visual rehabilitation and recovery time. We recommend using this technique in cases of IOFB with good visual potential (absence of severe posterior segment pathology, severe uveal prolapse through entrance wound, severe iris dialysis and giant tears, significant globe disorganization, signs of intraocular infection, and evidence of RD on computed tomography scan or ultrasonography). This technique will allow conserving globe integrity without additional sclerotomies.
Footnotes
Ethical Approval
The local research department confirmed that no ethical approval was required given the retrospective nature of the study, as there was no deviation from the usual standard of care.
Statement of Informed Consent
Direct written patient consent was not obtained for data collection and analysis, as such nonidentifying information has been included.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.