
Abstract
Purpose:
We describe 2 retinopathy cases with a possible herpetic association.
Methods:
Presentation, workup, and clinical course of 2 patients were reviewed and compiled.
Results:
Patients presented with no to mild symptoms and multiple bilateral funduscopic yellow hypopigmented lesions corresponding to outer retinal thickening with submacular fluid on optical coherence tomography. Findings mimicked central serous chorioretinopathy but lacked any leakage or pooling on angiography. Systemic workups were negative and our patients had anatomic resolution following a treatment course of oral valacyclovir.
Conclusion:
These cases suggest a possible viral herpes zoster prodrome in some patients who present with acute exudative polymorphous vitelliform maculopathy.
Introduction
Viral infections can result in a variety of ocular manifestations. Pathology in the posterior segment can present with uveitis, retinitis, or chorioretinitis. 1 Identified viral associations include cytomegalovirus, herpes simplex, and varicella-zoster viruses in acute retinal necrosis (ARN) and posterior outer retinal necrosis (PORN); 1 and hepatitis, enterovirus, and coxsackie virus in acute retinal pigment epitheliitis (ARPE) or Krill disease. 2,3
Acute exudative polymorphous vitelliform maculopathy (AEPVM) is a separate, rare entity initially described by Gass et al in 1988 in which patients presented with bilateral multifocal yellow-white lesions that corresponded to blister-like areas of serous retinal detachment. 4 AEPVM was previously described in the literature as a paraneoplastic syndrome predominantly in cases of cutaneous and choroidal melanoma and carcinoma, but has also been associated with nonparaneoplastic case reports of coxsackie virus infection and Lyme disease. 4 -8
Recently, Barbazetto et al published a comprehensive series on idiopathic AEPVM as a rare disease of unknown origin, distinguishing it from heritable Best disease and paraneoplastic polymorphous retinopathy. 9 To our knowledge, we present the first cases of AEPVM that may have associations with herpes zoster.
Case 1
An otherwise healthy 83-year-old Caucasian man presented with 4 months of decreased vision and photopsias in the form of “blue specks.” His ocular history was significant for open-angle glaucoma treated with daily latanoprost. Best-corrected visual acuity was 20/40 OU. Anterior segment exam was remarkable for minimal cataracts. Dilated ophthalmoscopy revealed creamy, deep, yellow lesions with mild diffuse hyperpigmentation in the macula bilaterally (Figure 1, A and B). There was no evidence of inflammation, and no retinal whitening, hemorrhage, or masses. His medical history was significant for basal cell and cutaneous melanoma that was completely excised nearly a decade prior. Review of systems was negative. He was previously treated with prednisolone and ketorolac eye drops without improvement.
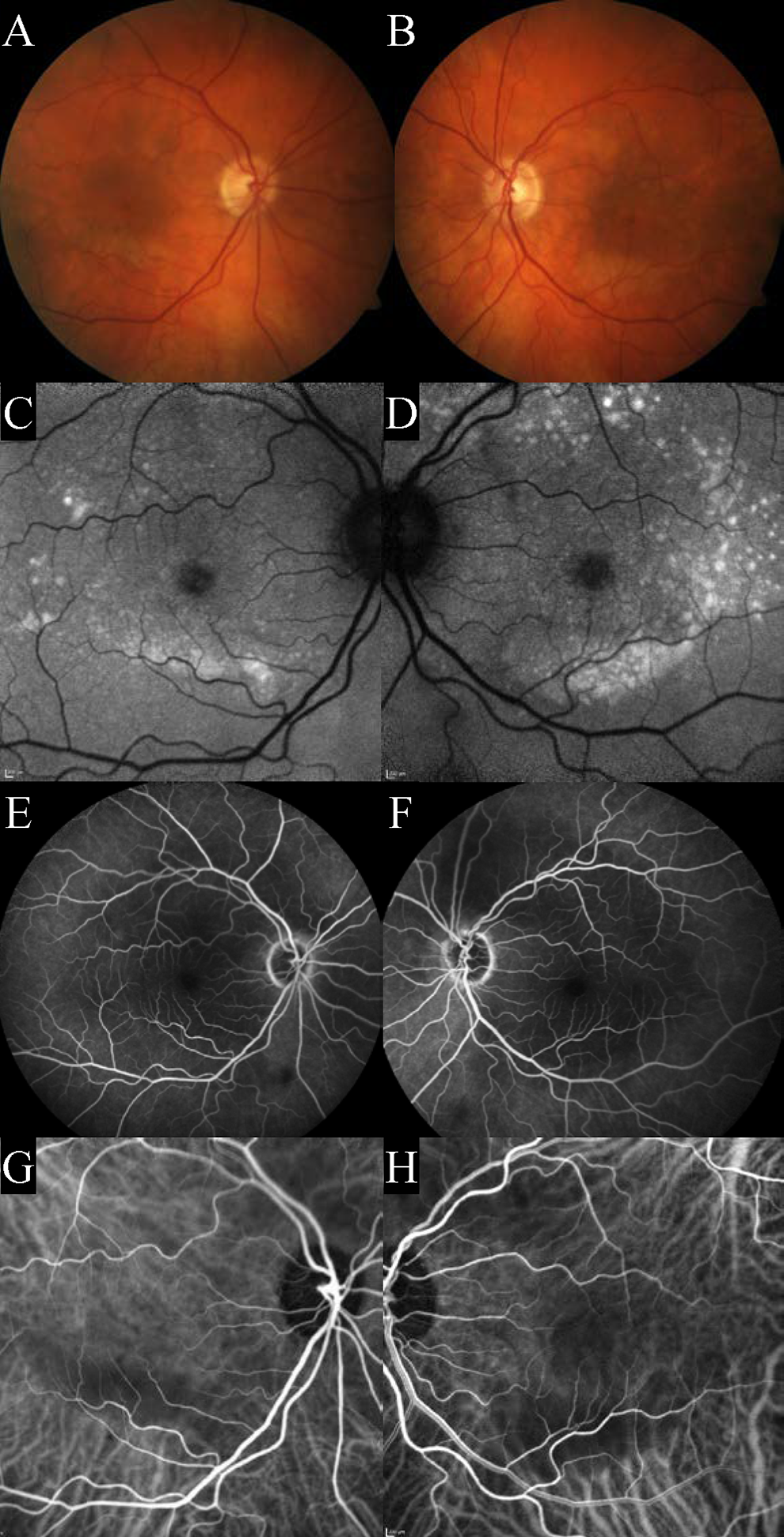
Initial presentation. (A, B) Color fundus photographs and (C, D) corresponding fundus autofluorescence, show distribution of confluent punctate hyperautofluorescence of right and left eyes. (E, F) Midarteriovenous-phase fluorescein angiography shows blockage of fluorescence corresponding to the creamy yellow lesions and areas of retinal thickening/subretinal fluid in the macula and around the temporal arcades without leakage, pooling, or staining. (G, H) Indocyanine green angiography similarly shows blockage without hot spots.
Optical coherence tomography (OCT) revealed subfoveal fluid and atypical outer retinal thickening in both eyes that spanned the macula from arcade to arcade (Figure 2A). Axial lengths were 24.78 and 24.6 mm in the right and left, respectively. B-scan showed no evidence of choroidal thickening or masses. There was blocked fluorescence from the subretinal fluid on fluorescein angiography (FA) and indocyanine green angiography (Figure 1, C-H). Electrooculogram showed borderline Arden ratios of 1.63 in the right eye and 1.96 in the left eye.
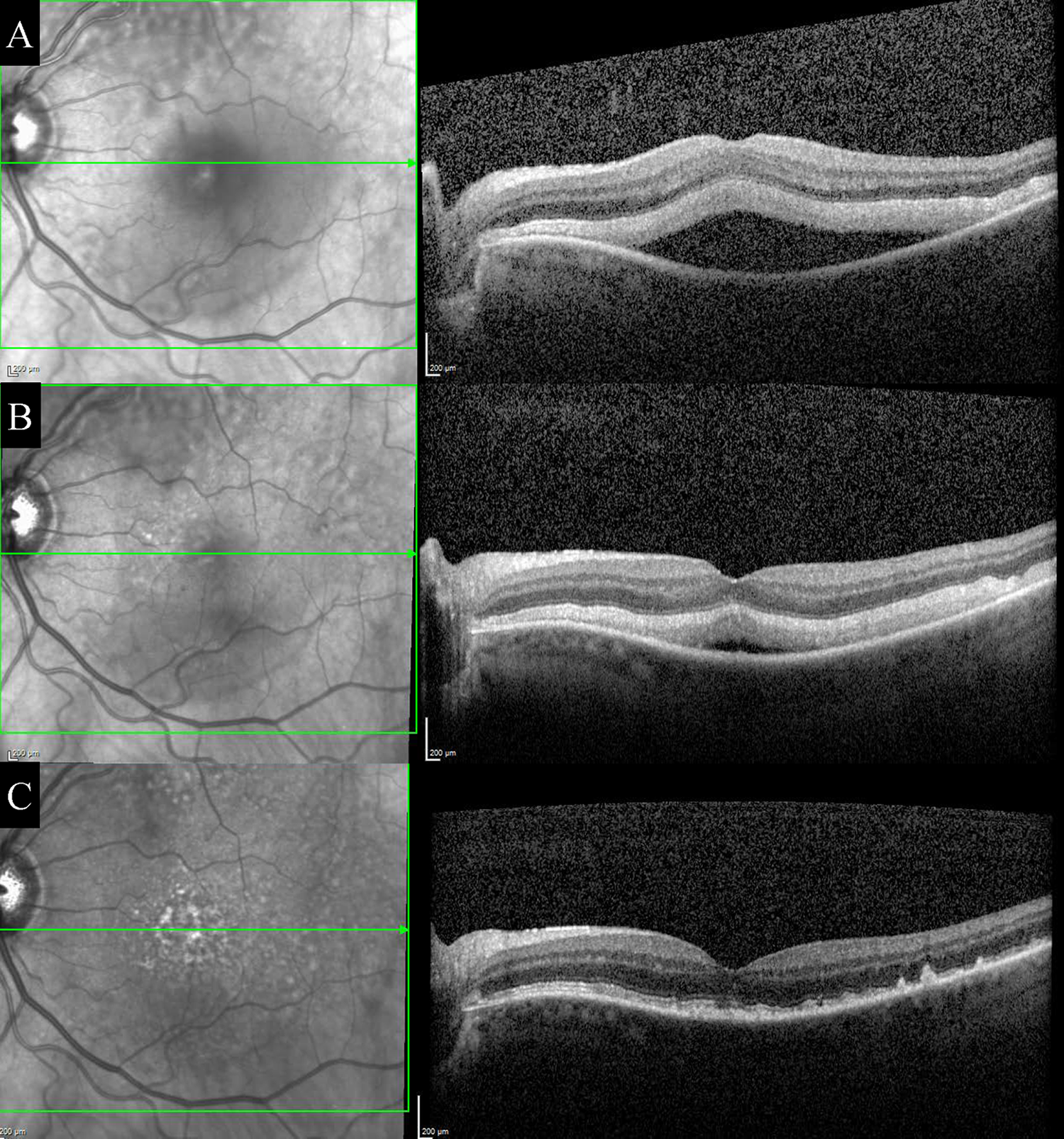
Optical coherence tomography (OCT) of representative left eye through the fovea at initial presentation and follow-up visits. (A) Initial OCT shows significant outer retinal thickening and presence of subretinal fluid. (B) There is interval improvement in the amount of subretinal fluid at month 1 follow-up with less thickening of the outer retinal layers and less subretinal fluid, and (C) complete resolution of fluid and thickening at month 2 with only moderate residual disorganization of the outer retina and disruption of the ellipsoid zone.
An extensive workup was unremarkable and included the following: syphilis, sarcoidosis, tuberculosis, chest computed tomography, brain and orbit magnetic resonance imaging with and without contrast, and cerebrospinal fluid analyses including cell count, protein, glucose, cytology, and flow cytometry. Observation was recommended.
One month later, his vision improved to 20/32 in the right eye but remained unchanged in the left eye. There was interval improvement in the amount of subretinal fluid on OCT in both eyes, although the outer retinal thickening remained unchanged (Figure 2B). On questioning, the patient disclosed that 1 week earlier, he had developed shingles on his trunk and had started oral valacyclovir 1000 mg 3 times a day.
The patient was monitored as he completed his 1-week course of valacyclovir. At follow-up 2 months from presentation and 4 weeks after completing valacyclovir, his vision had improved to 20/32 OU with resolution of photopsias and subretinal fluid, as well as significant improvement of outer retinal anatomy on OCT (Figure 2C). This improvement was quite remarkable and prompt following oral antiviral therapy.
Case 2
A 75-year-old Caucasian male was referred for bilateral asymptomatic macular lesions. He had a medical history of cutaneous melanoma with positive inguinal lymph nodes status postcomplete lesion excision and remained on ipilimumab therapy, but was to date disease free without evidence of solid organ metastasis. His vision was 20/25 OD and 20/30 OS. Intraocular pressures were normal and anterior segment exam was significant only for moderate cataracts. Fundus exam revealed bilateral multiple circular yellowish lesions with OCT through the lesions showing outer retinal thickening and subretinal fluid (Figure 3, A-C). FA revealed no leakage or hot spots and fundus autofluorescence showed mild hypoautofluorescence corresponding to multiple focal areas of subretinal fluid with adjacent areas of punctate hyperautofluorescence.
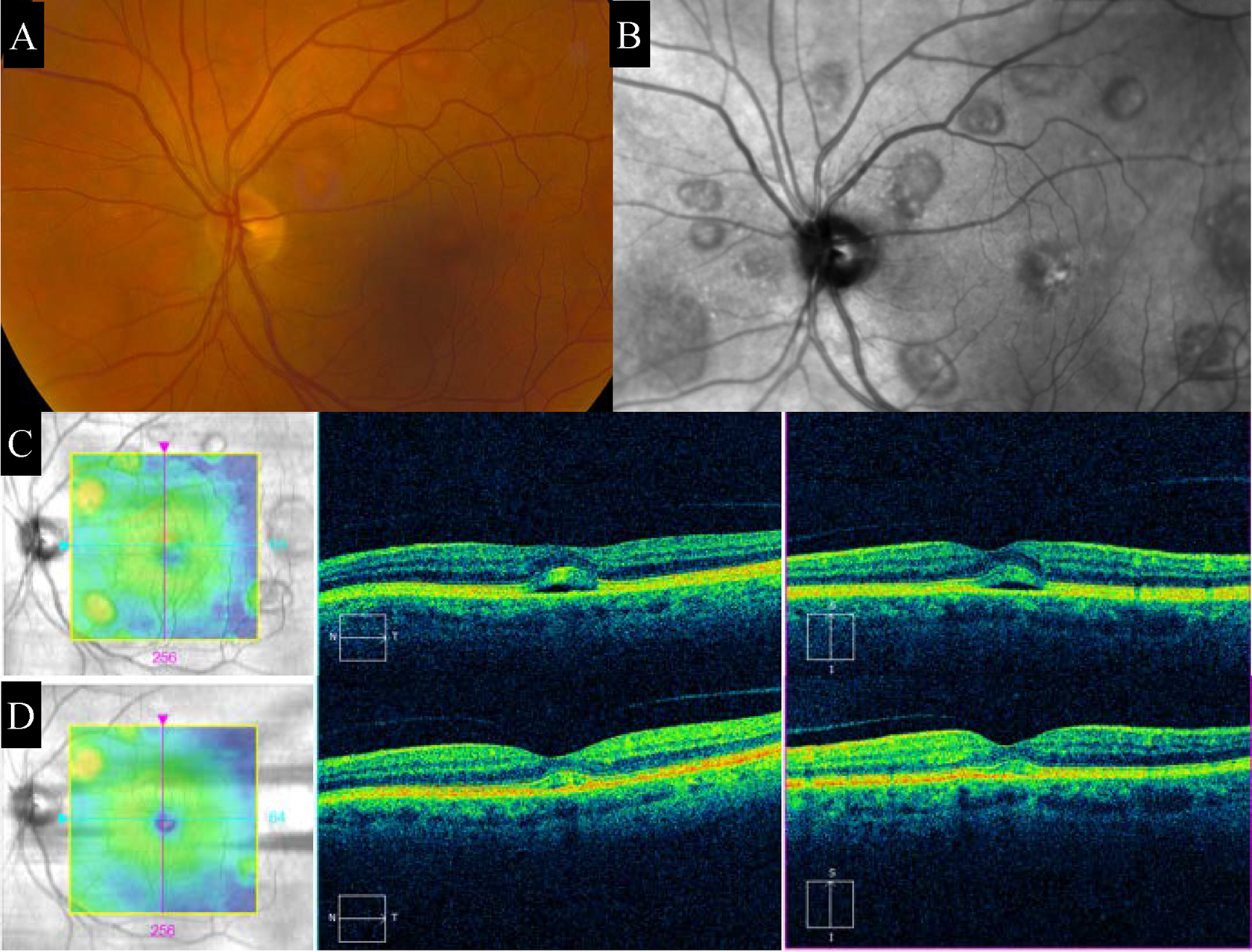
Representative color fundus photographs of the left eye showing (A) multiple yellow, round, hypopigmented retinal lesions with (B) corresponding fundus autofluorescence depicting punctate hyperautofluorescence in areas of hypoautofluorescence. Optical coherence tomography through foveal lesion shows (C) initial outer retinal thickening and presence of subfoveal fluid that (D) improves after treatment with valacyclovir at month 3.
As part of the initial workup in this patient with a history of malignancy, antiretinal antibodies were pursued and returned positive. He was followed closely but did not develop subacute or acute rapid progressive vision decline that would have suggested a paraneoplastic autoimmune retinopathy. During his follow-up after no improvement at 1 month, the patient was placed on oral valacyclovir 1000 mg 3 times a day for 6 weeks while remaining on his other medications including ipilimumab therapy. Three months following completion of antiviral therapy, the patient was found to have normalization of visual acuity in both eyes to 20/25 with concurrent improvement of subretinal fluid pockets on OCT (Figure 3D).
Discussion
Similar to reported cases of idiopathic and paraneoplastic AEPVM in the literature, our patients presented with no to mild visual complaints and were found to have yellowish lesions that corresponded to pockets of subretinal fluid with bilateral outer retinal thickening. 5,6 There was no retinal whitening, necrosis, vasculitis, or vitritis suggestive of ARN or PORN, no clinical similarity or OCT findings typical of ARPE, and no leakage on angiographic studies and/or thickened choroid typical of central serous chorioretinopathy (CSCR). 10 Interestingly, both patients were on chronic latanoprost in both eyes for glaucoma treatment, which has been associated with CSCR-like pathology that improves following cessation of topical prostaglandin. 11 -14 However, unlike our cases reported here, these cases documented leakage on FA and did not report outer retinal thickening. Our patients improved following antiviral therapy without cessation of their prostaglandin medication.
Visual improvement and resolution of serous fluid occurred at month 2 and month 4 following initial evaluation in our 2 patients. The timing of resolution falls within the self-resolution period reported in the case series by Barbazetto et al of 12 patients with idiopathic AEPVM wherein time from first presentation to resorption of subfoveal serous detachments was between 2 and 5 months. 9 It is possible that our patients had a self-limited disease and that apparent improvement on valacyclovir was simply coincidental. It is also possible, however, that antiviral treatment hastened recovery. This is the challenge to knowing the relationship between treatment and response in a condition that may be self-limited. More information is needed in understanding AEPVM and the possibility of a viral prodrome. Resolution of symptoms in our patients treated with antiviral therapy may provide a possible low-risk treatment option with a low side-effect profile to consider in patients with refractory symptoms.
A number of cases of paraneoplastic AEPVM associated with melanoma in the literature highlight the need to consider malignancy in individuals presenting with AEPVM. Barbazetto et al reminds us of the need for malignancy surveillance in patients presenting with AEPVM to distinguish idiopathic cases from paraneoplastic cases. 9 In that large series, the authors suggest that a possible way to distinguish between the 2 categories of patients is a known malignancy diagnosis. 9 While paraneoplastic syndromes may present with a self-limited course, most paraneoplastic cases are either refractory to treatment or responsive only to anticancer or immunomodulating therapies. A retrospective case series of 5 patients with paraneoplastic AEPVM highlights how sick these patients generally are: Within a mean follow-up time of 5 months, 3 of the 5 patients had died from metastasis. 15 At 5 months of follow-up in the surviving 2 patients with paraneoplastic retinopathy, 1 patient exhibited resolution of lesions, while the other patient had findings similar to those at initial presentation. 15
Both of our patients had a history of melanoma, which suggests a possible paraneoplastic etiology to their presentation; however, their clinical course is less typical of an insidious paraneoplastic etiology. Our patient in Case 1 had a remote history of a treated cutaneous melanoma in situ without evidence of current active melanoma, and our patient in Case 2 was being treated for cutaneous melanoma with positive lymph nodes status postsurgical excision without evidence of solid organ metastasis.
To date, our 2 patients remain without evidence of active disseminated malignancy. What is unique in our case series is the temporal occurrence of a viral infection (shingles in Case 1) and improvement of clinical symptoms and retinal findings on OCT with antiviral treatment in both patients without recurrence following treatment.
The original cases of AEPVM described by Gass in 1988 were preceded by a history of recent viral illness, leading the authors to postulate that the likely etiology was immune related via molecular mimicry. 4 This hypothesis is supported by findings of positive antiretinal and antiretinal pigment epithelium (anti-RPE) antibodies identified in cases of AEPVM (including our Case 2), suggesting an autoimmune mechanism in which the inciting cause may be infectious or neoplastic. 5,16
Although the exact etiology remains to be discovered, the pathophysiology has been suggested to be RPE dysfunction leading to the accumulation of shed photoreceptor segments and serous detachment of the neurosensory retina. 5,17 This accumulation of fluorophores in the subretinal space, instead of lipofuscin in the RPE, has been proposed to be the reason for the areas of hyperautofluorescence seen on imaging. 17
Current AEPVM treatment paradigms remain poorly understood. Close monitoring may be the first consideration, given the high rates of spontaneous resolution. 9 Other case reports have suggested improvement with intravitreal aflibercept or intravitreal triamcinolone. 9,18 While we cannot prove causation by a herpes virus etiology and while this disease entity may be self-limited in select individuals, the clinical history and improvement of ocular symptoms and imaging findings of our 2 patients on herpes zoster treatment suggest a possible zoster viral association to consider in patients presenting with AEPVM that has not previously been described. Antiviral therapy may be an additional consideration for these patients.
Careful history-taking and assessment for active malignancy must continue to be performed in patients presenting with AEPVM. Future studies are necessary to further investigate both paraneoplastic and nonparaneoplastic AEPVM cases and to better understand the pathophysiology underlying these mechanisms.
Footnotes
Ethical Approval
Our case series was exempt from formal review by the Duke Institutional Review Board because of an institutional decision that case reports without identifying patient information do not constitute research.
Statement of Informed Consent
We obtained verbal consent from our 2 patients to share their stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.