
Abstract
Purpose:
The purpose of this work is to report an association between intravenous immunoglobulin (IVIG) infusions and the development of bilateral ischemic optic neuropathy.
Methods:
A case report is described.
Results:
A 76-year-old male receiving IVIG infusions developed loss of vision in the left eye and was diagnosed with ischemic optic neuropathy. Two months later, he developed another episode of ischemic optic neuropathy in the contralateral eye. The investigation for giant-cell arteritis, vasculopathy, and infiltrative processes was negative. The patient had minimal improvement in visual acuity over several months of follow-up.
Conclusions:
Bilateral ischemic optic neuropathy was likely caused by IVIG infusion in this case, given the temporal relationship and the negative workup for other risk factors.
Introduction
Intravenous immunoglobulin (IVIG) infusions rarely have ocular side effects. Although uncommon, infusions have been noted to cause adverse side effects, such as thromboembolic events including myocardial infarction, stroke, deep-vein thrombosis, and pulmonary embolism. 1 A patient with Miller Fisher syndrome was treated with IVIG, and subsequently developed transient confusion and reversible blindness. The bilateral occipital lobe changes seen on brain MRI were secondary to cerebral infarction, which may have occurred because of hyperviscosity secondary to IVIG. 2 There have also been reported cases of central retinal vein occlusion occurring after IVIG infusion. 3 No previous case has correlated IVIG infusions with bilateral ischemic optic neuropathy.
We report a case of a 76-year-old man who developed bilateral ischemic optic neuropathy following IVIG infusions.
Case Presentation
A 76-year-old man with no ocular history was receiving monthly IVIG for chronic obstructive pulmonary disease. Two days after his fourth infusion, the patient developed acute blurry vision in the left eye and was referred to a vitreoretinal surgeon. At initial examination, the left eye was 2/200 on the E-card with an afferent pupillary defect. The right eye was 20/20 with a normal exam. The left optic disc was edematous with hemorrhages and the left disc was perfused with a cup-to-disc ratio of 0.2 (Figure 1). The arterioles were narrow throughout each eye. His medical history included hyperlipidemia and hypertension controlled with medications, and his review of systems was negative for the symptoms of polymyalgia rheumatica. He was diagnosed with ischemic optic neuropathy in the left eye and bilateral hypertensive retinopathy. His 81 mg daily aspirin dose was increased to 325 mg. A systemic workup was performed to rule out arteritic ischemic neuropathy and risk factors for atherosclerotic disease. Pertinent findings included a normal carotid ultrasound, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).
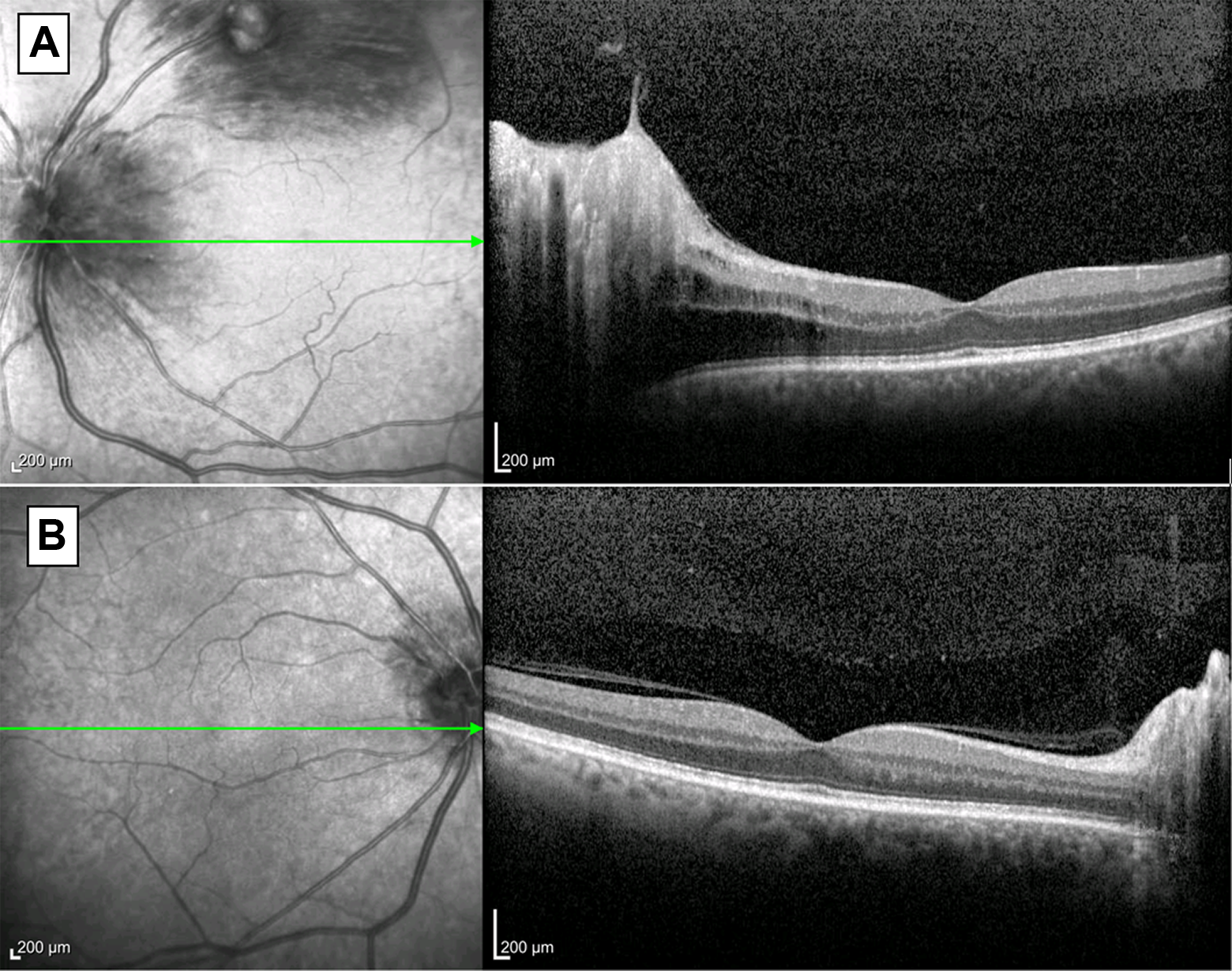
(A) Initial visit en face and B-scan optical coherence tomography demonstrating edema of the left optic nerve with macular superior temporal hemorrhage. (B) Right eye demonstrates normal optic nerve and macula.
Two months later, the patient had acute vision loss in the right eye. He had received his sixth IVIG infusion just 2 days before. Visual acuity decreased to hand motion in the right eye and count fingers at 6 inches in the left eye. The right optic disc was edematous with hemorrhages (Figure 2). Because of his profound sequential vision loss, he was admitted to the hospital and started on IV methylprednisolone. MRI of the brain and orbits was unremarkable and a temporal artery biopsy demonstrated no evidence of giant-cell arteritis (GCA). The optic disc edema was less 2 days after treatment, but the vision did not improve. He was discharged from the hospital and cautioned against receiving additional IVIG infusions without modification. At 2 weeks, the right eye was count fingers at 6 inches and the left eye was 20/400. Both optic discs were pale. His exam remained unchanged 9 months after his initial presentation.
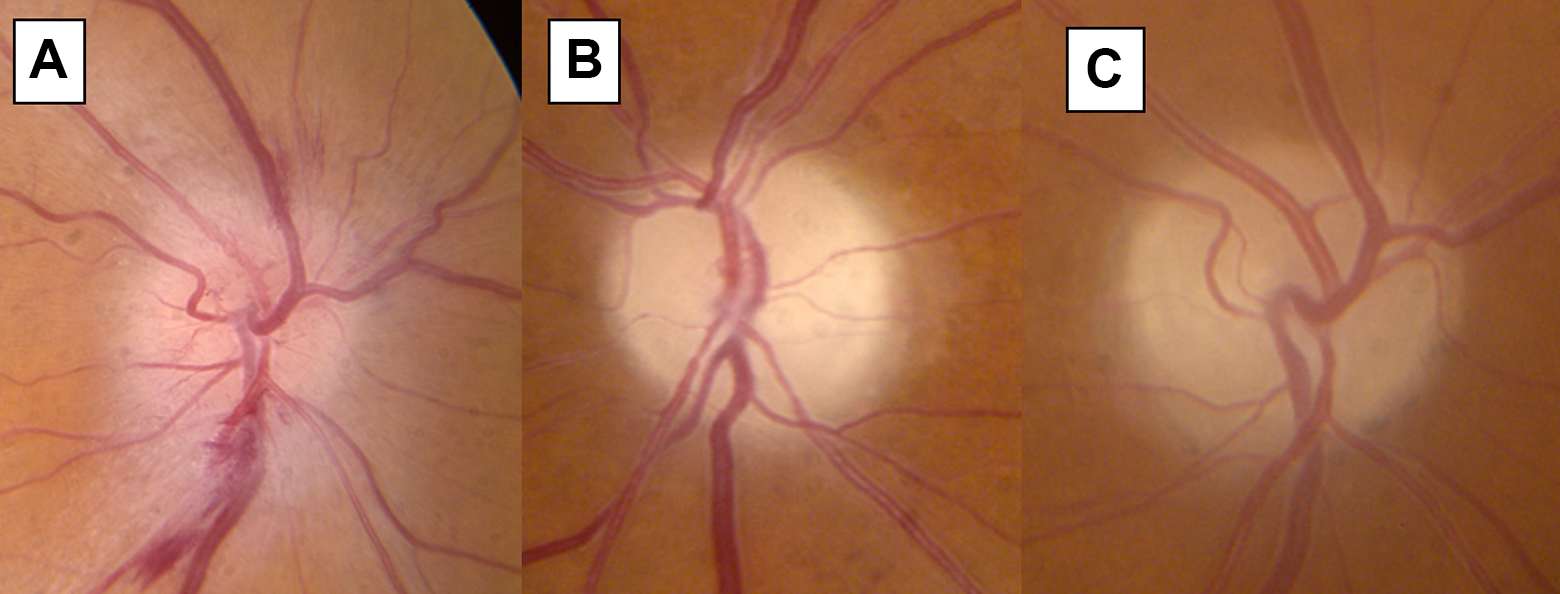
At the second follow-up, color fundus photos demonstrated (A) edema and hemorrhage of the right optic nerve, and (B) pallor of the left optic nerve. (C) Four months later, the right optic nerve also developed pallor.
Conclusion
IVIG is a sterile, purified immunoglobulin G (IgG) product manufactured from pooled human plasma; it treats a number of health conditions including primary immunodeficiency, idiopathic thrombocytopenic purpura, chronic inflammatory demyelination polyneuropathy, Kawasaki disease, HIV/AIDS, and other infections when a more specified immunoglobulin is unavailable. The exact mechanism of action of IVIG in most diseases remains unclear. It is thought to suppress inflammation by binding to receptors on antigen cells and increasing the expression of the inhibitory Fc receptor to shorten the half-life of autoreactive antibodies. While IVIG has many potential uses in ophthalmology, including its use as a treatment for neuromyelitis optica and cancer-associated retinopathy, where it has been shown to lead to a partial recovery of vision loss, it also may lead to ocular side effects, including a reversible loss of vision. 2,4
GCA is a granulomatous vasculitis that occurs in older adults. Symptoms include headaches, facial pain, and loss of vision. 5 Owing to the sequential profound vision loss in this present case, GCA was initially explored as a possible diagnosis. However, the ESR and CRP were normal, and the temporal artery biopsy was negative. It is possible that the biopsy was a false negative due to suppression effect from the IVIG. However, if this had been the case, it would be even more unlikely that GCA was the culprit. IVIG would have likely prevented the onset of GCA if it indeed could suppress the expression of inflammatory cells within the temporal artery. In fact, IVIG is most commonly used to treat autoimmune disease, making GCA an unlikely cause of the bilateral optic neuropathy.
IVIG complications of thromboembolic events, particularly in older patients, have been reported. 6 Concentration of infused IgG has been strongly correlated with viscosity of plasma and whole blood, both in vitro and in vivo, and plasma viscosity increases above normal range after IVIG infusion. A transient risk of arterial thromboembolic events occurs in patients with a hematologic malignancy on the day of IVIG infusion and in the following 24 hours. 7 High serum viscosity can impair blood flow, and in patients with cardiovascular risk factors, it has been reported to produce myocardial infarction or stroke. 8 It is reasonable to conclude the same reported thromboembolic events in other systems could affect the ophthalmic artery as well. Additionally, our patient has a history of hypertension and hyperlipidemia, which likely put him at additional risk of developing these complications.
No previous literature has demonstrated the relationship between IVIG and ischemic optic neuropathy. Anecdotally, patients have reported transient vision changes and optic nerve edema following IVIG infusion. It is important to note that it is possible that both nonarteritic anterior ischemic optic neuropathy events that occurred in our patient were due to underlying risk factors instead of the IVIG; however, we believe there is enough evidence to suggest IVIG may have played a role in this patient’s vision loss. A study involving ophthalmic screening of all patients receiving IVIG may clarify further. Studies suggest that slow infusion rate along with proper IV hydration, especially in those with vasculopathic risk factors, may decrease the risk of thromboembolic effects. 9 We suggest close monitoring for ocular side effects in those undergoing treatment with IVIG.
Footnotes
Ethical Approval
The authors have ensured that this report was written in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and that are consistent with the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use guidelines for Good Clinical Practice (GCP) and applicable regulatory requirements.
Statement of Informed Consent
No identifying information was used in the compilation of this manuscript and therefore informed consent was not necessary as deemed by the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This case report was sponsored by the Retina Research and Development Foundation (RRDF).