
Abstract
Purpose:
This study assesses the frequency of projection artifacts in optical coherence tomography angiography (OCTA) en face images and compares images before and after applying a 3-dimensional projection artifact removal (3D-PAR) algorithm.
Methods:
This is a single-center, retrospective study that included consecutive patients with any underlying diagnosis who had OCTA obtained from January to March 2017. Patients with various retinal diseases and also healthy eyes were included. All participants underwent imaging with a scan area of 3 mm × 3 mm. The 4 default en face slabs were analyzed: superficial capillary plexus (SCP), deep capillary plexus (DCP), outer retina (OR), and choriocapillaris (CC). Images were qualitatively analyzed before and after 3D-PAR by 2 independent graders.
Results:
None of the SCP images had projection artifact before or after 3D-PAR. Scans of the DCP presented projection artifact in 96.5% of the cases. After 3D-PAR, 14.7% had a complete improvement of projection artifact, 56.5% had a partial improvement, 14.1% were worse, and 14.7% presented no change. In the OR, 2.9% had projection artifact, with a complete improvement after 3D-PAR in 40%, partial improvement in 20%, and no change in 40%. Projection artifact was initially present in 97.6% of the images in the CC. After 3D-PAR, there was a complete improvement in 72.9%, partial improvement in 26.5%, and no change in 0.6%. Choroidal neovascularization (CNV) was detected in 29 eyes (17.1%), and 3D-PAR improved detection of CNV in 12 cases (41.4%).
Conclusions:
OCTA with 3D-PAR technology minimizes the appearance of projection artifacts in the DCP and CC slabs.
Introduction
Optical coherence tomography angiography (OCTA) is a transformative imaging modality that uses motion contrast to provide a noninvasive image of the retinal and choroidal vasculature. 1 Its ability to detect blood flow by motion contrast allows 3-dimensional (3D) visualization of the blood vessel network. 1 Essentially, repeated sequential cross-sectional B-scans are captured at the same location and then the relative change in signal is measured at each voxel. 2 Whereas stationary tissue structures will show little change, the intravascular flow of blood cells in the vessels will indicate movement and generate a signal. 1,2 As a result, OCTA can provide images of the layers of the retinal and choroidal vasculature without requiring dye injection, in contrast to fluorescein angiography (FA). 3
An important limitation of OCTA has been its vulnerability to commonly show image artifacts, which should be correctly recognized to avoid misinterpretations of the images. 2 Projection artifacts are one of the most common types of artifacts and an important source of confusion and lack of confidence when interpreting OCTA images. OCTA enables segmentation of various tissue layers, which ultimately generates en face images of the vasculature at any level of the retina and choroid. However, undesired projection effect from overlying blood vessels can result in the appearance of false blood flow signals in other layers, more commonly superficial vessels appearing to be in deeper layers, especially at the level of the retinal pigment epithelium (RPE) because of its highly reflective surface. 2 Because choroidal neovascularization (CNV) networks tend to be in close approximation to the RPE, these unwanted projection artifacts can be confused with CNV and prevent a correct identification and quantification of these lesions.
More recently, there have been efforts to improve the quality of OCTA images by minimizing the appearance of projections artifacts. An approach to minimize projection artifacts included a slab-subtraction algorithm, in which superficial signals were subtracted from deeper en face slabs. 4 However, this process can create shadowing artifacts in areas that previously had flow projection artifacts, and, in cases of CNV, can lead to underestimation of the real magnitude of the lesions and result in gaps of the neovascular network. 4,5
As an alternative, a projection-resolved algorithm has been created essentially based on the fact that projected flow signals are weaker than true flow signals. 4 The software then compares each voxel signal in relationship with the whole volume to decide which voxel represents projection artifact vs true flow. If a projection artifact is identified, its signal strength is automatically reduced to background level. Therefore, a projection-resolved algorithm can remove projection artifacts while preserving the continuity of deeper vessels and minimizing shadowing effects. 4,6
In light of the importance of minimizing projection artifacts for a correct clinical interpretation of OCTA images, the purposes of this study are to assess the frequency of projection artifacts in OCTA en face images of the retinal and choroidal vasculature networks and to compare these images before and after applying a 3D projection artifact removal (3D-PAR) algorithm technology.
Methods
This is a retrospective, observational, cross-sectional study that included consecutive patients with any underlying diagnosis who had OCTA obtained at a private-practice retina clinic in Canada from January 1, 2017, to March 31, 2017. Patients with various retinal diseases and also healthy eyes that had been scanned during this period were included. All participants underwent scan acquisition using spectral-domain OCTA obtained with Optovue RTVue XR Avanti (AngioVue, Optovue, Inc), including AngioVue DualTrac Motion Correction Technology to minimize OCTA artifacts related to fixation losses.
The scan area was 3 mm × 3 mm centered at the fovea. The 4 default autosegmented en face imaging slabs generated by the software were analyzed: superficial capillary plexus (SCP), deep capillary plexus (DCP), outer retina (OR), and choriocapillaris (CC). When needed, segmentations were manually manipulated to show the exact area of interest. Images with a scan quality less than 5/10 or with a signal strength index less than 55 were defined as nongradable and excluded from the analysis to ensure sufficient image quality.
Images were qualitatively analyzed by 2 independent graders before and after implementation of the phase 7 software with 3D-PAR technology. After undergoing 3D-PAR, projection artifacts in the images were classified as completely improved, partially improved, worsened, or unchanged. Grading disagreements were adjudicated by an additional grader. When CNV lesions were present, graders were asked to classify if 3D-PAR had improved, worsened, or had not changed CNV detection in these images. The vascular densities of the SCP and DCP were also obtained by the software using the built-in AngioAnalytics tool before and after images underwent 3D-PAR. However, a comparison between vessel densities before and after 3D-PAR could not be reliably conducted because the phase 7 software includes a segmentation border that significantly modifies vessel density compared with previous software versions. Therefore, these data were not included in our analysis.
Descriptive and statistical analyses were performed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corporation). Patients’ characteristics are presented in terms of mean, SD, or percentage as appropriate. Chi-squared test was used to compare proportions. Statistical significance was set at P < .05.
Results
A total of 194 eyes of 97 patients were included but 24 (12.4%) eyes of 21 patients were classified as nongradable and excluded from the analysis (total = 170 eyes). The mean age was 71.1 ± 15.7 years, and most patients were female (53.5%). Age-related macular degeneration was present in 70 eyes (41.2%), whereas 39 (22.9%) were healthy eyes without any underlying retinal disease. Table 1 shows the distribution of underlying retinal conditions of the study eyes.
Distribution of Underlying Diagnosis in the 170 Study Eyes.
Abbreviations: AMD, age-related macular degeneration; CNV, choroidal neovascularization; DME, diabetic macular edema.
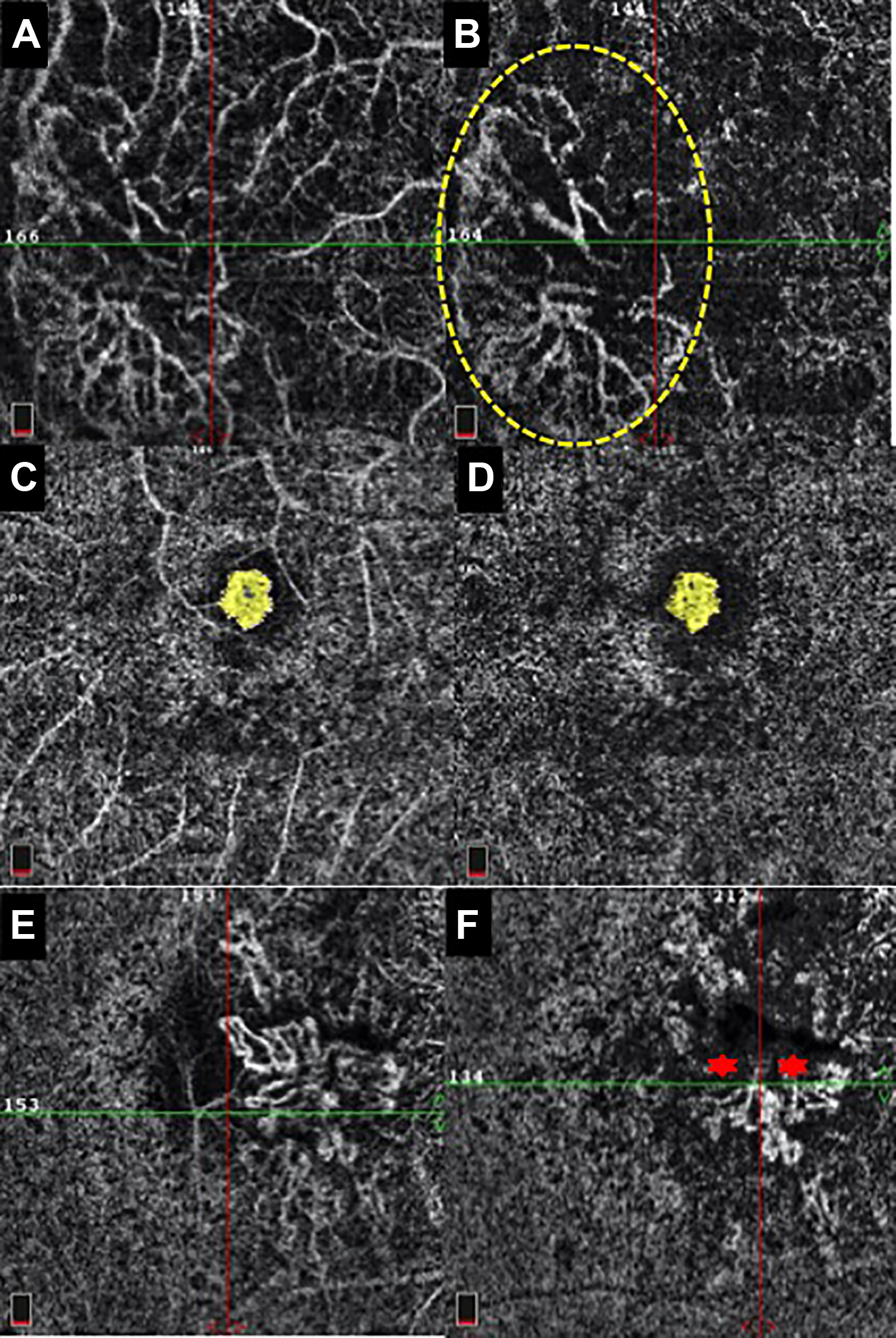
None of the eyes had projection artifact in the SCP before or after 3D-PAR. However, motion artifacts were present in the SCP of 3/39 healthy eyes and 25/131 eyes with retinal diseases (P = .138). In the DCP, 164 eyes (96.5%) had projection artifact before 3D-PAR. After 3D-PAR technology, 25 eyes (14.7%) had a complete improvement of projection artifact, 96 (56.5%) had a partial improvement, 24 (14.1%) were worse, and 25 (14.7%) presented no change (Figure 1).
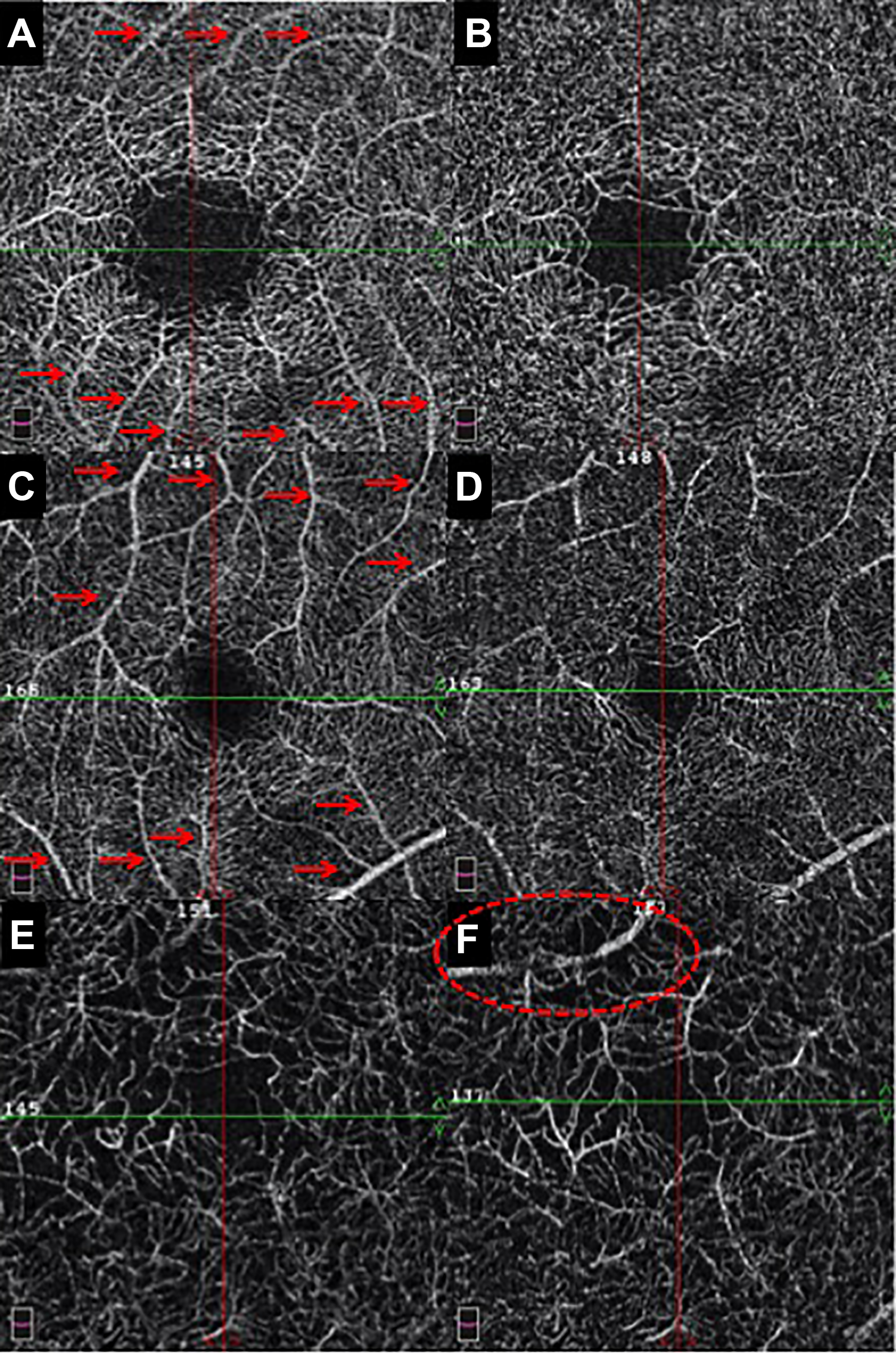
(A, C, and E) Optical coherence tomography angiography en face images of the deep capillary plexus before 3-dimensional projection artifact removal (3D-PAR) showing projection artifacts from more superficial retinal vessels (arrows). (B, D, and F) Images after 3D-PAR showing (B) a complete improvement of the projection artifacts, (D) partial improvement, and (F) subtle worsening as indicated by the dashed circle.
In the OR, 5 eyes (2.9%) had projection artifact. Among these images, there was a complete improvement after 3D-PAR in 2 eyes, partial improvement in 1, and no change in 2 (Figure 2). Among the 165 eyes (97.1%) that had no projection artifact in the OR before 3D-PAR, 26 images (15.8%) worsened after 3D-PAR and 139 (84.2%) remained unchanged (Figure 2).
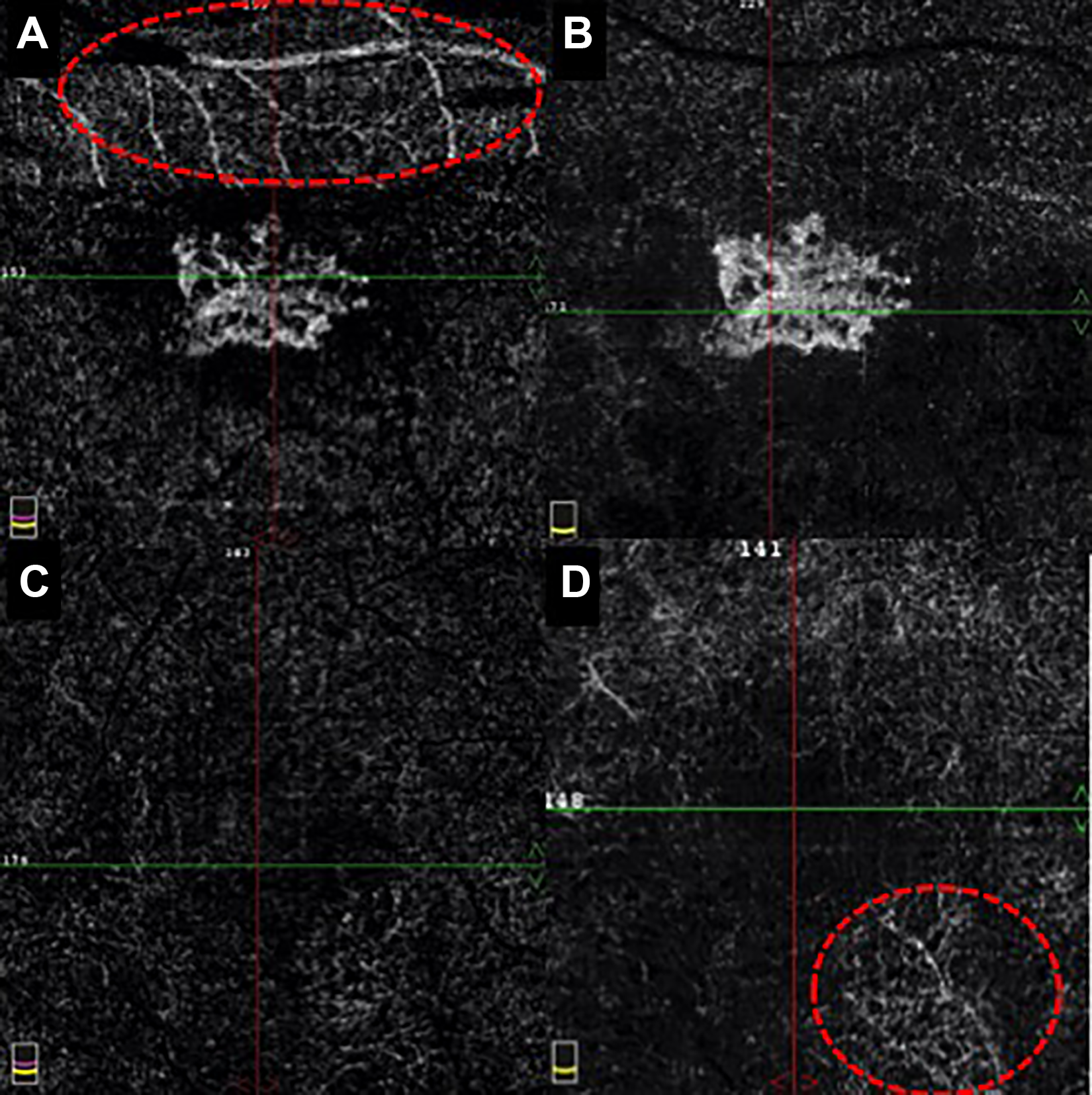
(A) Optical coherence tomography angiography en face image of the outer retina before 3-dimensional projection artifact removal (3D-PAR) reveals projection artifacts from more superficial retinal vessels (dashed circle) that (B) completely improve after 3D-PAR. (C) Outer retina slab before 3D-PAR without projection artifact, and (D) the same scan after 3D-PAR reveals a subtle projection artifact (dashed circle).
Projection artifact in the CC was initially present in 166 images (97.6%). After 3D-PAR, there was a complete improvement in 121 eyes (72.9%), partial improvement in 44 eyes (26.5%), and no change in 1 eye (0.6%) (Figure 3). None of the images of the CC layer presented with a worsening of projection artifact after 3D-PAR. In addition, all images of the CC classified as not having projection artifact (2.4%) before 3D-PAR remained unchanged. No significant differences were encountered between the presence of projection artifacts before and after 3D-PAR in OCTA images of eyes with retinal diseases vs healthy eyes.
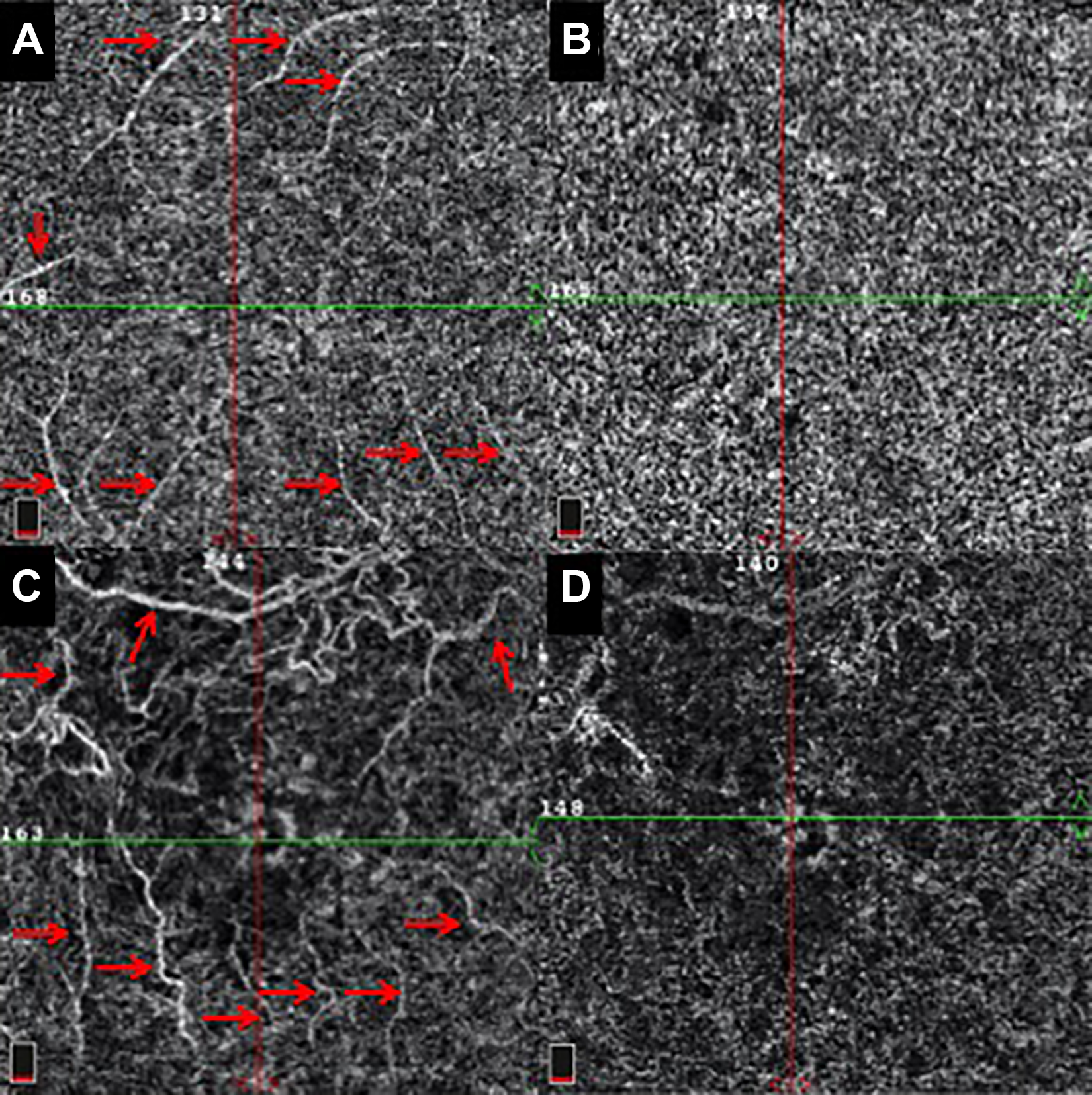
Optical coherence tomography angiography en face images of the choriocapillaris before 3-dimensional projection artifact removal (3D-PAR) (A and C) reveal projection artifacts (arrows) that (B) completely and (D) partially improve after 3D-PAR.
CNV was detected in 29 eyes (17.1%) and 3D-PAR improved CNV detection in 12 cases (41.4%). Detection of CNV lesions was classified as more difficult in 6 eyes (20.7%) and as unchanged in 11 (37.9%) (Figure 4).
Optical coherence tomography angiography en face images of the choriocapillaris in patients with choroidal neovascularization (CNV). (A) Large CNV network initially surrounded by projection artifact. (B) Same CNV network becomes more clearly visualized (dashed circle) after 3-dimensional projection artifact removal (3D-PAR) eliminates the surrounding projection artifacts. (C and D) An example of complete improvement of projection artifact after 3D-PAR that did not interfere with the detection of the CNV (outlined). (E) CNV network evident in a scan that contains some projection artifacts and then (F) the same scan after 3D-PAR showing less projection artifacts but significant gaps and shadows (asterisks) within the CNV lesion.
Conclusions
OCTA technology has revolutionized the assessment of the retinal and choroidal vascular networks by providing a 3D view of the multilayered vasculature. However, projection artifacts can frequently be present in OCTA images, confounding the interpretation of these 3D vascular networks, which can lead to misdiagnosis and unnecessary treatments. In an attempt to resolve this important limitation, a 3D-PAR algorithm has become commercially available and we compared images before and after undergoing 3D-PAR processing.
The addition of 3D-PAR in OCTA minimized the appearance of projection artifacts in en face images of the DCP. In this study, almost all (96.5%) images of the DCP originally presented projection artifacts. After 3D-PAR, 71.2% of these images showed a partial or complete improvement of projection artifacts. Removing projection artifacts immediately beneath large-caliber vessels can be challenging because of greater and more variable signal disturbances. 6 Previous studies have also shown examples of how PAR algorithms have improved visualization of the DCP by minimizing projection artifacts. 6 -8 A better visualization of the DCP is important to reveal microvascular changes and areas of nonperfusion in common diseases, such as diabetic retinopathy and retinal vein occlusion, and in the early detection of retinal angiomatous proliferation because these vessels originate in the DCP. 6,9 For instance, one of the great advantages of OCTA when compared with FA is its ability to allow visualization of 3 vascular plexuses and enable a clear separation between the SCP and DCP. Diabetic retinopathy, for example, tends to affect preferentially smaller vessels, so removing projection artifacts from the DCP becomes particularly important for the quantitative analysis of vessel density and areas of nonperfusion, since projections from the SCP can result in falsely higher vessel density in the DCP. 7
A significant advantage of OCTA is its ability to detect CNV without requiring dye injection as used in FA, and can be a tool to noninvasively observe disease progression and response of CNV lesions to anti–vascular endothelial growth factor therapy. 10 -12 However, a major source of criticism involving OCTA technology is that projection artifacts can interfere with a clear visualization of CNV and with the quantitative analysis of the neovascular lesions.
Most (97.6%) en face images of the CC originally presented projection artifacts, and the 3D-PAR algorithm was effective in reducing projection artifacts in 99.4% of the cases, with the majority of the images showing a complete improvement. In addition, the images that originally did not present projection artifact remained unchanged after 3D-PAR. This finding will likely enhance physicians’ confidence when observing images of the CC, as this main source of confusion is mostly eliminated. Projection-free images of the CC layer can also possibly allow for a more accurate delimitation of the CNV and therefore result in more reliable measurements of the lesions in an attempt to monitor progression and response, as reported previously. 13
Even though 3D-PAR technology is known to maintain more vascular continuity of the deeper layers than earlier methods of projection artifact removal such as slab subtraction, we also assessed whether resultant shadowing effects were still present and could interfere in the detection of CNV lesions. 4,6 In our study, of eyes that had CNV, 3D-PAR improved or did not interfere with the detection of CNV lesions in 41.4% and 37.9% of the cases, respectively. The minority of the lesions presented shadowing effects after 3D-PAR and resulted in gaps in the CNV that interfered with CNV detection. Therefore, the addition of 3D-PAR may enhance detection of CNV but still remains imperfect as it may introduce gaps in deeper vascular networks.
As expected, none of the eyes presented projection artifacts in the SCP, since this artifact is typically produced by superficial vessels casting false flow shadows on deeper layers. 2 However, motion artifacts in the SCP were still present in 16.5% of the eyes despite the use of DualTrac Motion Correction technology. These were much more predominant in eyes with retinal diseases compared with healthy eyes, even though this difference was not statistically significant, as also described by Enders et al. 14 This fact could be attributed to issues involving fixation losses that can be more common in patients with reduced visual acuity due to their underlying retinal conditions.
The OR slab, which is supposed to show an avascular state, originally had the majority of the eyes without any projection artifact. Even though most cases remained unchanged after 3D-PAR, artificial flow signals were created in 15.8% of the eyes. It must be highlighted, though, that these tended to be subtle changes as illustrated in Figure 2. Because only 5 eyes (2.9%) originally presented with projection artifact in the OR, appropriate conclusions regarding projection artifact removal from these images cannot be drawn.
This study has some limitations that should be addressed. Because of its retrospective design, only 3 mm × 3 mm scans were included in this study, as these had been more commonly obtained than larger scans. Therefore, our results cannot be extrapolated to other scans such as 6 mm × 6 mm. In addition, it would have been useful to obtain quantitative analysis, including vessel densities in the SCP and DCP, areas of nonperfusion, and flow area of CNV networks. However, a comparison of these measurements before and after 3D-PAR could not be reliably performed as previously mentioned.
In conclusion, OCTA with 3D-PAR technology minimizes the appearance of projection artifacts in the DCP and CC slabs. Therefore, this can be a helpful tool used by retina specialists to better and more confidently interpret OCTA images and to improve the efficacy of clinical assessments and lesion detection.
Footnotes
Ethical Approval
This retrospective chart review of patients was conducted under appropriate institutional review board approval and was conducted according to the Declaration of Helsinki.
Statement of Informed Consent
No informed consent was necessary because of the retrospective nature of this review, and all data collection and analyses were performed without any patient identifiers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.