
Abstract
Purpose:
This case report describes a unique case of a young patient with retinopathy of prematurity (ROP), a unilateral Coats-like response, and X-linked retinoschisis (XLRS).
Methods:
A 9-year-old boy with a history of regressed ROP presented with a unilateral Coats-like response, subretinal exudation, and XLRS. Examination and imaging findings demonstrated a highly unique combination of bilateral retinoschisis and a dramatic unilateral Coats-like response with a large schisis cavity.
Results:
Treatment with laser photocoagulation and anti-VEGF therapy led to resolution of the subretinal exudative changes.
Conclusions:
This is the first published description to our knowledge of a patient with a Coats-like response, XLRS, and a history of regressed ROP with resolution after treatment.
Introduction
Retinopathy of prematurity (ROP) is a vasoproliferative disease affecting premature and low-birthweight infants. 1 Eyes with ROP have abnormal vascular growth, peripheral ischemia, and fibrovascular proliferation. ROP can regress or may lead to tractional retinal detachment (RD). 2 Treatment involves laser photocoagulation or cryotherapy, antivascular endothelial growth factor (anti-VEGF) therapy, and in severe stages, vitrectomy. 1,2
Coats disease is a predominantly unilateral retinal vasculopathy characterized by telangiectasia, ischemia, aneurysmal change, and exudation usually in young males between ages 8 and 16 years. 3 -5 Treatment includes photocoagulation or cryotherapy with adjunctive anti-VEGF or triamcinolone. 6 -8
X-linked retinoschisis (XLRS) is an inherited retinal dystrophy classically described by foveal schisis of the inner retinal layers, with possible involvement of the peripheral retina in some cases. 7,9 Certain diseases can present with Coats-like reactions, including retinitis pigmentosa, retinoblastoma, retinal vasoproliferative tumors, and XLRS. 7,9 -12 We describe a unique case of a child screened for ROP who later developed decreased vision and bilateral macular and peripheral schisis consistent with XLRS and a Coats-like response in the setting of regressed ROP.
Methods
A 9-year-old African American boy, born at 24 weeks’ gestational age and 625 grams birthweight, presented to the pediatric retina clinic with blurred vision. Both parents and the patient’s 5 siblings were all noted to have normal visual development without any family history of ocular diseases. As a neonate, he had spent 4 months in intensive care, where he received supplemental oxygenation for bronchopulmonary dysplasia and intraventricular hemorrhage. He was diagnosed with zone II, stage 2 ROP without plus disease in both eyes that spontaneously regressed to zone III without treatment.
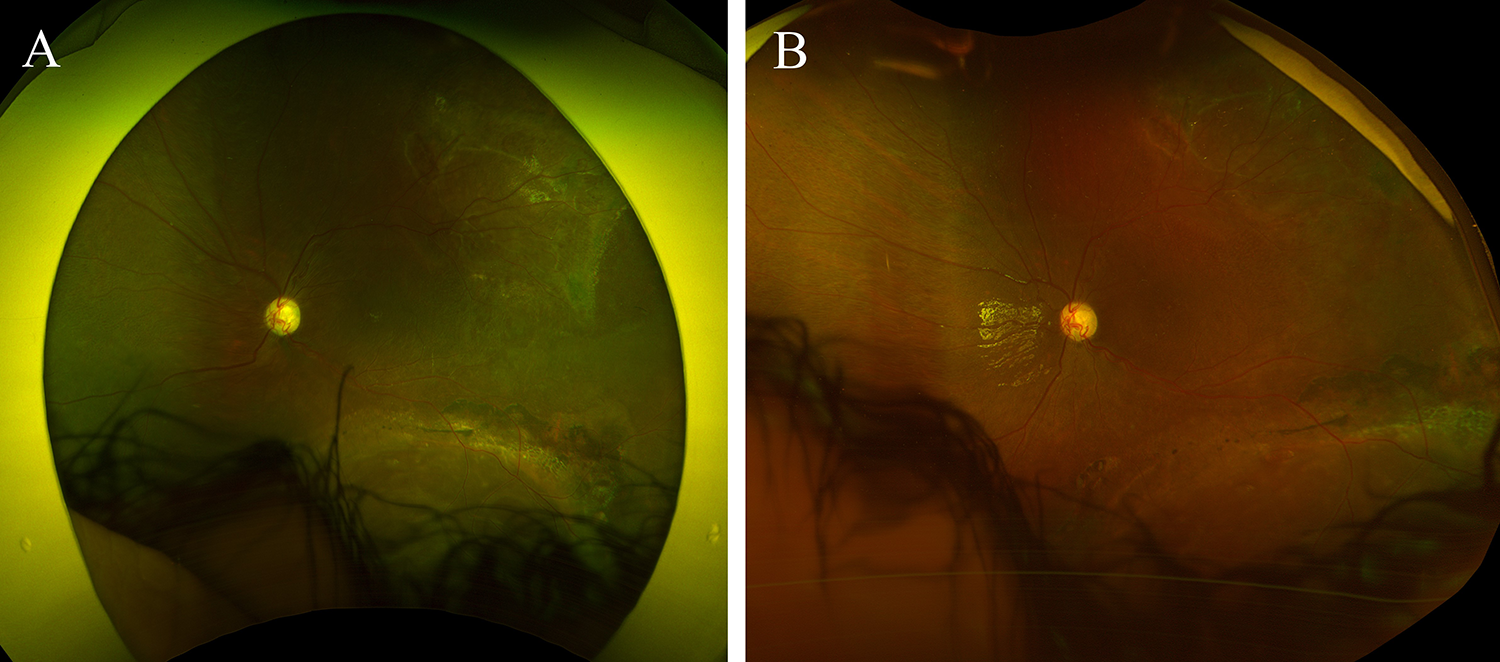
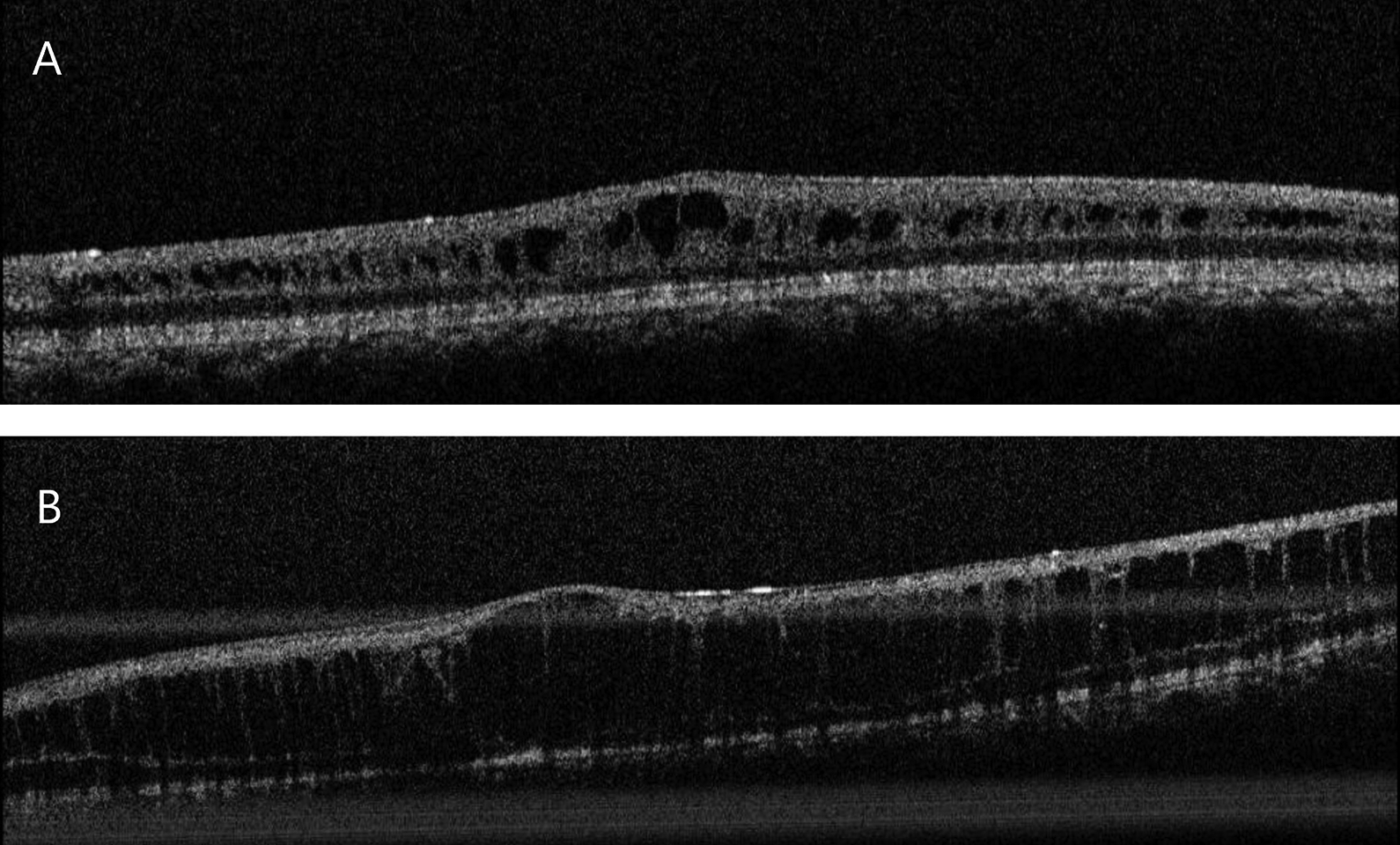
On presentation, best-corrected visual acuity was 20/70 and 20/200 in the right and left eyes, respectively. Clinical examination disclosed a normal anterior segment in both eyes, and funduscopic examination showed macular schisis in both eyes with temporal and inferior areas of peripheral retinoschisis in the right eye and diffuse exudation most prominent near a large inferior schisis cavity in the left eye (Figure 1). Optical coherence tomography confirmed the macular schisis and a large schisis cavity in the right eye and subretinal fluid accumulation inferiorly in the left eye (Figure 2). Fluorescein angiography showed telangiectasias, aneurysms, and capillary dropout in the left eye, concentrated near the area of exudative RD (Figure 3). Ultrasound demonstrated a schisis cavity in the right eye and RD in the left eye (Figure 4).
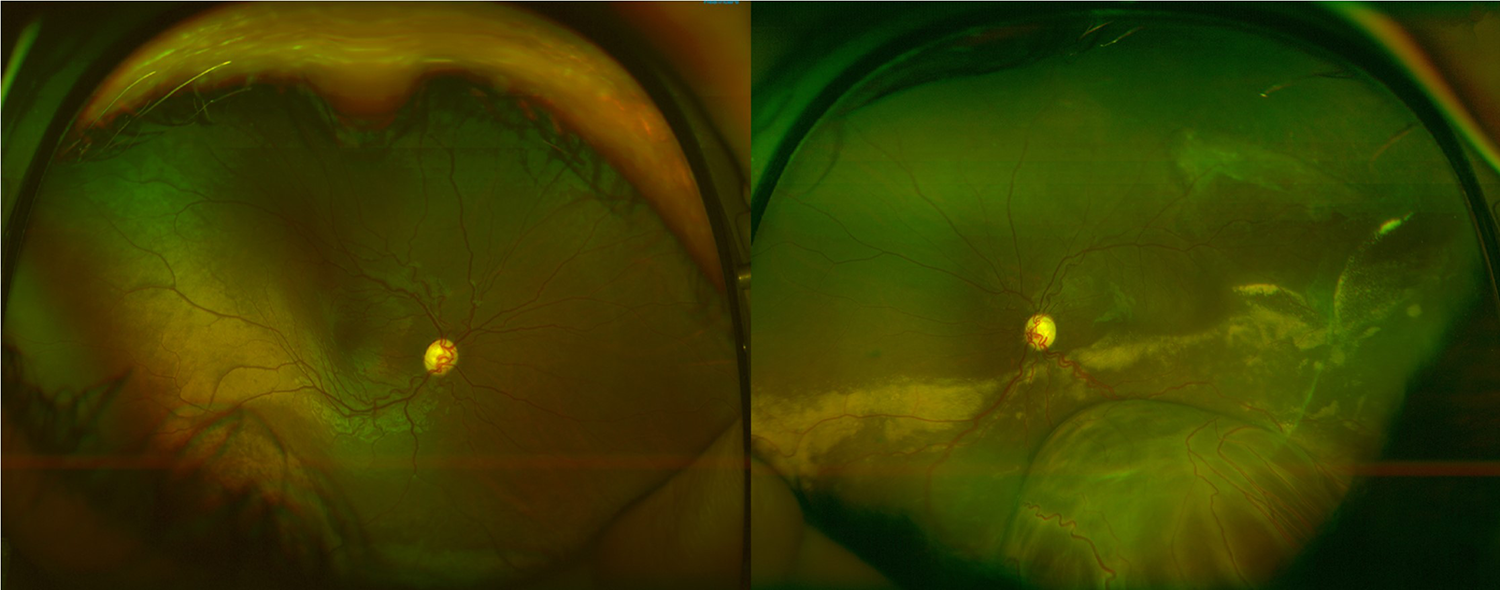
Color fundus photograph of the right eye shows temporal and inferior areas of whitening elevation with cystic appearance consistent with retinoschisis and of the left eye discloses diffuse inferior exudative changes associated with associated exudative retinal detachment.
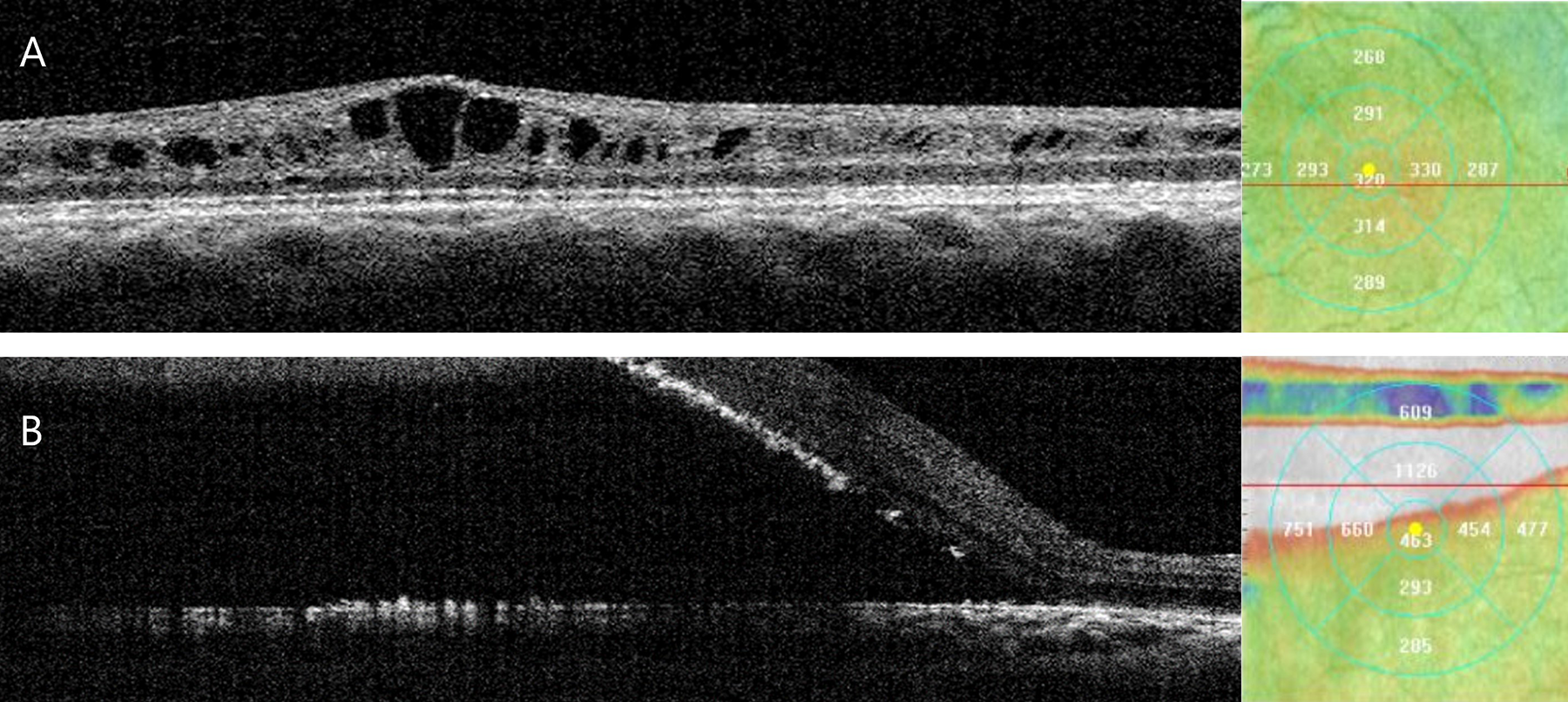
Optical coherence tomography of (A) the right eye reveals macular cystic intraretinal fluid. (B) Optical coherence tomography of the left eye with associated thickness map demonstrates significant macular subretinal fluid with hyperreflective exudation consistent with exudative retinal detachment.
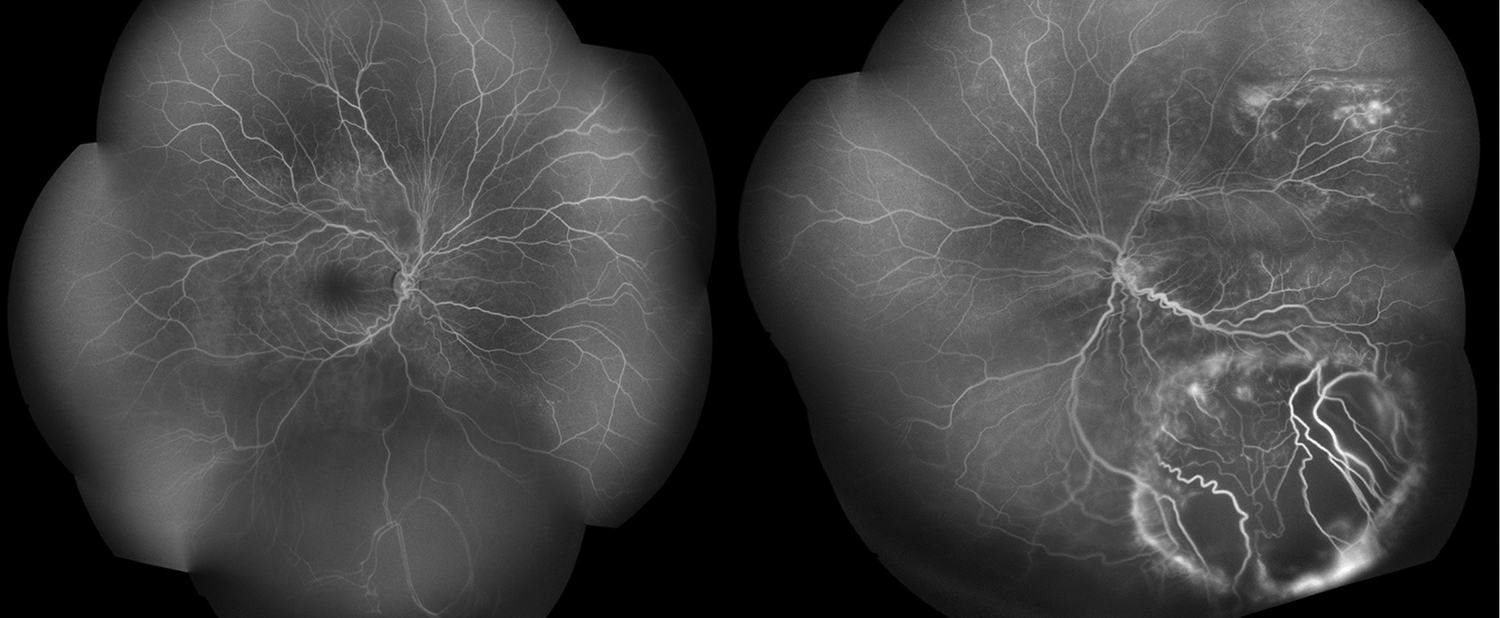
Late-phase fluorescein angiography of the right eye reveals inferior capillary nonperfusion and of the left eye shows temporal and inferior telangiectasias, aneurysms, and areas of nonperfusion with peripheral late-phase leakage.
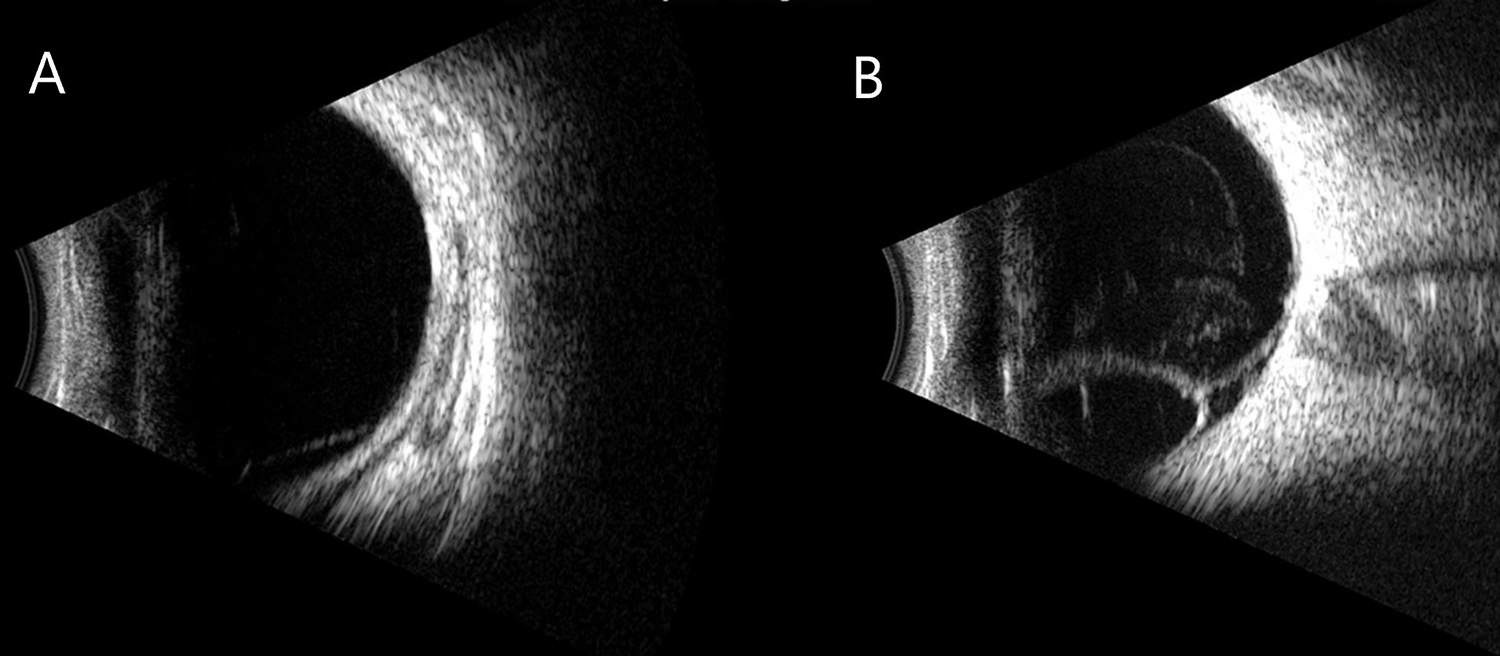
B-scan of (A) the right eye shows retinoschisis and of (B) the left eye demonstrates a retinal detachment with subretinal fluid and schisis without a retinal break.
Results
During examination under anesthesia, the left eye was injected with intravitreal bevacizumab (IVB) and diode laser photocoagulation was applied around the inferior detachment and areas of retinal vascular leakage. No treatment was performed in the right eye. A second session of photocoagulation was repeated during examination under anesthesia 6 weeks later with a second injection of IVB in the left eye. Two months following treatment, best-corrected visual acuity was 20/60 in both eyes. Improvement was noted in the level of exudation as well as a stable appearance of the inferior retinal schisis cavity at 2 and 6 months postoperatively (Figure 5, A and B, respectively). Optical coherence tomography of the right eye demonstrated improvement of schisis and of the left eye showed significant resolution of the serous RD (Figure 6).
Color fundus photographs of the left eye demonstrate improvement of exudation, with a persistent dome-shaped schisis cavity inferiorly located after laser photocoagulation and intravitreal bevacizumab at (A) 2 months postoperatively and (B) 6 months postoperatively.
Optical coherence tomography of (A) the right eye reveals persistent intraretinal cystic changes with mild improvement of schisis and of (B) the left eye shows significant improvement of subretinal fluid with persistent schisis and intraretinal cystic changes.
Conclusions
The present report describes the first case to our knowledge of XLRS with a unilateral Coats-like response in a patient with a history of ROP that resolved after IVB and laser. The coexistence of Coats-like retinopathy with presumed XLRS is highly unusual and has not been reported in concurrence with ROP. 7,9,13 A few studies in the literature have reported exudative peripheral vascular changes in XLRS. 10,14 Such cases have reported Coats-like reactions associated with central and peripheral retinoschisis localized to areas of telangiectatic and robust exudative changes in the ipsilateral eye. 7,9 These findings were consistent with those in our patient, where the foveal and peripheral retinoschisis coincided with the area of exudative RD. Unfortunately, our patient declined genetic testing.
The Coats-like response in our patient coincided with a history of ROP. The de novo onset of Coats exudation in ROP has been described only once in the literature but never with concomitant retinoschisis. 4,7,13,15 Conversely, the occurrence of tractional retinoschisis without Coats exudation in late, untreated ROP has been reported by Hamad et al at an incidence of almost 12% of eyes. 16 In 2015, Gursoy and colleagues reported a case of advanced bilateral ROP with sequential bilateral Coats-like retinopathy without retinoschisis. 4 A combination of anti-VEGF, photocoagulation, and cryotherapy resulted in regression. Severe exudative Coats-like responses have also been noted after laser photocoagulation. 17 In our patient, the ROP regressed without treatment, but a severe unilateral Coats-like response occurred years later. Furthermore, bilateral macular and peripheral retinoschisis were present.
The pathophysiology of this specific Coats-like reaction in the setting of both XLRS and ROP cannot be definitively known. The authors hypothesize that given the location of the exudation, the Coats-like exudation was largely attributable to the anatomical vasculature changes associated with the retinoschisis. Additionally, it is possible that the abnormal vessels in ROP after regression are prone to leaks under anatomical stress and may have worsened the initial exudative reaction.
Regarding treatment of exudative RD associated with Coats-like reactions, multiple groups have reported reasonable visual outcomes in eyes treated with laser photocoagulation and IVB, with or without sub-Tenon triamcinolone. 18,19 However, it is important to note that these patients did not have concurrent bilateral XLRS or retinal macrocysts. One group demonstrated that only 33% of patients with retinal macrocysts in Coats disease experienced anatomical resolution after repair, subretinal drainage with cryotherapy, or photocoagulation, implying that macrocysts may be a risk factor for poorer prognosis. 20 The present case resulted in 20/60 vision in both eyes with anatomic resolution of exudation, RD, and macrocyst in the left eye after laser photocoagulation and IVB.
In conclusion, we present the first reported case of a Coats-like exudative RD in XLRS in the setting of regressed ROP. Although a handful of similar cases of XLRS with exudative retinopathy have been reported in the literature before, each unique case lends insight into the mechanisms by which Coats-like retinopathy, retinoschisis, and ROP are related and the complications that may arise. In our patient, there was a favorable outcome after a combination of IVB and laser. Although we suggest that anti-VEGF and laser photocoagulation in these cases may be effective treatments, further studies should investigate the best approach for these complex pediatric vitreoretinal disorders.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)–compliant manner.
Statement of Informed Consent
Informed consent was obtained prior to performing the procedure, including permission for publication of all photographs and images included herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by NIH center grant P30-EY014801, and an unrestricted grant to Bascom Palmer Eye Institute from Research to Prevent Blindness, Inc.