
Abstract
Purpose:
We describe the development and management of choroidal neovascularization (CNV) in a patient with acute syphilitic posterior placoid chorioretinitis (ASPPC).
Methods:
A retrospective case review is presented.
Results:
A 66-year-old man presented with unilateral blurry vision. He had a history of systemic syphilis infection twice, the last diagnosed 15 years before presentation and treated with intravenous ceftriaxone, resulting in seroreversion of an initially positive rapid plasma reagin (RPR). Examination revealed ASPPC with subfoveal CNV. Repeat testing revealed an RPR titer of 1:16 384. He was treated with 6 monthly intravitreal injections of bevacizumab and systemic antibiotics, resulting in resolution of his ASPPC and regression of his CNV.
Conclusions:
CNV is a rare complication of ASPPC. Multimodal imaging can be useful to suggest the diagnosis, and prompt treatment with systemic antibiotics and intravitreal anti-vascular endothelial growth factor agents can lead to resolution of ASPPC and regression of CNV, respectively.
Introduction
Syphilis is a chronic sexually transmitted disease caused by the spirochete Treponema pallidum (T pallidum). Syphilis infection is often termed the great imitator, because virtually any organ system can be affected, with protean clinical manifestations. As the incidence of syphilis is increasing in the United States, along with the rate of ocular syphilis, ophthalmologists may encounter various ocular manifestations of undiagnosed or untreated secondary or tertiary T pallidum infection.1,2 Early diagnosis is critical to promptly initiate appropriate therapy and prevent irreversible vision loss.
Ocular syphilis can manifest with a multitude of posterior segment findings, including vitritis, superficial retinal precipitates, serous retinal detachment, retinitis, vasculitis, retinal vascular occlusions, chorioretinitis including acute syphilitic posterior placoid chorioretinitis (ASPPC), and optic nerve abnormalities.3,4 Rarely, posterior segment syphilis can be complicated by the formation of choroidal neovascularization (CNV), and there are few reports documenting the clinical presentation and management of this uncommon complication.5–7 We present a case of ASPPC presenting with subfoveal CNV that improved with combined systemic antibiotics and intravitreal anti-vascular endothelial growth factor (anti-VEGF) therapy.
Methods
Case Report
A 66-year-old White man was referred to our institution for evaluation of 3 months of blurry vision and floaters in the left eye that had worsened over the past week. He was asymptomatic in the right eye. He had a past medical history of systemic hypertension, hyperlipidemia, atrial fibrillation, and HIV infection. He reported compliance with antiretroviral therapy resulting in an undetectable HIV viral load 2 months prior and a CD4 count of 1055 cells/mm3. He also reported 2 prior independent diagnoses of active syphilis, the last being 15 years before presentation, around the time of his HIV diagnosis. Owing to a previously reported penicillin allergy, the patient was treated with intravenous (IV) ceftriaxone at the time. He was followed by an infectious disease physician with serial rapid plasma reagin (RPR) titers, and his last RPR 2 years before presentation was nonreactive. His review of systems was negative for any fevers, chills, cough, hearing changes, balance issues, or rashes.
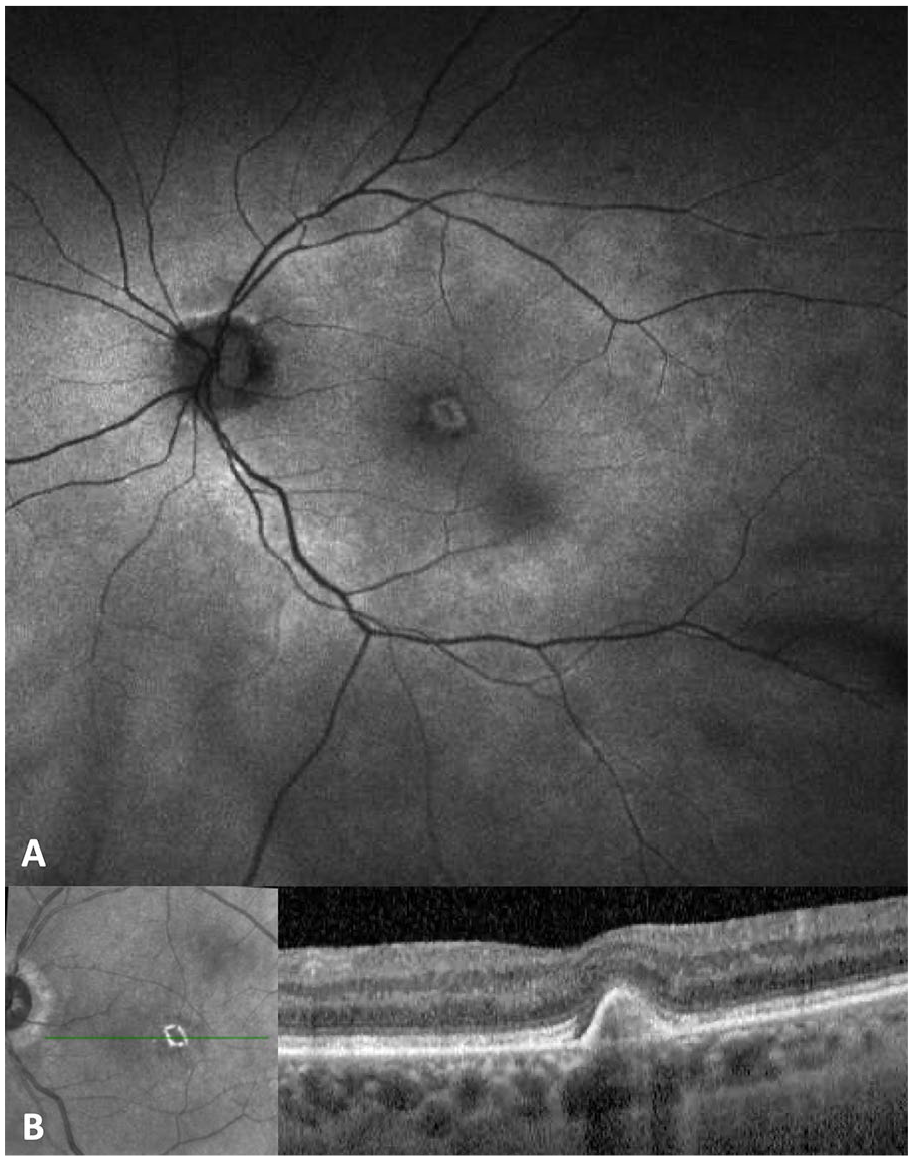
On our initial examination, his visual acuity (VA) was 20/20 OD and counting fingers at 4 feet (1.2 m) OS. Pupillary examination and intraocular pressures were normal bilaterally. Examination of the right eye was unremarkable, and there was no evidence of inflammation. Examination of the left eye showed trace anterior vitreous cell, white cellular deposits on the elevated posterior hyaloid, optic disc edema, peripapillary subretinal fluid, a subtle round placoid lesion with stippled edges centered on the posterior pole, and a subfoveal lesion (Figure 1). Autofluorescence of the left eye showed hyperautofluorescence corresponding to the placoid lesion (Figure 2A). Optical coherence tomography (OCT) of the left eye showed peripapillary subretinal fluid and subfoveal pigment epithelial detachment (PED) with hyperreflective material, trace overlying intraretinal fluid, and marked irregularity of the ellipsoid zone (Figure 2B). Fluorescein angiography of the left eye demonstrated leakage at the optic nerve and fovea as well as staining of scattered peripheral punctate spots (Figure 3). In the area of the subfoveal lesion, there was corresponding blockage on indocyanine green angiography of the left eye (Figure 4). Multimodal imaging was unremarkable in the right eye.

Optos photograph of the left eye demonstrating mild vitreous haze, multiple deposits on the posterior hyaloid, optic disc edema, and a subfoveal lesion. (A) Widefield Optos photograph. (B) Higher magnification photograph.
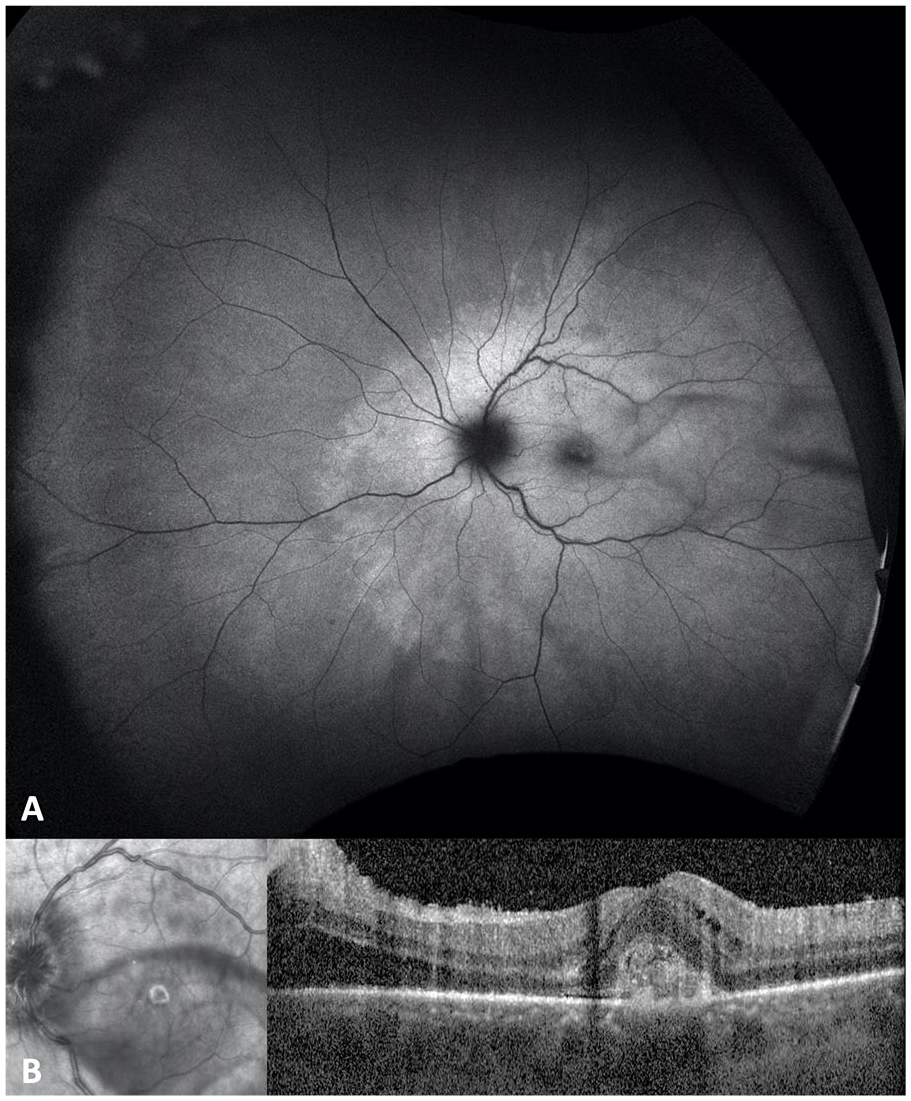
(A) Fundus autofluorescence demonstrating hyperautofluorescence in the macula and peripapillary region. (B) Optical coherence tomography demonstrating subfoveal hyperreflective material with overlying intraretinal fluid and peripapillary subretinal fluid and disruption of the inner segment/outer segment junction.
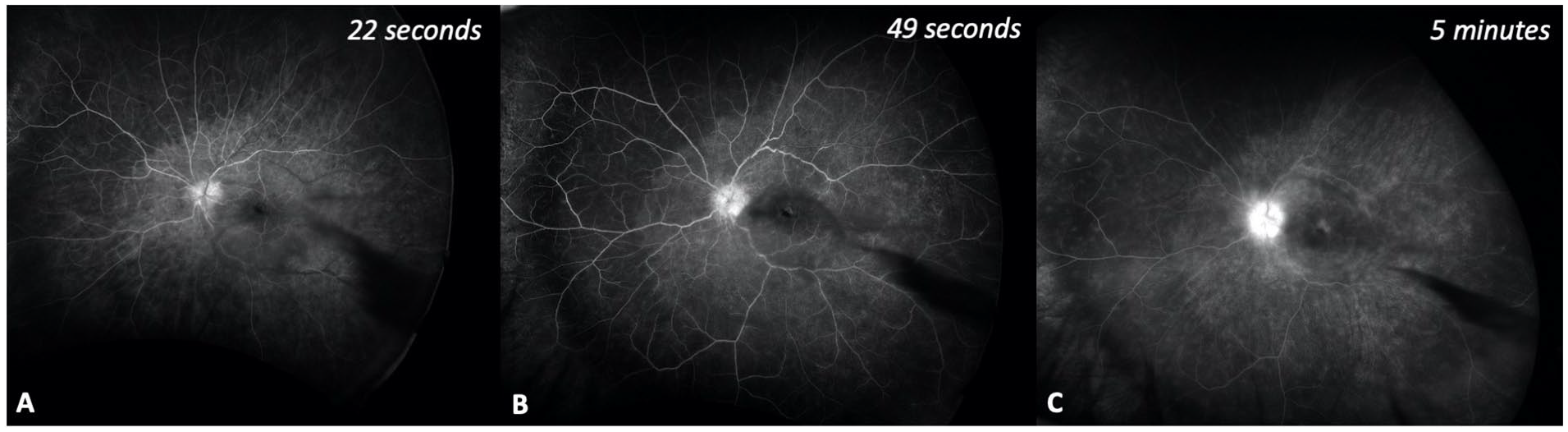
Fluorescein angiography with mild hyperfluorescence corresponding to the posterior pole placoid lesion and with leakage from the optic nerve and subfoveal lesion, suggestive of subfoveal choroidal neovascularization: (A) 22 seconds; (B) 49 seconds; and (C) 5 minutes.
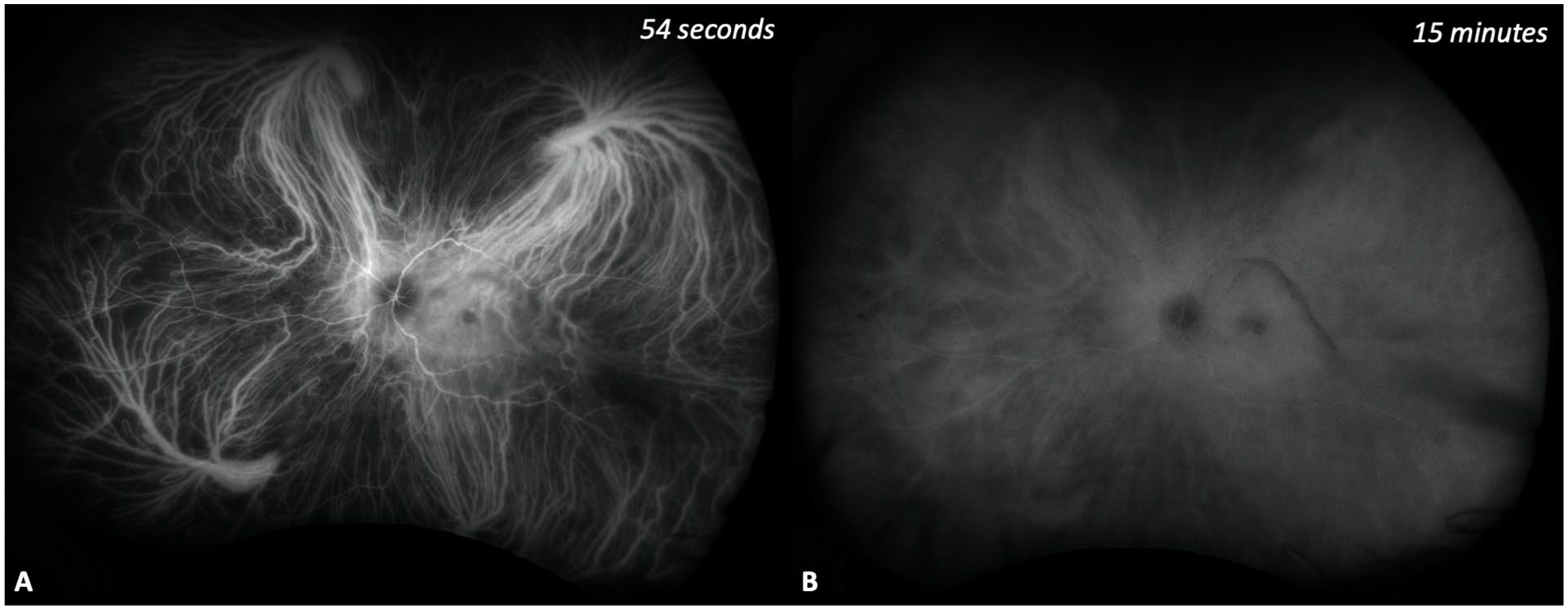
Indocyanine green angiography demonstrating blockage in the area of the subfoveal lesion: (A) 54 seconds; and (B) 15 minutes.
Results
The patient was diagnosed clinically with ASPPC complicated by the formation of CNV. An RPR was positive at 1:16 384. Other tests including QuantiFERON-TB Gold, anti-Toxoplasma gondii serology, and angiotensin-converting enzyme and lysozyme levels were unremarkable. The patient refused lumbar puncture (as he did at the time of his prior diagnosis). He underwent a 14-day course of IV ceftriaxone while undergoing formal allergy testing for penicillin. After his penicillin allergy blood and skin tests were both negative, he received a 14-day course of IV penicillin.
At his initial presentation and monthly thereafter, he received an intravitreal bevacizumab injection (1.25 mg/0.05 mL) to treat the CNV in the left eye. After 2 injections and completion of 14 days of IV ceftriaxone, but before initiating IV penicillin, the patient’s VA had improved to 20/100 with resolution of peripapillary subretinal fluid and reduction in hyperautofluorescence in the macula and peripapillary regions. His OCT angiography (OCTA) after 2 anti-VEGF injections showed a CNV membrane within the outer retinal layer (Figure 5). After 6 intravitreal bevacizumab injections and completion of the IV penicillin course, his VA improved to 20/40 with pinhole to 20/30 with resolution of subretinal and intraretinal fluid and persistence of a medium reflectivity PED (Figure 6). His repeat RPR titer improved to 1:1024.
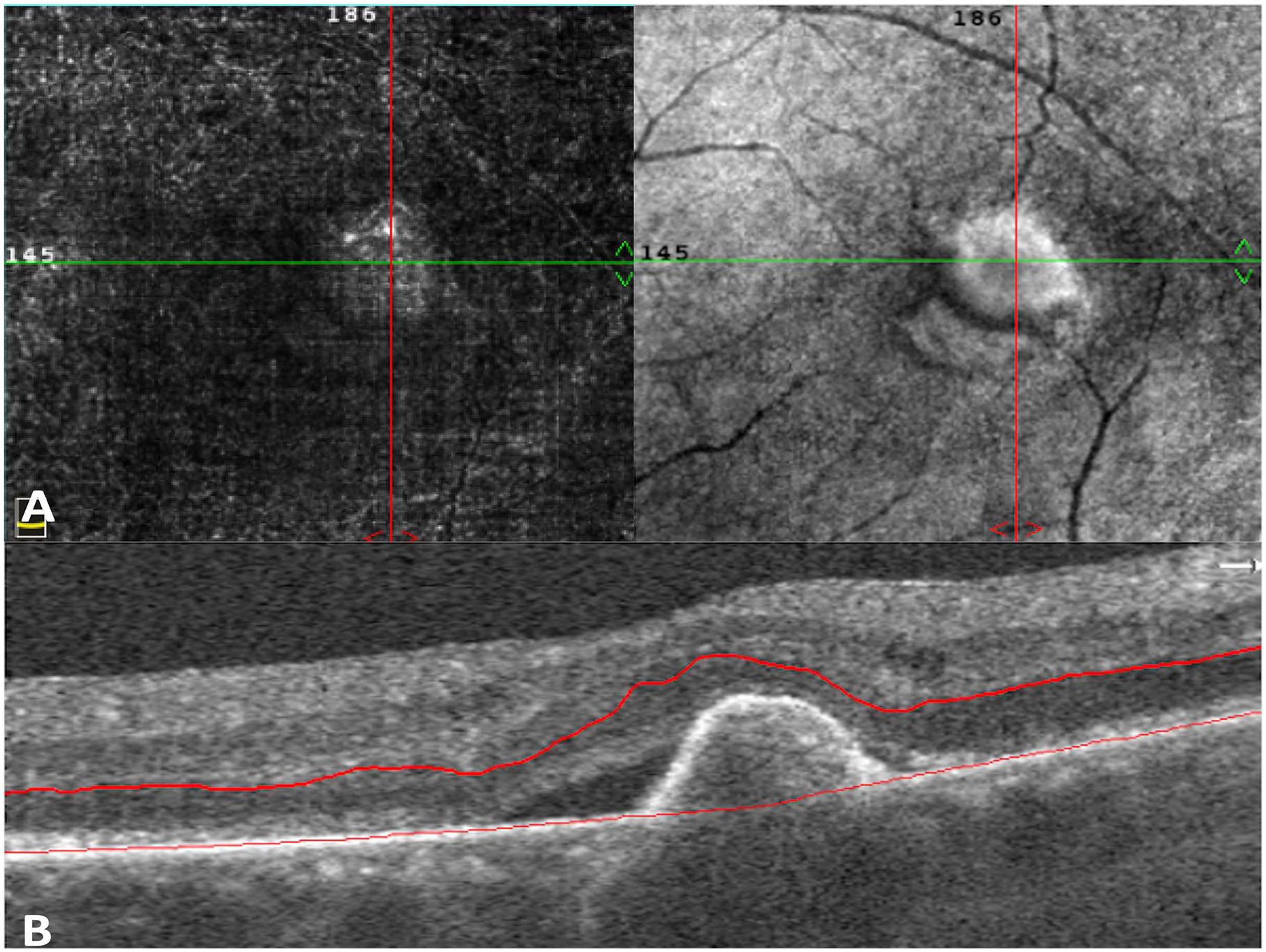
Optical coherence tomography angiography (OCTA) of the left eye demonstrating a choroidal neovascular membrane in the outer retinal layer after 2 anti-vascular endothelial growth factor injections. (A) OCTA and en face OCT images of the outer retinal layer. (B) Corresponding OCT B scan.
Status post 6 anti-vascular endothelial growth factor injections and intravenous antimicrobials. (A) Fundus autofluorescence with reduction of hyperautofluorescence in the macula and peripapillary region. (B) Optical coherence tomography showing resolution of peripapillary subretinal fluid and improved subfoveal hyperreflective material.
Conclusions
Patients with both infectious and noninfectious posterior uveitis can develop inflammatory CNV, which is particularly common in the setting of multifocal choroiditis/punctate inner choroiditis and presumed ocular histoplasmosis syndrome but uncommon in other forms of uveitis. These acute inflammatory lesions can occur with localized PEDs and are often hyperreflective and subretinal in location on OCT imaging. 8 The lesion described in our patient is consistent with subfoveal inflammatory CNV. Although rare, this presentation is important to recognize as part of the various manifestations of syphilis involving the posterior segment.
There are few reports of CNV secondary to syphilis. In 1989, Halperin et al 5 reported 5 patients with unilateral CNV secondary to T pallidum infection. Patients with active infections were managed systemically with antibiotics. Three of the 5 patients had subfoveal CNV that was managed conservatively, whereas one had extrafoveal CNV that was treated with argon laser photocoagulation; 4 of the 5 patients had minimal acuity recovery, and the remaining patient did not have VA data after treatment. Balaskas and colleagues 6 reported a single case of peripapillary CNV that occurred during active syphilis infection; this patient was treated with IV penicillin and oral corticosteroids as prophylaxis for Jarisch-Herxheimer reaction with improvement in his VA from 6/18 to 6/9. Giuffrè et al 7 more recently described a case of peripapillary CNV that developed 2 years after resolution of syphilitic chorioretinitis that was treated with 3 anti-VEGF injections and oral corticosteroids, resulting in some VA improvement from 20/63 to 20/50. Given negative Venereal Disease Research Laboratory test titers both in serum and cerebrospinal fluid, syphilis reinfection was ruled out, and thus IV penicillin was not given for this patient.
The mechanism of CNV formation in ocular syphilis is not completely understood. Our patient developed ASPPC and subfoveal CNV in the setting of an extremely elevated RPR titer and a history of 2 earlier episodes of syphilis infection. A likely mechanism of CNV formation in our patient is extensive inflammatory damage to the retinal pigment epithelium–Bruch membrane complex, 7 either from repeated infection or chronic infection. He may have become reinfected with syphilis, or perhaps he was inadequately treated for his prior syphilis infection 15 years ago when he was treated only with IV ceftriaxone given a reported penicillin allergy.
Of note, our patient was HIV positive, although well managed with antiretroviral therapy with undetectable viral load. There are high rates of coinfection with HIV and syphilis, likely due to shared risk factors in tramission.9,10 Lee et al 10 examined RPR titers in patients with ocular syphilis with HIV compared with HIV-negative individuals; the authors found significantly higher serum RPR titers in ocular syphilis patients with HIV-positive status relative to HIV-negative status. Interestingly, our patient had an extremely high titer of RPR at 1:16 384. Patients with positive syphilis serologic tests and ocular findings are recommended to undergo a lumbar puncture to screen for neurosyphilis. 9 Although our patient refused lumbar puncture, his overall management plan was unchanged as he was treated with a 2-week systemic course of IV ceftriaxone, then IV penicillin. Ocular syphilis, as well as otosyphilis and neurosyphilis, requires a 10- to 14-day course of a systemic antibiotic for treatment. 9
Our patient responded well with resolution of his intraocular inflammation, disc edema, and subretinal fluid, with corresponding substantial improvement in his VA after treatment with anti-VEGF injections and systemic antimicrobials. This is the first report to use intravitreal anti-VEGF agents for the management of syphilitic subfoveal CNV. Anti-VEGF agents, in addition to systemic antimicrobials, may represent a good treatment option with favorable visual outcomes for patients with syphilitic CNV, especially in the setting of syphilis reinfection or inadequate initial treatment of prior syphilis.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected health information was performed in a HIPAA (Health Insurance Portability and Accountability Act)-compliant manner.
Statement of Informed Consent
Informed consent was not necessary because the case described the care of one patient and excluded any personally identifiable information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.