
Abstract
Purpose:
Suprachoroidal hemorrhage is an uncommon but serious ocular condition that typically occurs in the setting of intraocular surgery and trauma. We present an external trans-conjunctival vitreoretinal trocar-cannula-based drainage of suprachoroidal hemorrhage as a viable surgical approach.
Methods:
Case report.
Results:
Trans-conjunctival trocar-cannula-based drainage of suprachoroidal hemorrhage is a safe and efficacious surgical approach to drainage of large choroidal hemorrhages.
Conclusions:
Although discrepancies persist regarding the optimal surgical approach to suprachoroidal hemorrhage management; herein, we describe the successful execution of an external trans-conjunctival vitreoretinal trocar-cannula-based drainage of suprachoroidal hemorrhage.
Introduction
Suprachoroidal hemorrhage (SCH) most commonly occurs during or following intraocular surgery or in the setting of trauma. SCH requires early recognition and appropriate monitoring to prevent severe vision loss. Fortunately, some cases of SCH are self-limited and can resolve spontaneously with careful observation. However, in cases of large, progressive, or appositional SCH, the need for surgical drainage is often necessary to prevent further complications such as retinal detachment, angle-closure glaucoma, retinal incarceration, or expulsion of intraocular contents, all of which can be associated with permanent vision loss and a guarded prognosis.1–3
The traditional approach to SCH drainage involved external drainage via a 2.0-mm to 3.0-mm sclerotomy window or tunnel at the apex of the choroidal detachment. In some instances, a cyclodialysis spatula can be introduced into the suprachoroidal space to expedite outflow. 1 Problematically, this technique can often result in postoperative leakage and hypotony, endophthalmitis, retinal incarceration, and the need for subsequent pars plana vitrectomy (PPV).
Here, we present external transconjunctival drainage of SCH using vitreoretinal trocar-cannulas on a patient with SCH following glaucoma surgery. This technique has the potential for improved efficiency, efficacy, and safety compared with previous drainage methods owing to the use of modern vitreoretinal instrumentation and technique.
Methods
Case Report
A 92-year-old woman presented with painful vision loss in the left eye and was found to have appositional (“kissing”) SCH following trabeculectomy surgery for advanced glaucoma (Figure 1). Past ocular history included selective laser trabeculoplasty, trabeculectomy with mitomycin C, and a Baerveldt glaucoma drainage device with scleral patch in the left eye. Presenting best-corrected visual acuity (VA) was counting fingers at 3 feet (1 m) with an intraocular pressure (IOP) of 8 mm Hg in the left eye. Anterior segment examination demonstrated pseudophakia, a well-positioned Baerveldt tube, and a 1-mm hyphema. The patient was monocular with hand motions VA OD secondary to advanced glaucoma. After discussing treatment options with the patient and her family, the decision for surgical drainage of the SCH in the left eye was made given the patient’s monocular status and persistent ocular pain in the left eye.
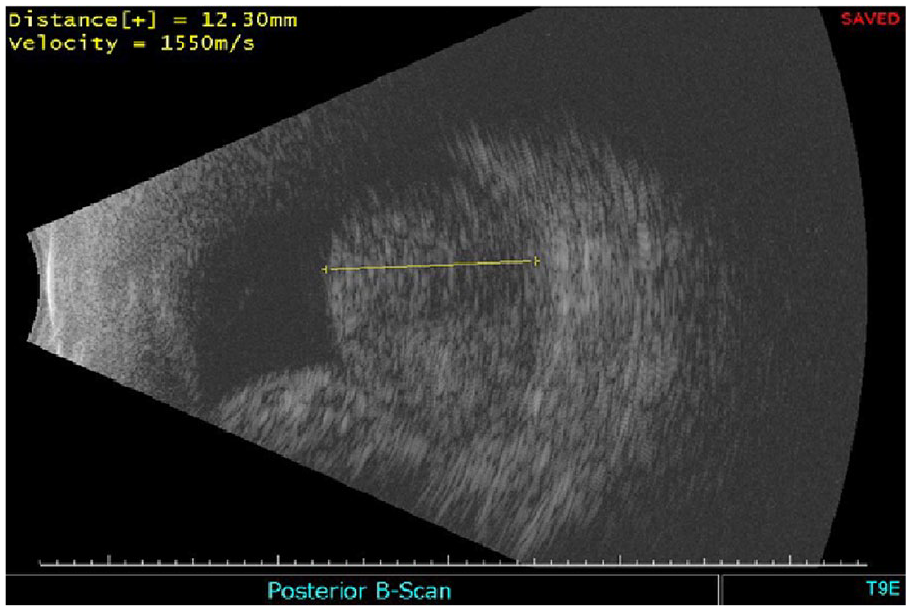
B-scan echography performed before surgical intervention demonstrates a large suprachoroidal hemorrhage with retinal contact in the left eye.
Surgical Technique
Preoperative B-scan echography was first performed to determine the ocular quadrant with the largest component of SCH. For optimal drainage, the quadrant with a SCH height greater than 5 mm was selected. Next, anterior infusion was secured at the corneal limbus using a 25-gauge trocar-cannula and the IOP was temporarily elevated to 60 mm Hg. We use the Alcon Constellation vitreoretinal unit and, with the infusion secured and the IOP elevated to 60 mm Hg, a 23-gauge nonvalved trocar-cannula is inserted approximately 7 mm posterior from the corneal limbus (ie, roughly near the functional equator) in the previously identified quadrant with the largest SCH component. Critical to technique success is that the trocar-cannula is inserted parallel to the functional equator and nearly flat or parallel to the conjunctiva and sclera with an angle of incidence of approximately 15° to 20°. The trocar-cannula should be positioned toward the functional equator to ensure proper positioning for drainage (Figure 2).
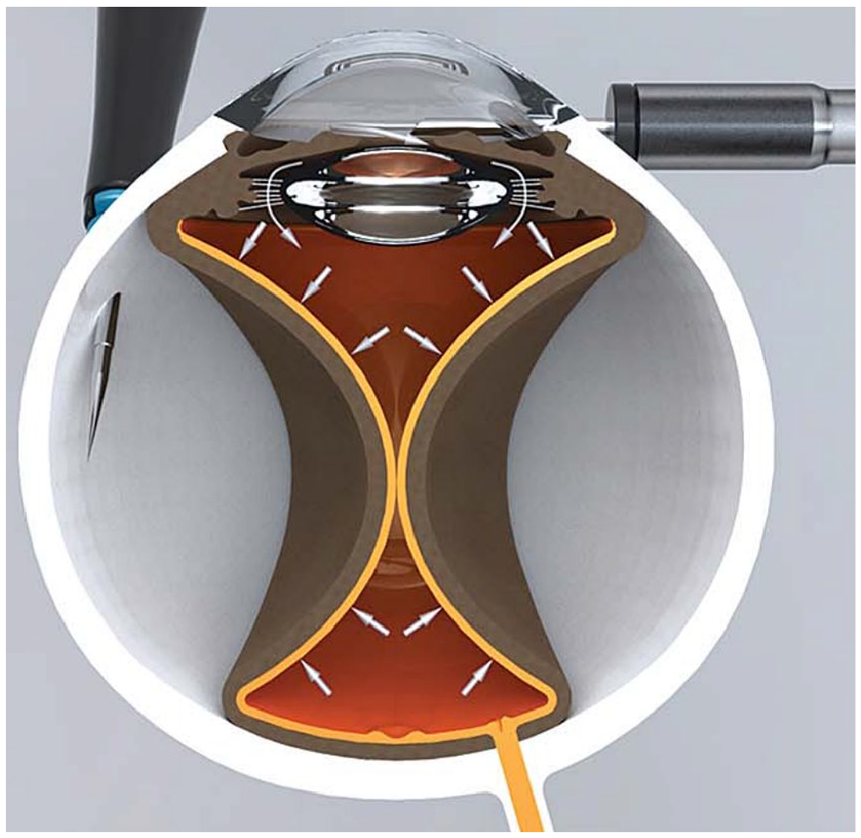
Schematic illustration demonstrating insertion of a vitreoretinal trocar-cannula at a flat angle of incidence (approximately 20°) to the sclera and positioned toward the functional equator.
Drainage of the SCH can proceed with minimal manipulation by means of the nonvalved 23-gauge cannula. Once the SCH is drained, the 23-gauge cannula can be removed, and we recommend leaving the drainage site open without suture closure. When required, PPV can be performed in eyes with concomitant pathology. You can find the complete surgical technique in the supplemental video file. The patient improved to a VA of 20/200 with stable IOP in the left eye.
Results
The technique described here provides a safe, efficient, efficacious, and reproducible surgical approach to management of SCH. Note that smaller-gauge 25-gauge trocars and/or valved trocars can be used for drainage; however, the drainage of blood may be slower and more likely to occlude with small blood clots. The sutureless approach makes use of beveled incisions to allow for slow, passive effusion and adequate drainage of the choroidal hemorrhage, minimizing the likelihood of postoperative hypotony sometimes seen in external drainage via larger sclerotomy wounds.
Several surgical pearls should be noted including avoiding drainage at the 3- and 9-o’clock meridians to spare possible iatrogenic trauma to the ciliary nerve. Moreover, if possible, it is advised to drain the inferotemporal quadrant as this will facilitate surgical access and be gravity dependent for optimal blood evacuation. Finally, if concomitant PPV is required, limbal-based vitrectomy (as shown in the supplemental video) is preferred to avoid instruments inadvertently entering the suprachoroidal space.
When PPV is performed after SCH drainage, if endotamponade is desired, we recommend avoiding air because choroidal formation and possible SCH often recur during this step. A noncompressible medium such as a balance salt solution or silicone oil will prevent choroidal formation from pushing fluid posteriorly and thereby protect the macula. Given the possibility of recurrent SCH, a noncompressible medium such as silicone oil or fluid offers the best mechanical approach to mitigating this risk.
Conclusions
We review a case and present the surgical management of SCH using external vitreoretinal trocar-cannula–based drainage. This is a safe and reproducible technique that affords vitreoretinal surgeons improved maneuverability when encountering these uncommon but challenging cases of SCH.
Footnotes
Authors’ Note
All authors attest that they meet the current ICMJE criteria for authorship.
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a HIPAA (Health Insurance Portability and Accountability Act)-compliant manner.
Statement of Informed Consent
Informed consent was obtained before performing the procedure, including permission for publication of all photographs and images included herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.