
Abstract
Keywords
Introduction
Amyloidosis refers to systemic disorders involving the deposition of insoluble misfolded polymer protein fibrils in various organs and tissues. Circulating precursors of amyloid proteins made by plasma cells, most commonly immunoglobulin light chain fragments, 1 can create misfolded protein oligomers and β-amyloid fibrils, disrupting tissue architecture and leading to tissue dysfunction. 2 Accumulation of the proteins commonly occurs in the heart, kidneys, liver, spleen, peripheral nervous system (PNS), musculoskeletal system, and upper gastrointestinal tract. The kidney, heart, and PNS are the most common sites of organ involvement at presentation in the United States. Common presenting symptoms include fatigue, weight loss, tissue edema, and paresthesia. 3
The median age of diagnosis in patients with amyloidosis is 63 years, with a 12-month survival time in untreated cases. 4 Cases can include familial amyloidotic polyneuropathy (FAP) as well as sporadic nonhereditary disease states. FAP is associated with a mutation in the transthyretin (TTR) gene (locus 18q11.2-q12.1) and inherited in an autosomal-dominant fashion. 5 Symptoms include nonischemic cardiomyopathy, albuminuria, peripheral neuropathy, hepatomegaly, carpal tunnel syndrome, tongue enlargement, and weight loss. 6 Diagnosis involves direct tissue biopsy (heart, bone marrow, fat pads) with Congo red staining for amyloid. Management mainstays center on bortezomib, daratumumab, dexamethasone, or high-dose melphalan chemotherapy followed by autologous blood stem-cell transplantation. Problematically, the condition is challenging to diagnose because of the low prevalence rate of 9 cases per million per year. 7
Vitreous involvement8 –11 can be seen in systemic amyloidosis with amyloid deposition in the vitreous appearing as diffuse whitish gray or yellowish material with a cobweb or cotton-wool appearance. Other fundus findings include perivascular deposits, superficial retinal gray–white deposits, and small-vessel occlusions with associated angiographic filling delays on fluorescein and indocyanine green angiography. 10 Here, we report a case of vitreous amyloidosis in the setting of a progressive decrease in visual acuity (VA) and persistent vitreous opacities in a patient with history of bilateral vitrectomy.
Methods
Case Report
A 69-year-old White woman presented with a 7-year history of blurred vision, fatigue, shortness of breath, and significant fluctuations in blood pressure. She reported an unintentional weight loss of 20 pounds over the previous 6 months. The patient’s medical history consisted of peripheral neuropathy, carpal tunnel syndrome, arthralgias, bowel and urinary incontinence, and pacemaker insertion 2 years previously for sick sinus syndrome. Her ocular history was significant for a previous pars plana vitrectomy (PPV) with endolaser for retinal neovascularization of unclear etiology in the right eye and PPV and membranectomy for persistent vitreous opacities and epiretinal membrane (ERM) in the left eye. She was being treated in the left eye for neovascular glaucoma. The treatment comprised brimonidine twice a day, dorzolamide/timolol twice a day, and prednisolone acetate 4 times a day.
The best-corrected VA was 20/70 OD and 20/100 OS with a mild relative afferent pupillary defect in the left eye. A slitlamp examination revealed moderate nuclear sclerotic cataract in the right eye with vitreous opacities in both eyes (Figure 1). A fundus examination of the right eye demonstrated blurred optic nerve margins and moderate sheathing of vessels with scattered peripheral retinal hemorrhages. The fundus examination of the left eye demonstrated mild pallor of the optic disc, vessel sclerosis, scattered peripheral retinal hemorrhages, ERM, and panretinal photocoagulation laser scars. These tests can be considered when formulating a formative diagnosis of vitreous amyloidosis.
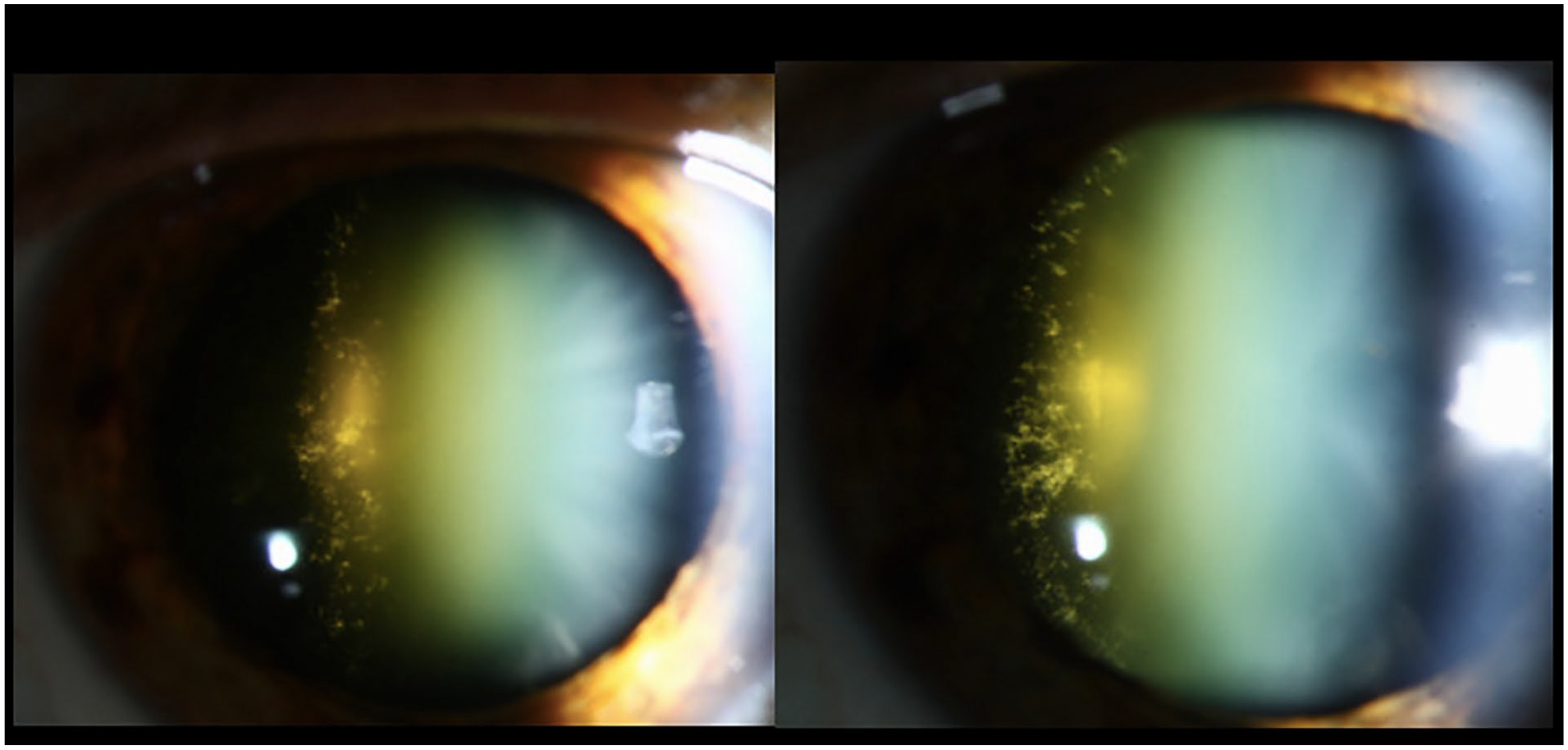
Slitlamp examination of the right eye shows retrolenticular opacities that appear granular and are strung along the vitreous fibrils.
Initial vitreous biopsies performed 4 years (left eye) and 6 years (right eye) after initial presentation by referring physicians were negative in both eyes in the setting of previous vitrectomy in both eyes. Optical coherence tomography showed mild cystoid macular edema in both eyes (Figure 2). On further ancillary testing, head computed tomography imaging showed bilateral medial rectus infiltration with enlarged proximal intraconal optic nerves. A lumbar puncture revealed elevated protein, and serum electrophoresis showed a mildly elevated kappa-free light chain. On further investigation into the significant systemic presence of protein deposits in the cerebrospinal fluid, conduction of a fat pad biopsy with Congo red staining under polarized light microscopy was performed within the year of the second negative vitreous biopsy (of the right eye). Fibroadipose tissue with small vessels showing congophilic amyloid deposition with apple-green birefringence (Figure 3) was found, confirming the diagnosis of ocular amyloidosis.
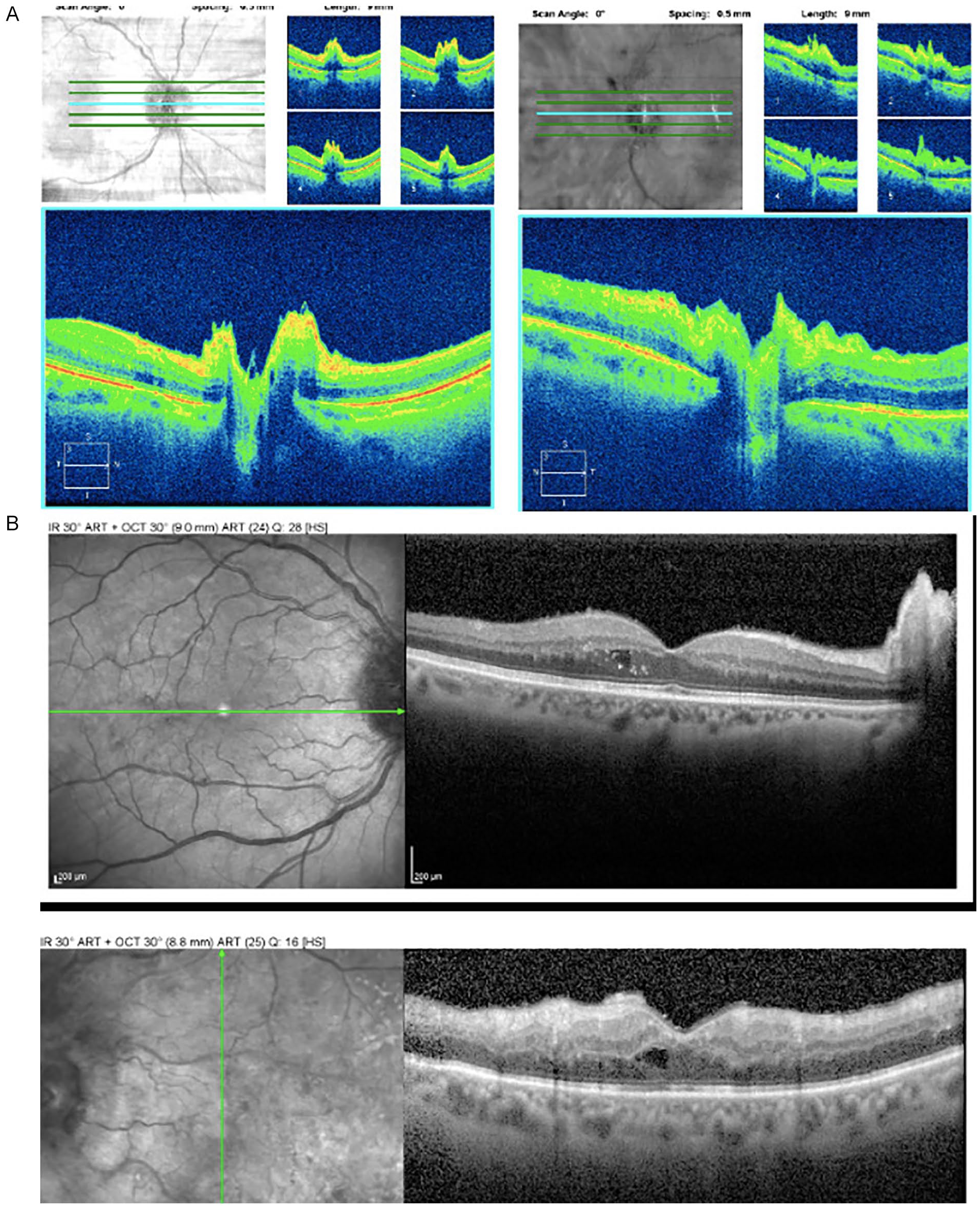
(A) Optical coherence tomography (OCT) (Cirrus, Zeiss) of the optic nerve in both eyes indicating mild infiltration of the optic nerve in both eyes. (B) OCT (Heidelberg Spectralis, Heidelberg) in the macula in both eyes indicating mild cystoid macular edema.
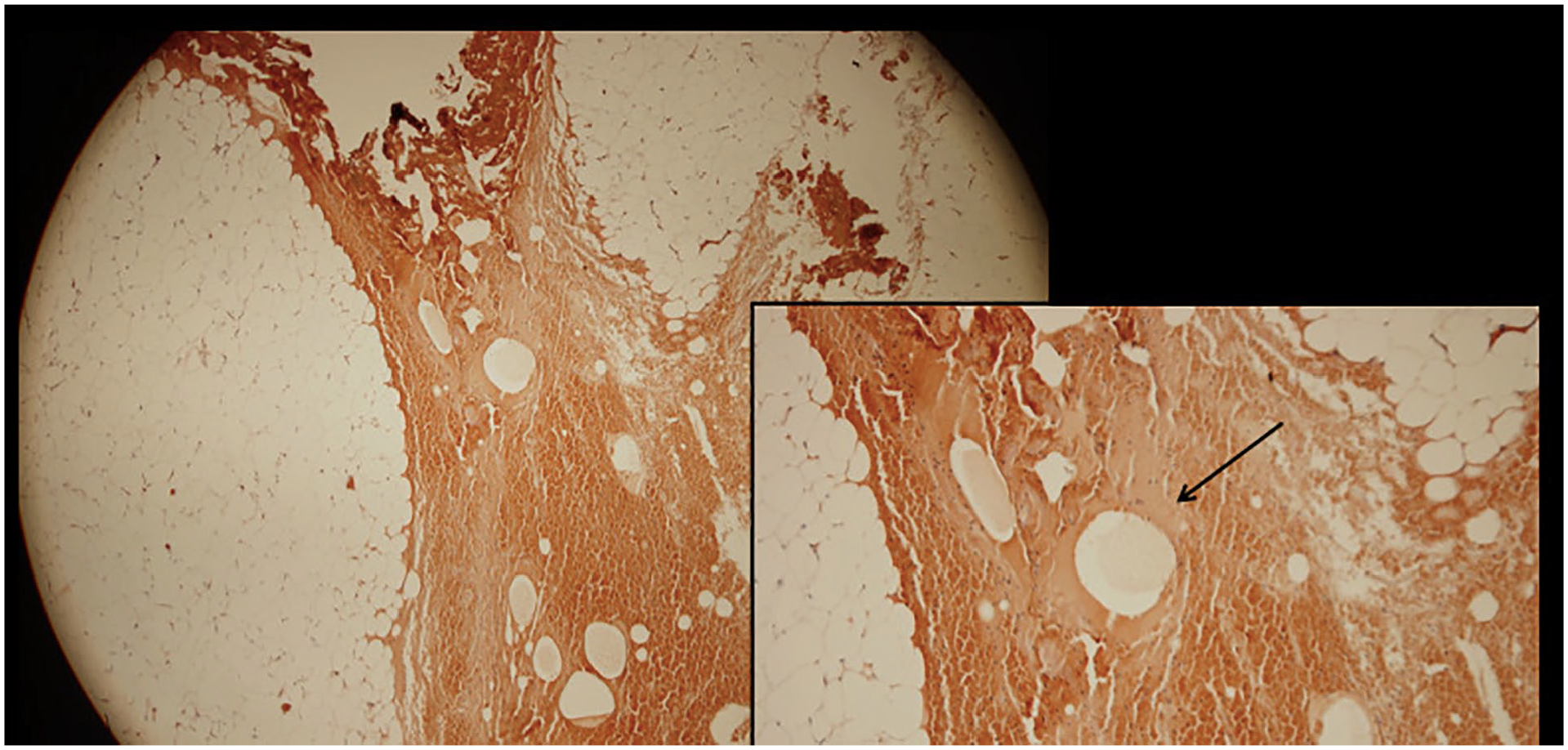
Congo red stain of fibroadipose tissue with small vessels showing congophilic amyloid deposition.
Results
This case study highlights the challenges ophthalmologists face in diagnosing ocular amyloidosis. The constellation of typical constitutional symptoms and examination findings, including vitreous opacities, retinal neovascularization, and cataracts, can be nonspecific and cause substantial delays in diagnosis. Systemic amyloidosis can have several systemic manifestations and might be difficult to diagnose in certain situations. The complex pathology of amyloidosis requires clinicians to be aware of the masquerading effect of amyloidosis.
The signs and symptoms that raise suspicion for a diagnosis of vitreous amyloidosis are often nonspecific. In comparable clinical presentations, myriad disease conditions of varying etiologies are often considered in the differential, including those inflammatory, infectious, infiltrative, or neoplastic in nature (eg, vitreous hemorrhage, uveitis, multiple myeloma, crystalline retinopathy, asteroid hyalosis, and synchysis scintillans). Although it is a difficult task, identifying patients with amyloidosis early through understanding the pathology and referring them for further evaluation and fatpad biopsy can mitigate a delay in diagnosis and further exacerbations. Therefore, a thorough review of systems and uncovering manifestations in other organ systems is an integral factor in considering the diagnosis of amyloidosis.
In our case, making the diagnosis was met with an additional level of difficulty; that is, vitreous biopsies performed 2 years apart were negative despite the systemic presence of amyloid plaques. This was likely because the patient had previous vitrectomies in both eyes. It is essential to note the additional roadblock of negative biopsies to the diagnosis of vitreous amyloidosis because patients with similar presentations of persistent vitreous opacities might have had previous intraocular surgery, leading to false-negative biopsies.
Conclusions
Amyloidosis of the vitreous cam be primary, acquired, or familial and should be considered in the differential diagnosis of vitreous opacities. FAPs are rare forms of amyloidosis that have been associated with amyloid accumulation in the vitreous. 11 Although they are not often seen, an early accurate diagnosis might improve the patient’s life expectancy as well as the quality of life.
Footnotes
Authors’ Note
All authors attest that they meet the current ICMJE criteria for authorship.
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a HIPAA (Health Insurance Portability and Accountability Act)–compliant manner.
Statement of Informed Consent
Informed consent was obtained prior to performing the procedure, including permission for publication of all photographs and images included herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.