
Abstract
Introduction
Retinal detachments (RDs) are among the sight-threatening conditions encountered in a vitreoretinal clinic. The estimated incidence of an RD is approximately 6.3 to 17.9 per 100 000 population, with 7.26% of patients developing bilateral detachments. 1 If the detachment involves the macula, there is a potential for significant, permanent vision loss. 2 Visual decline can affect the length and quality of life, increasing the risk of fractures, depression, and social isolation. 3 RD repair is considered emergent or urgent and can be performed with a variety of techniques, most commonly a pars plana vitrectomy with or without a scleral buckle. 4
The US Centers for Medicare and Medicaid Services (CMS) determines physician reimbursement rates based on estimated physician work, practice expenses, and medical liabilities, which are each assigned a relative value unit (RVU). The physician work relative value unit (wRVU) is based on the time spent and the intensity of work and skills required by the physician. 5 The value of an RVU is converted into a dollar reimbursement based on the conversion factor and is reevaluated yearly by CMS. There has been a trend toward increasing the value for office-based care in recent years to increase payments for primary care. With mandated budget neutrality, these increases have resulted in a trend toward progressive devaluation of surgical procedures.6,7
The purpose of the current analysis was to determine the opportunity cost for a retinal surgeon performing an uncomplicated RD surgery and managing the patient in the global perioperative period compared with the opportunity cost for office-based patient care in equivalent time.
Methods
Theoretical Model
A theoretical model was constructed using TreeAgePro (TreeAge Software LLC). Institutional review board approval was not required because the study did not involve human subjects.
CMS set the 2019 physician reimbursement for RD repair (Current Procedural Terminology [CPT] code 67108) at 34.10 wRVUs (consisting of 17.13 physician wRVUs + 15.73 practice expense RVUs + 1.24 malpractice RVUs). The analysis was performed from the physician work perspective, so practice expenses and medicolegal liabilities, which each have separate wRVU allocations by CMS, were not evaluated.
The reference case was a vitreoretinal surgeon performing 67108 RD repair in the time and with the number of postoperative visits allocated by CMS.8,9 For 67108, CMS allocated 33 minutes for preoperative care to account for review of the medical record and diagnostic testing, preoperative orders, and the informed consent process; 128 minutes were allocated for intraoperative time, consisting of 90 minutes of “median intraservice time” (from surgery incision to closure) and 38 minutes of immediate perioperative care, consisting of 3 minutes “prepositioning time,” 15 minutes “preservice scrub dress wait time,” and 20 minutes “postservice time.” For 67108, CMS allocated 5 postoperative visits within the 90-day global period. 8
The current model calculated the potential wRVUs for office-based productivity in the equivalent global period with the following formula:
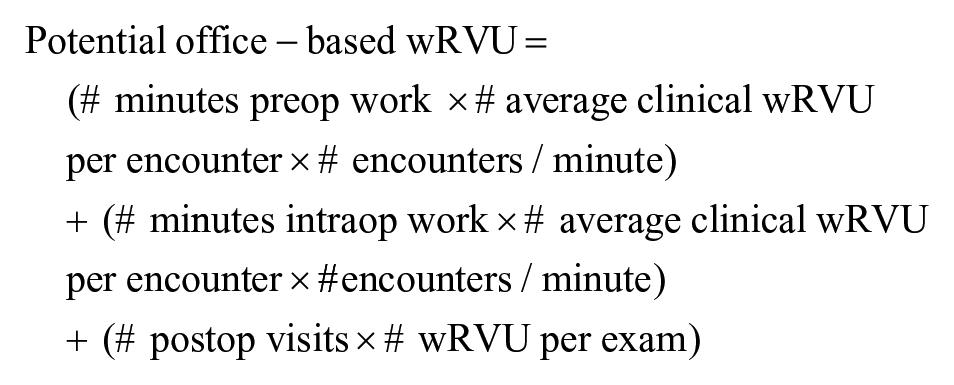
In the aforementioned formula, the valuation for preoperative cost and intraoperative cost was based on the potential office productivity that could have been otherwise generated during the CMS-allocated preoperative time period and intraoperative duration (intraoperative defined as intraservice + immediate perioperative work). Potential office productivity was estimated through analysis of the Vestrum Health retina database (Vestrum Health LLC). The database partnered with 65 geographically diverse practices in 2019 throughout the United States, consisting of 358 distinct retina specialists. From each of these practices, the electronic medical records of more than 2.4 million patients in 2019 were collected for analysis and practice reporting.
In this study, aggregated real-world data were analyzed to identify the total wRVUs (inclusive of all evaluation and management [E/M] codes, imaging, procedures, diagnostic testing, etc) coded into the database from January 1, 2019, through December 31, 2019, along with the total number of patient encounters in the same period; these data were used to identify the means and interquartile ranges (IQRs) of wRVUs coded per encounter. CMS defined the preoperative time as 33 minutes and the intraoperative time as 128 minutes (90 minutes intraservice time + 38 minutes immediate perioperative work). 8 The number of office patient encounters per hour was modeled with assumptions and was varied.
The valuation for postoperative cost in the formula was based on the potential office productivity that could have been generated instead of the postoperative visits included in the global period for surgery. In contrast to the valuation for intraoperative work, which accounted for all potential office-based work that could have been otherwise performed during the surgery time, the valuation for postoperative visits was based on E/M codes only for established patient examination visits (CPT 99211-5, 92012, and 92014). New patient visits were excluded because it was assumed that the physician work involved with postoperative visits is more closely represented by an established visit of varying time or intensity, depending on the postoperative circumstances. Ancillary wRVUs, such as from imaging, procedures, and diagnostic testing, were also excluded because they might be billed separately in the global period. Real-world aggregated data from the retinal database were used to identify a weighted average of the frequency of CPT codes 99211, 99212, 99213, 99214, 99215, 92012, and 92014 during January 1, 2019, through December 31, 2019, which were multiplied by their wRVU values to identify the mean and IQRs of wRVUs coded per examination. CMS allocated 5 postoperative visits in the 67108 global period. 10
The opportunity cost associated with surgery was expressed as a percentage of potential office-based productivity (ie, opportunity cost = 1 − [CMS-allocated wRVUs for surgery]/[potential office-based wRVUs]).
In the model for clinical productivity, the reference case assumed an average of 40 patients per 8 hours of office-based care (5 patients/hour, or 0.0833 patients/minute) and used the mean Vestrum-derived wRVU per encounter and wRVU per examination. A less busy clinician was modeled as seeing 30 patients over 8 hours (3.75 patients/hour, or 0.0625 patients/minute) and used the lower IQR of Vestrum-derived wRVU per encounter and wRVU per examination. A busier and more efficient (reported here as “busier”) clinician was modeled as seeing 50 patients over 8 hours (6.25 patients/hour, or 0.104 patients/minute), with the upper value of the IQR for Vestrum-derived wRVU per encounter and wRVU per examination. Table 1 shows the variables.
Physician Reimbursement for Retinal Detachment Repair. a
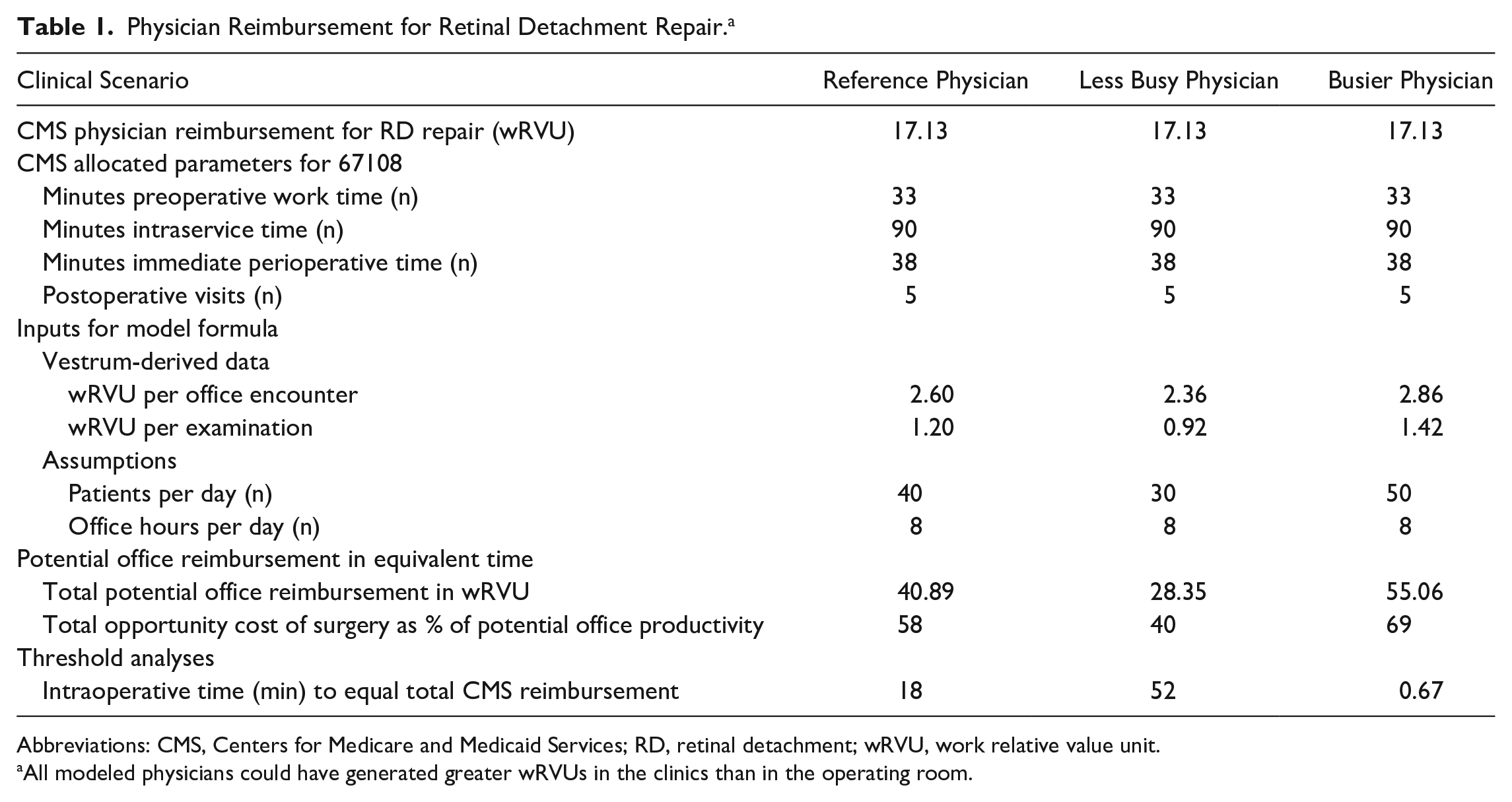
Abbreviations: CMS, Centers for Medicare and Medicaid Services; RD, retinal detachment; wRVU, work relative value unit.
All modeled physicians could have generated greater wRVUs in the clinics than in the operating room.
Threshold Analyses
Threshold analyses were performed to identify the intraoperative duration that would render lost office-based productivity equal to CMS reimbursements. Specifically, the threshold analysis determined the intraoperative duration, including intraservice time and the immediate perioperative work time, required for the wRVU value of lost office-based productivity to equal the total CMS reimbursement, assuming 5 postoperative office visits.
Probability Sensitivity Analyses
Probability sensitivity analyses were performed to assess for uncertainty with Monte Carlo simulations using 100 000 second-order parameter samples. The model was assessed through a broad range of surgical and clinical conditions, varying the preoperative time (15-45 minutes), intraservice time (30-120 minutes), immediate perioperative time (20-60 minutes), clinic volume (30-50 patients per 8-hour day), number of postoperative visits (3-7), and clinical productivity (using Vestrum-derived IQRs of RVU productivity per office encounter and per examination).
Results
Analysis of the Vestrum database identified a mean of 2.60 wRVUs per office encounter (IQR, 2.36-2.86 wRVUs), which was used to model potential lost clinical productivity during the equivalent preoperative period and intraoperative period. This lost productivity factors all potential work performed in the office, inclusive of all new and established E/M of varying levels of intensity along with imaging (eg, optical coherence tomography, fluorescein and/or indocyanine green angiograms, ultrasound), diagnostic testing (eg, electroretinograms and visual field testing), and office-based procedures (eg, extended ophthalmoscopy, lasers [eg, for retinal tears, proliferative diabetic retinopathy, diabetic macular edema], intravitreal injections, vitreous biopsies, and pneumatic retinopexy).
The database also identified a mean of 1.20 wRVUs per any established patient examination visit (IQR, 0.92-1.42 wRVUs), which was used to model potential clinical productivity during the equivalent postoperative period; only E/M codes were factored because other services, such as imaging and procedures, might be separately billed during the global period. The CMS valuation of 67108 surgery was 17.13 wRVUs.
The physician in the reference case, who saw 40 patients in an 8-hour clinic day, maintained a mean RVU productivity (2.60 wRVUs per office encounter and 1.20 wRVUs per examination), per CMS allocations operated in 90 minutes with 33 minutes of preoperative work and 38 minutes of immediate perioperative work, and used 5 postoperative visits in the global period, could have generated 40.89 wRVUs in the office during the equivalent global period. Based on these reference CMS allocations, the opportunity cost for performing surgery was 58% compared with potential office-based productivity. In the threshold analysis, the surgeon in the reference case would have 18 minutes to complete surgery and all immediate perioperative care, assuming a preoperative work time of 33 minutes and 5 postoperative visits, for lost office productivity to equal the total CMS valuation for surgery. Figure 1 shows the inverse relationship between surgical time and the total potential wRVUs that could have been produced in the office during the equivalent time.
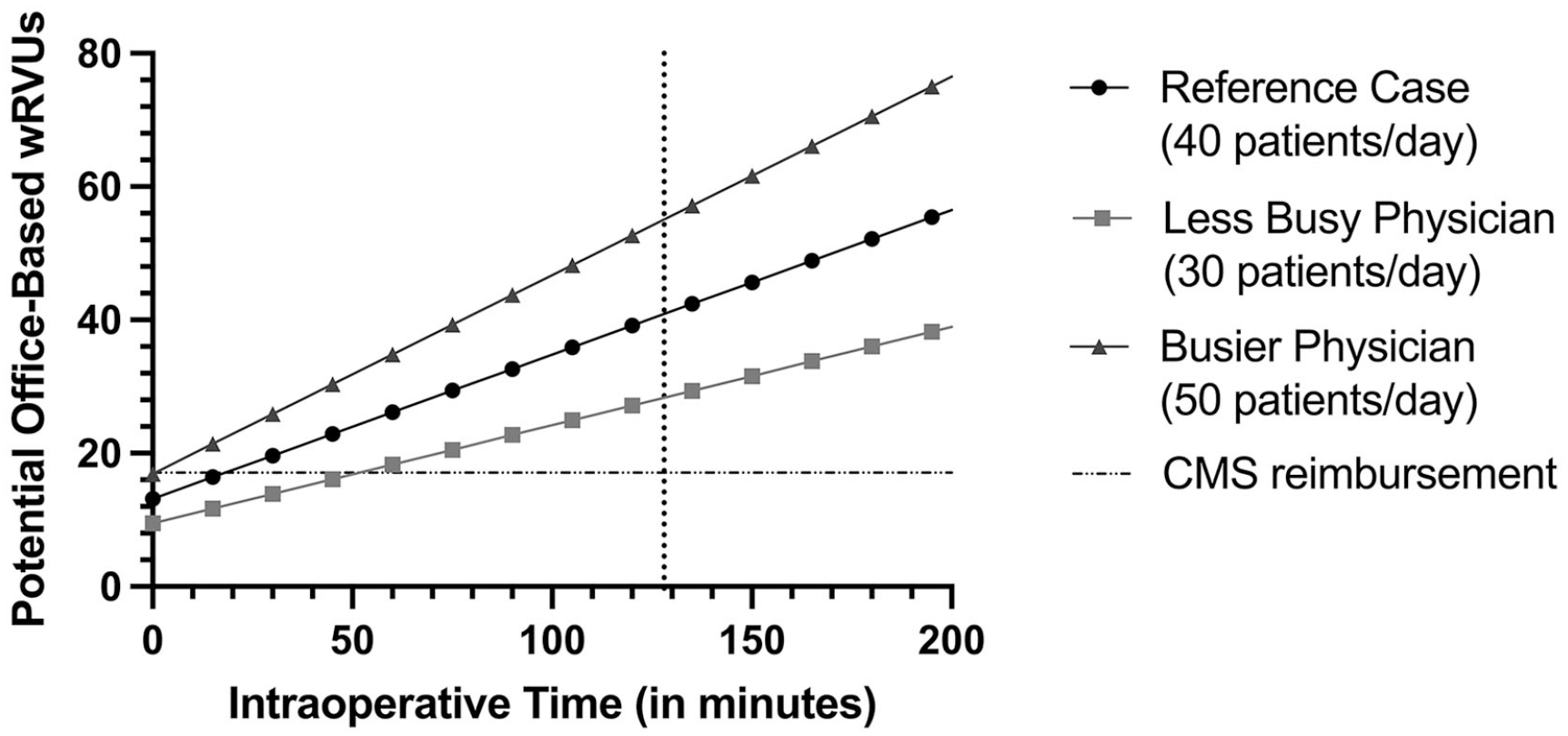
Potential total office-based work relative value units (wRVUs). The sloped lines represent the total potential office-based wRVUs that could have been produced during the 67108 surgery and its global period for the reference case (surgeon managing 40 patients/day), the less busy physician (30 patients/day), and the busier physician (50 patients/day). The vertical dotted line represents 128 minutes of intraoperative time (90 minutes intraservice time + 38 minutes immediate perioperative work time) allocated by the Centers for Medicare and Medicaid Services (CMS), and the horizontal dashed line represents the current CMS reimbursement of 17.13 wRVUs. The intersection of the solid sloped lines and the dashed horizontal line is the threshold value of intraoperative time (ie, intraservice + immediate perioperative time) to equal clinical productivity.
A second scenario was modeled with a less busy physician, who saw 30 patients per 8-hour day, was at the lower quartile of RVU productivity (2.36 wRVUs per office encounter and 0.92 wRVUs per examination), operated in 90 minutes with 33 minutes of preoperative work and 38 minutes of immediate perioperative work, and performed 5 postoperative visits in the global period per CMS allocations. This physician could have generated 28.35 wRVUs in the office during the equivalent global period, representing an opportunity cost of 40% of potential office-based productivity. For lost office productivity to equal the total CMS valuation for surgery, this less busy surgeon would have to complete the surgical procedure and all immediate perioperative care within 52 minutes, assuming a preoperative work time of 33 minutes and 5 postoperative visits.
A third scenario was modeled with a busier physician, who saw 50 patients per 8-hour day, was at the higher quartile of RVU productivity (2.86 wRVUs per office encounter and 1.42 wRVUs per examination), operated in 90 minutes with 33 minutes of preoperative work and 38 minutes of immediate perioperative work, and performed 5 postoperative visits in the global period per CMS allocations. The busier physician could have generated 55.06 wRVUs in the office during the equivalent global period, representing an opportunity cost of 69% of potential office-based productivity. In the threshold analysis assuming 33 minutes of preoperative work and 5 postoperative visits, the more efficient surgeon would have to complete surgery and all immediate perioperative care in less than 1 minute for lost office productivity to equal the total CMS valuation for surgery.
In the probability sensitivity analyses, the preoperative work time varied from 15 to 45 minutes, the intraservice time from 30 to 120 minutes, the immediate perioperative care from 20 to 60 minutes, the clinic volume from 30 to 50 patients per 8-hour day, the number of postoperative visits from 3 to 7, the average value of clinical visits from 2.36 to 2.86 wRVUs, and the average value of postoperative visits from 0.92 to 1.42 wRVUs. Clinical reimbursements for outpatient office-based practice exceeded surgical reimbursements in approximately 99% of the clinical scenarios.
Conclusions
Surgical advances have increased the success rates of RD repair, decreased surgical times and postoperative complications, and have decreased the overall cost burden to the health care system. In cost-utility analyses, RD repairs were found to be cost-effective and associated with gains in quality-adjusted life years and increases in utility values.11–13
Although vitreoretinal surgical times, in-patient hospitalizations, and in-patient surgeries have declined over the years, decreasing the costs for the health care payer, 14 the current model identified significant opportunity cost for the physician for performing CPT code 67108 surgery (RD repair) compared with office-based care of equivalent time. Losses associated with performing surgery were modeled as 58% of potential clinical productivity in the reference case and 69% for the busier modeled clinician. Even the less busy clinician in the model experienced a loss of 40% of potential clinical productivity associated with performing CPT code 67108 surgery. Varying clinical conditions still resulted in opportunity costs associated with 67108 surgery in 99% of scenarios.
Threshold analyses indicated that the reference surgeon would have to complete the surgery and all immediate perioperative care with a surgical turnover within 18 minutes to neutralize this opportunity cost. The threshold time was less than 1 minute for the busier clinician, and to avoid losses, even the least busy clinician in the model would have to complete surgery in significantly less time than that allocated by CMS. For any surgery, in particular 67108 surgery, which includes a vitrectomy with (and without) a scleral buckle, these average threshold times might be extremely difficult or impossible to achieve.
These results suggest that from a purely financial perspective, vitreoretinal surgeons are reimbursed higher by CMS for managing patients in the clinic than for repairing RDs in the operating room. The discrepancy is likely a result of undervaluation of vitreoretinal surgery along with the nature of tertiary subspecialty office-based care for many of the patients seen by retina specialists. These patients have complex chronic diseases that require ancillary imaging, diagnostic testing, and office-based procedures (eg, intravitreal injections and laser procedures) to treat appropriately.
Undervaluation of vitreoretinal surgery has been explored in healthcare systems from a variety of perspectives, with disproportionality between reimbursement rates and costs. In an academic hospital setting in the United States, the costs of vitrectomy surgery were found to be less than CMS reimbursements from the healthcare institution’s perspective.15,16 In the United Kingdom, the cost of vitreoretinal surgery for macular holes, epiretinal membranes, and vitreomacular traction were similarly less than healthcare payer reimbursements. 17 Even from the patient perspective, undervaluation of vitreoretinal surgery has been shown. Although patients considered physician reimbursements of up $14,115 to be reasonable for an RD repair, the actual physician reimbursement by CMS ($1683) was significantly lower. 18 When surgical reimbursements were adjusted for inflation, the overall decline was even greater. 19
Limitations of the current study include the theoretical nature and the assumptions made in the model. Coding data from the Vestrum database were used whenever possible to best simulate real-world practices. The database represents a geographically diverse and large group of retinal specialists; however, coding data might not fully reflect actual reimbursements from insurers. Furthermore, 2019 data were used because sufficient data from 2021 were not available at the time of the current analysis and 2020 practice patterns likely were profoundly altered as a result of the COVID-19 global pandemic.
Although it might be possible that 2019 data do not accurately reflect 2021 billing practices, the wRVU valuation for 67108 surgery has not changed since 2016. Moreover, in 2021, CMS made upward adjustments to the reimbursement schedules for stand-alone E/M codes, with up to 46% increases in wRVU valuations for certain codes and 19% increases on average across all E/M codes. These upward adjustments were not similarly applied to visits in the postoperative global period. Postoperative surgery care is already undervalued according to the current model using 2019 values. The undervaluation is further amplified by these 2021 changes, giving even higher reimbursements for office-based care than for surgical care with a 10-day or 90-day global period, which includes 1 or more postoperative E/M office visits. In addition, the model assumed that physicians worked an 8-hour day; however, busier clinics, emergency cases, after-hours charting, or patient telephone calls might change the total hours worked and the hourly patient volume on which the model is based.
Modeling is also inherently restrictive, and the current model of uncomplicated RD repair did not account for postoperative complications, which would likely increase the opportunity costs associated with surgery; this warrants further investigation. The model did not account for the significant but intangible costs associated with surgery, such as the stress, inefficiencies, and work–life balance costs of performing emergency surgery or managing postoperative complications. The model also did not account for intangible benefits beyond reimbursement, such as potentially increased patient referrals for a physician who can perform surgery in addition to office-based care.
The estimated costs and perioperative times could also differ if the patient had surgery in a hospital facility, particularly after-hours, compared to an ambulatory surgery center. Of note, the current analysis applied only to CPT code 67108; similar analyses would have to be performed to determine whether other surgeries were associated with losses relative to office-based patient care.
In conclusion, the current model indicated that surgical reimbursement for an RD repair was significantly less than the equivalent reimbursement for office-based patient care during the same time period. Although a reduction in surgery time could minimize this opportunity cost, modeled threshold times would likely not be achievable. Greater efficiency with in-office patient care along with declining surgery reimbursements over the past decade might discourage clinically busy physicians.
Footnotes
Ethical Approval
Institutional review board approval was not required because the study did not involve human subjects.
Statement of Informed Consent
Informed consent was not required because the study did not involve human subjects.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.