
Abstract
Introduction
Tractional retinal detachment (TRD) is a potentially blinding complication of advanced diabetes. 1 Chronic uncontrolled hyperglycemia and ischemia lead to hypersecretion of vascular endothelial growth factor (VEGF), angiopoietin-2, and fibroproliferative mediators.2,3 Subsequent extension of neovascular membranes onto the vitreous scaffold creates an adhesive tether at the vitreoretinal interface. Progression of neovascular membranes often leads to contraction and eventual detachment of the neurosensory retina from its underlying choroid.1–4
Given that the goal of TRD management is to relieve the mechanical traction on the retina, pars plana vitrectomy (PPV) remains the primary treatment for diabetic TRD.1,5 TRD repair has been documented with all currently available vitrectomy gauges. Minimally invasive vitrectomy surgery with 23-gauge or 25-gauge systems has been the most popular and well-studied approach recently.1,6–8 Outcomes data for 27-gauge PPV repair of diabetic TRD, however, are limited.
Introduced in 2010, 27-gauge vitrectomy has gained popularity for a variety of vitreoretinal conditions, including epiretinal membranes, rhegmatogenous RDs (RRDs), macular holes, and vitreous hemorrhages.9–14 It is reported to provide outcomes similar to those of 23-gauge and 25-gauge systems with respect to anatomic success, visual acuity (VA), and postoperative complications.13,14 The benefits of 27-gauge PPV include faster wound closure, fewer cases of hypotony, and improved patient comfort, even in more complex cases.9–14 The smaller gauge instrumentation used in 27-gauge PPV enables more surgical precision and control because of the smaller distance between the opening of the cutter and the tip of the instrument, which allows the surgeon to use it as scissors during dissection at the retinal surface in diabetic TRD repair. 15
Despite the potential benefits of 27-gauge PPV for diabetic TRD, there has not been wide acceptance of this surgical modality and there is a paucity of outcomes reported in the literature.15,16 The goal of this study was to assess 27-gauge PPV for diabetic TRD repair and evaluate the preoperative and perioperative variables that might affect visual recovery and anatomic success.
Methods
This single-center retrospective interventional case series analysis comprised consecutive patients with diabetic TRD who had 27-gauge PPV performed by the same surgeon from 2016 to 2020. This research was approved by the Institutional Review Board, University of Virginia; adhered to the tenets of the Declaration of Helsinki; and was conducted in accordance with regulations set forth by the US Health Insurance Portability and Accountability Act (HIPAA). A HIPAA-complaint database was queried to obtain medical records, including medical history, surgical history, and postoperative outcomes data.
Data Collection
Included were all patients aged 18 years or older with history of significant diabetic vitreoretinal traction with or without detachment repaired with 27-gauge PPV who had a minimum follow-up of 6 months. Excluded were patients with previous vitrectomy or 27-gauge PPV performed for other indications. Baseline patient data included demographics, baseline clinical and medical characteristics, underlying eye pathology, and operative details. Outcomes data included logMAR VA, with severe visual impairment defined as 20/200 or worse (logMAR > 1.0) and good vision defined as 20/40 or better (logMAR < 0.3); retinal attachment status; and complications. These data were collected when available from postoperative day 1, week 1, month 1, month 3, month 6, and year 1 and from the final documented visit.
Tractional Retinal Detachment Grading System
A severity classification system was proposed based on the extent of RD using multimodal imaging (optical coherence tomography [OCT], B-scan, fundus photographs), baseline examination data, and intraoperative examination data. The classification was as follows: grade A = vitreoretinal traction without detachment; grade B = evidence of extramacular detachment; grade C = macular involvement by the detachment; grade D = detachment involving the posterior pole and extending beyond the equator up to total RD. OCT imaging was preferably used to identify and classify detachment, specifically grades A and B, while B-scans were used to identify and classify grades C and D when OCT could not be obtained (Figure 1).
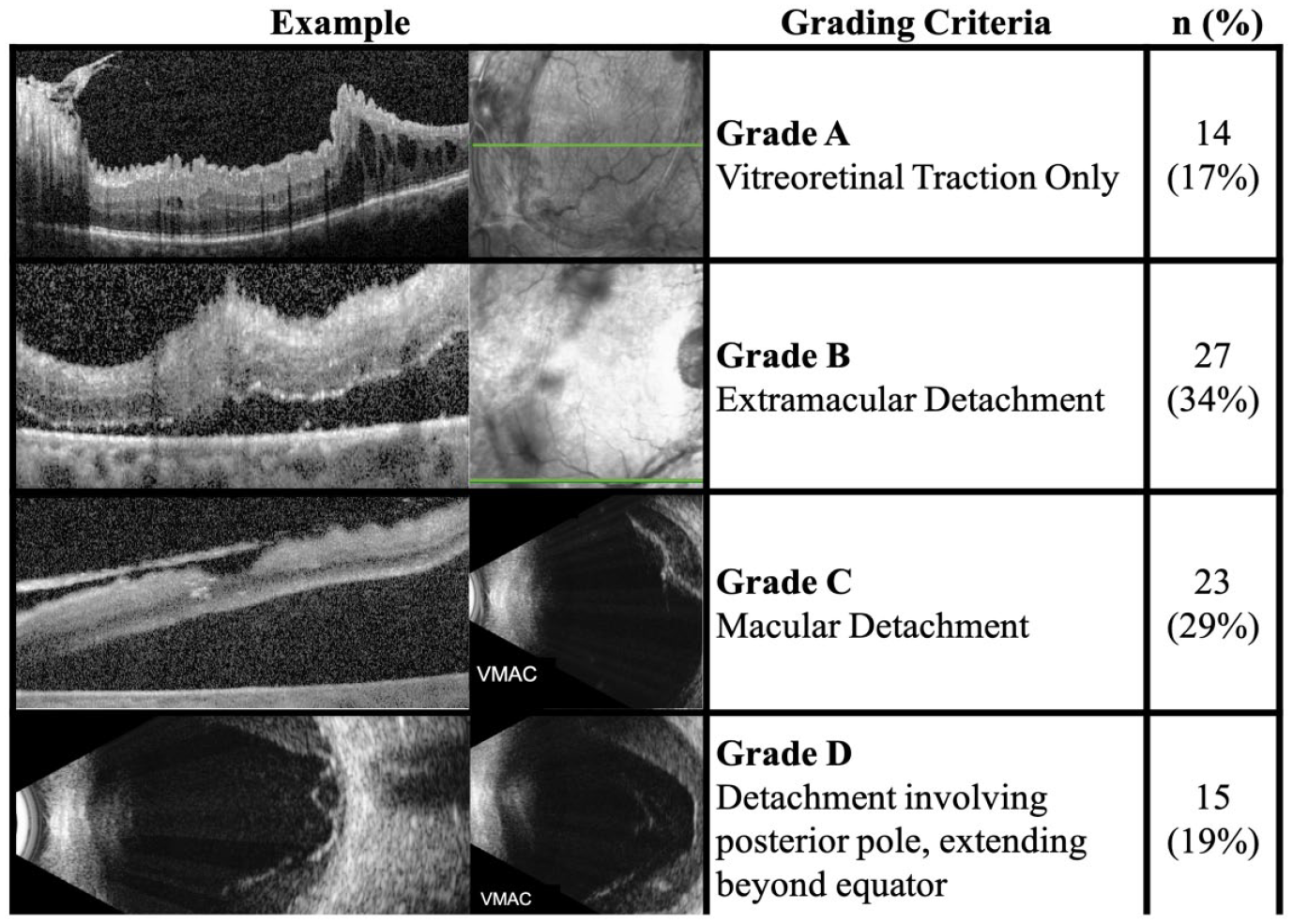
Characterization of tractional retinal detachment severity.
Surgical Technique
All surgeries were performed by the same surgeon with assistance from a surgical fellow as previously described. 17 Given that many patients in this cohort were traveling from far distances and had multiple comorbidities, pretreatment with anti-VEGF was deferred to avoid inducing a crunch syndrome in case surgery was delayed. In all cases, a standard 3-port vitrectomy was performed using a 27-gauge EVA system (Dutch Ophthalmic Research Center). Multi-gauge (single 23-gauge cannula) vitrectomy was used in eyes requiring silicone oil (SO) infusion. Patients were under general anesthesia or received monitored anesthesia care.
The 27-gauge trocars were placed in a standard fashion. Core and peripheral vitrectomy was performed in all cases at 15 000 cuts per minute. At 680 mm Hg vacuum, a maximum aspiration of 9 mL/min was achieved. When required, membrane dissection was performed with the vitreous cutter on shave mode using delamination and segmentation techniques with the vitrector acting as scissors via the Pac-Man approach or in-plane lift-and-shave approach as described by Berrocal. 18 Peripheral dissection was limited in cases of peripheral traction that involved thin/atrophic retina not extending to the macula. A forceps was rarely used and only for developing or elevating membrane edges.
The decision to perform retinotomy, often superonasally, was based on the presence of significant subretinal fluid that induced folds in the macula during fluid–air exchange. Fluid–air exchange was performed, and a soft-tipped cannula was used for endodrainage in these cases. Panretinal photocoagulation with an endolaser was performed for 360 degrees and around retinal breaks. Filtered air or 20% sulfur hexafluoride (SF6) was used as a tamponade agent in patients with no identified retinal breaks. If a retinal break was identified or a retinotomy created, 14% to 16% perfluoropropane (C3F8) was used. SO was reserved for complex RDs that could not be flattened, in which case a 23-gauge cannula was used for oil infusion. Sclerotomies were typically self-sealing; however, 7-0 polyglactin suture was used to close sclerotomies if SO was infused. Intraoperative bevacizumab was injected in most cases.
Statistical Analysis
Statistical analyses were performed using SPSS statistics software (version 28.0.1.1, IBM). Figures and tables were created using Excel and Powerpoint software (2016, Microsoft Corp). Primary outcomes analyzed included retinal reattachment, VA, intraocular pressure, and complications, including endophthalmitis, hyphema, cystoid macular edema (CME), and persisting vitreous hemorrhage. Retinal reattachment was defined as macular attachment postoperatively that allowed for persistent pockets of submacular fluid less than 1 disc diameter. Descriptive and comparative statistics, including univariate and multivariate regression models, were used for estimating predictors of outcomes.
A 1-sided paired t test was used to evaluate the overall postoperative change in the mean logMAR VA from baseline. An independent-sample t test with the Levene test for equality of variance or 1-way analysis of variance with Tukey post hoc testing was used to compare the mean VA between groups at specific timepoints. Pearson chi-square tests were used to compare frequencies between preoperative and postoperative categorical variables and outcomes. Linear regression was used to evaluate predictors of postoperative VA, while binary logistic regression was used to evaluate predictors of redetachment and complications.
Potential prognostic factors analyzed included the preoperative VA, ocular history, diabetic history (duration in years, preoperative glycolated hemoglobin (HbA1c), duration of insulin use, history of amputation, other signs of end organ dysfunction), medical history (hypertension, dialysis use, evidence of major adverse cardiac event), and detachment severity grade. A P value less than 0.05 was considered statistically significant. A Bonferroni correction for multiple comparisons was applied when applicable. The VA is reported as the mean logMAR ± SD (Snellen equivalent). Other continuous variables are reported as the median, mean ± SD, and range.
Results
Baseline Features
Of the 110 eyes screened, 79 eyes of 79 patients with diabetic TRD met the inclusion criteria. The median age of the 44 women (55.7%) and 35 men (44.3%) at the time of surgery was 46.5 years (Table 1). The median follow-up was 17 months (mean 18.8 ± 9.5 months; range, 6-44 months).
Patients’ Baseline Demographics and Medical Characteristics (79 Eyes).
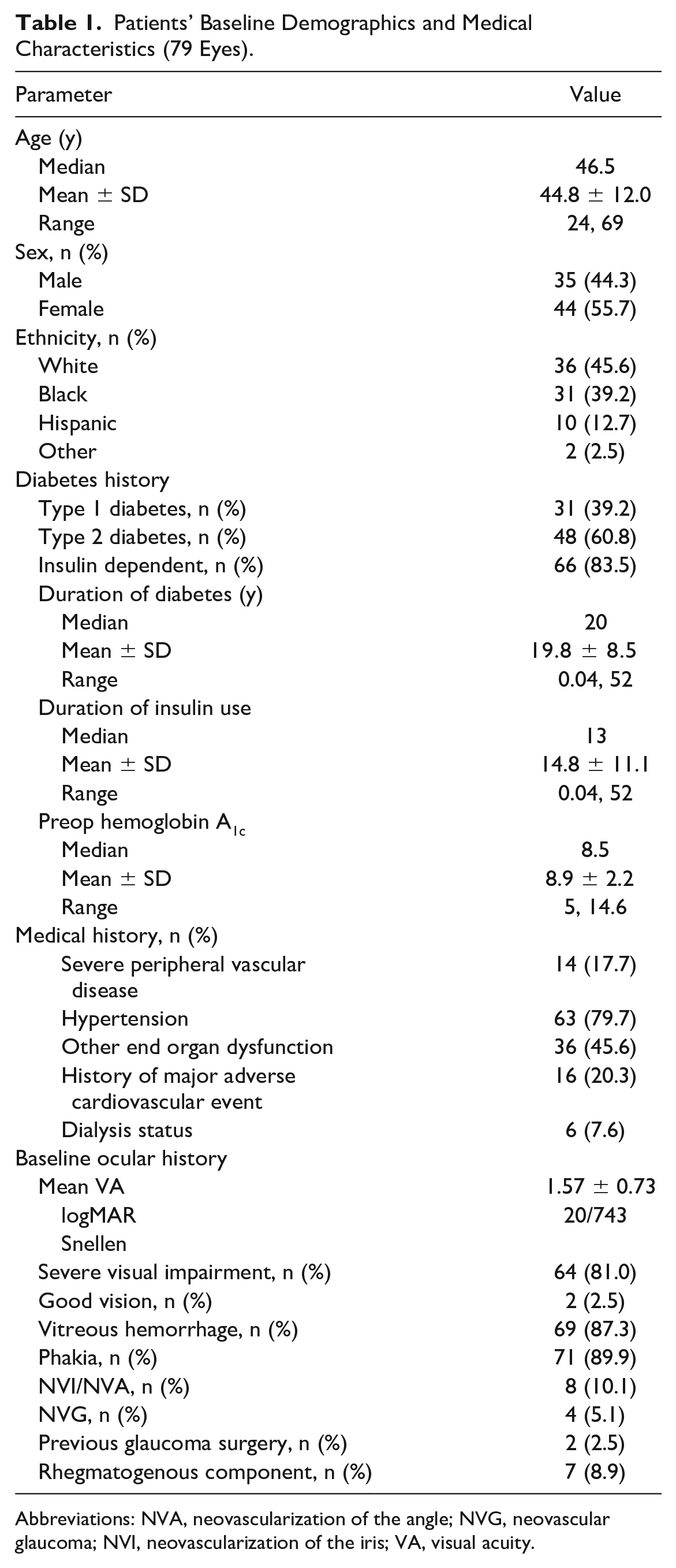
Abbreviations: NVA, neovascularization of the angle; NVG, neovascular glaucoma; NVI, neovascularization of the iris; VA, visual acuity.
Table 1 shows the baseline diabetic severity, medical history, and ocular history. Insulin dependence was reported in 66 patients (84%) for a median duration of 13 years before surgery. Hypertension was reported in 62 patients (80%), while severe peripheral vascular disease requiring amputation was found in 14 patients (18%). Six patients (8%) were undergoing regular hemodialysis at the time of surgical repair.
Before surgery, 64 patients (81%) had severe vision impairment (20/200 or worse; logMAR > 1.00) with an overall mean preoperative logMAR VA of 1.6 ± 0.7. Sixty-nine eyes (87%) had evidence of vitreous hemorrhage on preoperative examination. The majority of eyes included in the study were phakic (90%), with evidence of iris or angle neovascularization in 8 cases (10%). Four eyes (5%) had documented evidence of neovascular glaucoma before surgery.
Regarding the severity of the baseline diabetic TRD, vitreoretinal traction alone (grade A) was found in only 14 cases (17%). Detachment with extramacular involvement (grade B) was found in 27 eyes (34%). Detachment with macular involvement (grade C) was found in 23 eyes (29%). Detachment involving the posterior pole and extending beyond the equator (grade D) was found in 15 eyes (19%) (Figure 1). Although not considered in staging, 7 TRDs (8%) included a rhegmatogenous component.
Operative Outcomes
The median case length was 94 minutes (mean 102 ± 32.6 minutes; range, 50-232 minutes). Multi-gauge vitrectomy (27-gauge with single 23-gauge cannula) was planned in 5 cases (6%) for SO infusion. Other tamponade agents included filtered air (27 [34%]), SF6 (12 [15%]), and C3F8 (35 [44%]). Perfluoro-N-octane was used in 3 cases (3.8%). Intraoperative scissors were used in 1 case (1.3%). An intraoperative forceps was used in 12 cases (15%). Retinotomy was performed in 14 cases (17%).
The rate of overall macular reattachment throughout the entire study period was 89.9% (n = 71). All 8 cases of redetachment were identified by postoperative month 6; 3 of the cases were associated with significant baseline traction that could not be safely addressed with the initial surgery, and 5 cases resulted from new retinal contracture vs proliferative vitreoretinopathy. Four of 8 cases with subsequent detachment required a retinotomy. In the 71 patients with attached retinas at 6 months, persistent pockets of submacular fluid were identified in 15 cases (21.1%). The fluid ultimately resolved in 6 eyes by 1 year and 7 eyes by the final visit.
Table 2 shows the VA outcomes. Overall, the mean logMAR VA improved from 1.57 ± 0.72 (20/743) at baseline to 1.22 ± 0.93 (20/331) 6 months postoperatively (P < .001) and 1.08 ± 0.91 (20/240) at the final visit (P < .001). The proportion of eyes with severe visual impairment decreased from 81.0% (n = 64) preoperatively to 56.9% (n = 37) at 6 months (P < .001) and 49.3% (n = 39) at the final visit (P = .006) (Figure 2). The percentage of eyes with good vision increased from 2.5% (n = 2) at baseline to 10.8% (n = 7) 6 months postoperatively (P = .780) and 15.2% (n = 12) at the final visit (P < .001) (Figure 2). Likewise, 53.8% (n = 35) of cases had 3 or more lines of improvement in Snellen VA by month 6, which increased to 58.2% (n = 46) at the final visit. Only 65 of the 79 eyes had available 6-month postoperative data and were included in the calculation of the frequencies at that timepoint.
Overall VA Postoperative Outcomes Over Time.
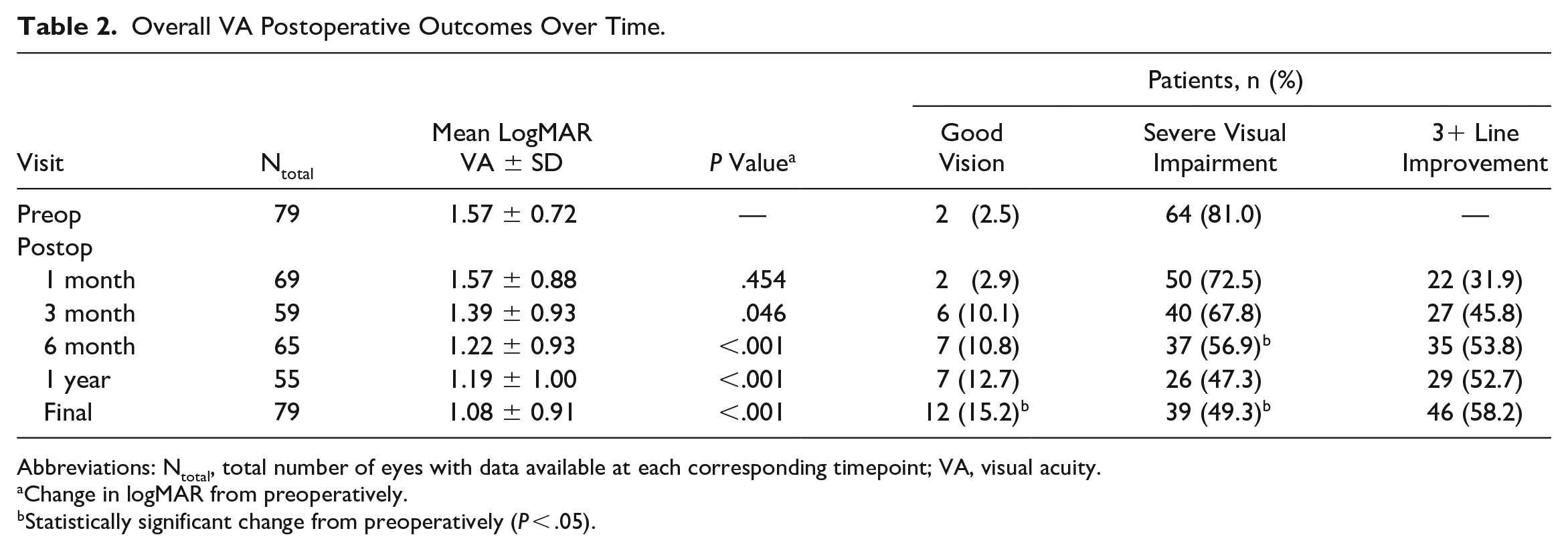
Abbreviations: Ntotal, total number of eyes with data available at each corresponding timepoint; VA, visual acuity.
Change in logMAR from preoperatively.
Statistically significant change from preoperatively (P < .05).
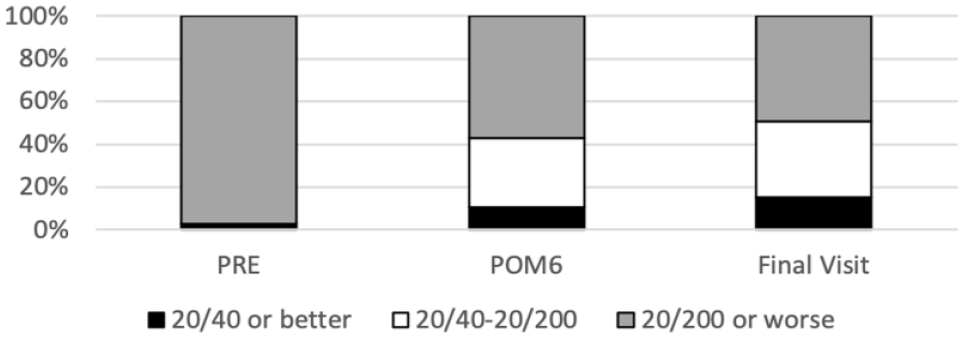
Overall postoperative change by visual acuity group.
None of the patients in our cohort developed endophthalmitis. Eleven patients (14%) had evidence of hyphema in the postoperative period. Postoperative CME developed in 9 patients (11.4%). Forty patients (50.6%) developed vitreous hemorrhage at some point in the postoperative period. The hemorrhage cleared spontaneously in 23 eyes (57.5%) within a mean of 6.08 ± 5.3 months. Reoperation was pursued to clear 13 of the 17 vitreous hemorrhages that did not clear.
Risk Factor Analysis
Table 3 shows the VA outcomes by difference predictors. Eyes with severe visual impairment at baseline had significantly worse VA at 6 months (P < .001). Insulin dependence was associated with a lower chance of severe visual impairment at 6 months (P = .045). Although there was no difference in the frequency of severe visual impairment at 6 months between eyes with and without baseline neovascularization of the iris (NVI) or angle (NVA) (P = .085), worse overall VA was observed 6 months postoperatively in eyes with NVI or NVA (Table 3). The mean reported duration of diabetes was shorter in patients with severe visual impairment at 6 months (17.5 ± 7.72 years) than in those with a VA better than 20/200 (22.6 ± 9.31 years) (P = .011). In addition, although not significant at 6 months, better preoperative VA (P < .01), absence of NVI/NVA (P < .01), and duration of diabetes greater than 15 years (P = .013) were associated with a higher frequency of achieving good vision at the final visit.
Six-Month Visual Outcomes by Different Predictor Variables.
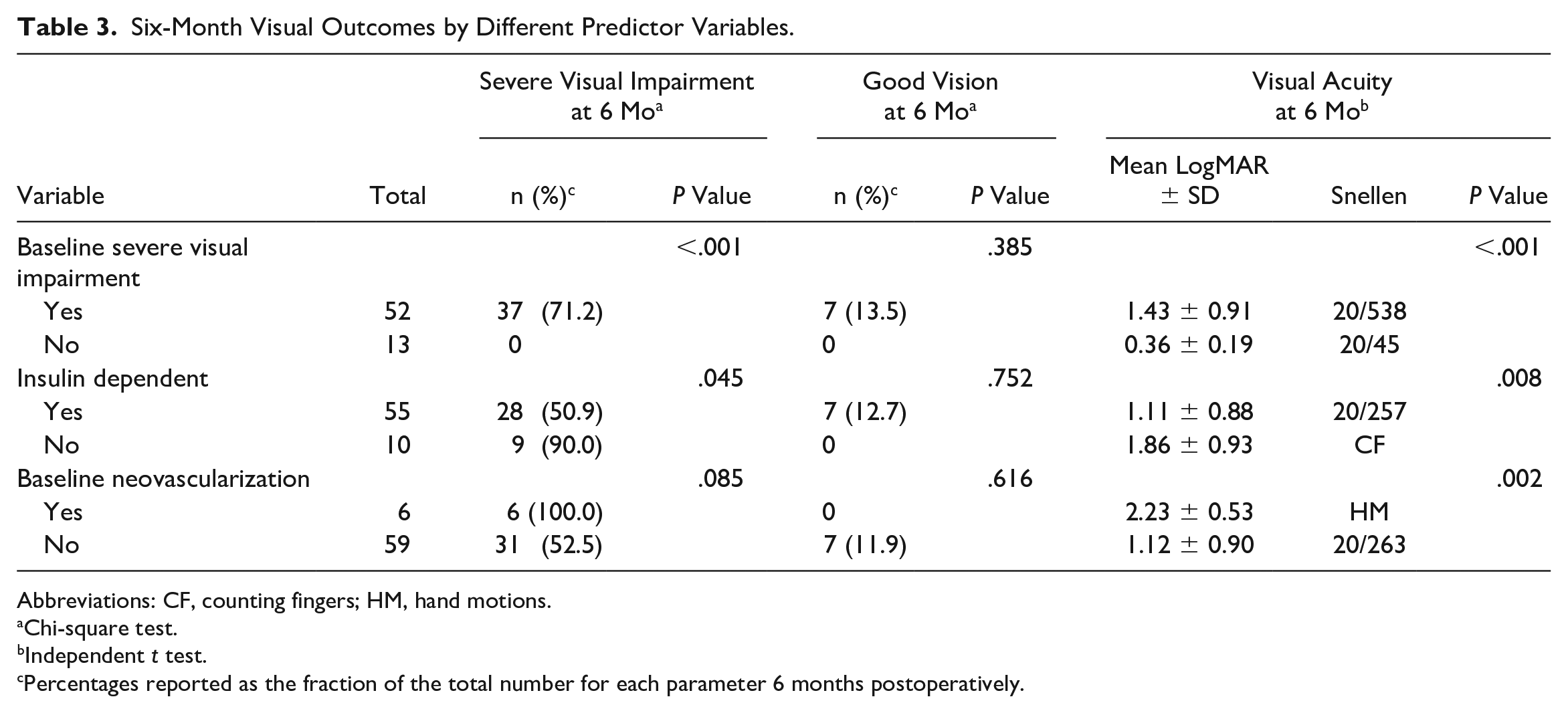
Abbreviations: CF, counting fingers; HM, hand motions.
Chi-square test.
Independent t test.
Percentages reported as the fraction of the total number for each parameter 6 months postoperatively.
Univariate linear regression analyses confirmed that preoperative logMAR VA (P < .001), insulin use (P = .017), duration of diabetes (P = .026), and baseline NVI/NVA (P = .004) were individual predictors for visual recovery at 6 months. There was a trend toward worse 6-month postoperative VA in patients on dialysis, although this did not reach statistical significance (P = .052). Of these variables, preoperative VA (P < .001) and insulin use (P = .045) were found to be significant coefficients for estimating 6-month postoperative VA when combined in a multivariate linear regression model (r = 0.691; P < .001). In both the univariate and multivariate regression models, no other medical or ocular history variable or baseline feature was found to be a significant predictor of visual recovery, including age, hypertension, previous stroke, preoperative vitreous hemorrhage, previous glaucoma surgery, or lens status (P > .05).
All 8 cases of macular redetachment occurred in patients with a preoperative VA of 20/200 or worse, and a binary logistic regression model confirmed that worse VA was significantly associated with a higher rate of redetachment (P = .017). Other preoperative factors, including the patient medical and ocular parameters listed in Table 1, were not found to be associated with an increased risk for redetachment (P > .05).
No preoperative variables were identified as significant risk factors for developing postoperative complications such as CME or hyphema (P > . 05).
Detachment Grading Analysis
Significant differences in logMAR VA between the RD severity groups were noted 6 months postoperatively (P = .015) but not at the final visit (P = .212). Tukey post hoc testing showed the greatest difference in VA between grade D and grade C at 6 months (P = .009). A higher proportion of eyes with grade D detachments had severe visual impairment at 6 months (P = .048) and the final visit (P = .003) compared with eyes with grades A, B, and C detachments combined (Figure 3). No differences were observed between the detachment grades with respect to the frequency of eyes achieving 20/40 or better VA at 6 months (P = .513) or at the final visit (P = .272). No differences in postoperative visual recovery were observed between grades A, B, and C at any timepoint (Figure 3).
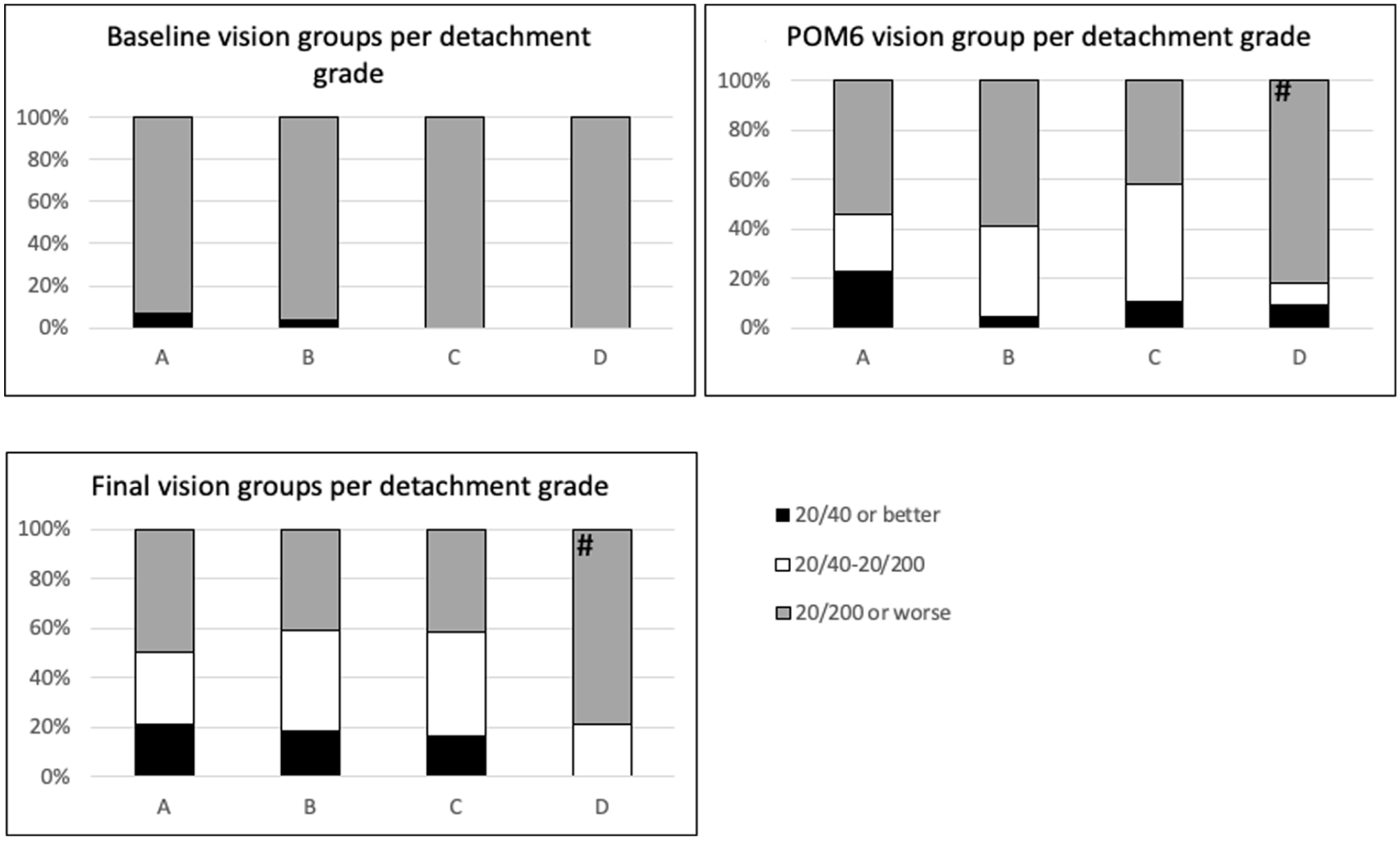
Postoperative visual acuity changes by baseline detachment grade.
Detachment severity grading was not associated with a higher frequency of redetachment or complications, such as vitreous hemorrhage (P = .52) or CME (P = .36). Similarly, none of the preoperative variables in Table 1, such as duration of diabetes, preoperative HbA1c, insulin use, or previous glaucoma surgery, were correlated with detachment grade (P > .05).
Conclusions
In this retrospective study, successful completion of diabetic TRD surgery was accomplished in all 79 eyes with 27-gauge PPV. SO infusion was required in only about 6% of cases. By the final visit, 58% of patients had an improvement in VA of at least 3 lines. There was nearly a 40% reduction in cases of severe vision loss and nearly a 4.5-fold increase in the frequency of eyes achieving 20/40 VA. Worse preoperative VA was associated with a higher risk for redetachment and worse vision at 6 months. Of the patient history parameters assessed, insulin dependence, duration of diabetes, and NVI/NVA were significant predictors of visual outcomes after diabetic TRD repair. Preoperative evidence of posterior pole detachments extending beyond the equator portended a poor visual prognosis. Surprisingly, there were no differences in outcomes between eyes with vitreoretinal traction alone, eyes with extramacular detachment, and eyes with macular detachment.
Diabetic TRD remains a major source of vision loss in diabetic patients and can be associated with other complications of severe diabetic retinopathy (DR), such as vitreous hemorrhage and macular edema. 19 In PPV, removal of the vitreous and delamination of membranes allows relaxation of the retina and prevents further tractional membrane formation into the vitreous scaffold.1,4 Although 23-gauge and 25-gauge repair have remained popular for diabetic TRD repair because of the improved surgical time, comfort, and recovery compared with its 20-gauge predecessor,1,6–8 the newer 27-gauge vitrectomy system introduced in 2010 may provide additional advantages, including easier and safer access between planes in complex detachment repair and potentially less risk for iatrogenic breaks resulting from the smaller field of influence.1,9
To our knowledge, our study is the largest retrospective analysis of 27-gauge PPV for diabetic TRD repair. The ultimate reattachment rate was 89.9%, which is in line with published outcomes with larger gauge instrumentation. Although the small number of redetachments in our cohort limited the ability to perform statistical analyses, the presence of previous retinotomy in nearly 50% of redetachments points to the baseline severity of TRD and the known association between retinal breaks and redetachment in TRD surgery as important factors in redetachment in this population.
Storey et al 8 observed a primary reattachment rate of 87.6% in a 2018 study of 403 eyes with diabetic traction and traction RRD that had PPV with a 20-gauge, 23-gauge, or 25-gauge system. Sokol et al 20 performed a retrospective analysis of 69 eyes that had diabetic TRD repair with 23-gauge PPV; the primary reattachment rate was 98.6% (n = 68). Chen et al 15 compared 27-gauge and 25-gauge repair of diabetic TRD in a retrospective case series. They reported a primary reattachment rate of 90.9% (20/22) for 25-gauge PPV and 100% (0/21) for 27-gauge PPV. Although there are some reservations about the ability to successfully perform tractional detachment repair with a smaller gauge approach, our findings suggest that the outcomes with 27-gauge PPV are comparable to those achieved with larger gauges and are likely more affected by the TRD severity than the choice of instrumentation.
Although visual improvement after diabetic TRD repair can be limited, more one half of all patients in our study had 3 or more lines of VA improvement and there was roughly a 40% decrease in the number of patients with severe VA (20/200 or worse) by the final visit. By comparison, Storey et al 8 saw 2 or more lines of improvement in 56.3% of eyes that that had PPV with a 20-gauge, 23-gauge, or 25-gauge PPV for diabetic TRD. Choovuthayakorn et al 21 reported that 44% of eyes had 2 or more lines of improvement after 20-gauge and 23-gauge repair, and Sokol et al 20 saw a 53.6% decrease in patients with severe visual impairment with 23-gauge PPV. Although not typically evaluated in the literature, there was a roughly 13% increase in patients with 20/40 or better VA by the end of our study, which is similar to the 21.8% increase in patients with 20/50 VA or better observed by Sokol et al. 20 As vitrectomy technology and outcomes continue to develop, the frequency of good VA may become a more studied endpoint for diabetic TRD repair with PPV.
Our findings of preoperative VA and NVI as negative visual prognostic factors for 27-gauge PPV are in line with the literature examining ocular factors associated with poor outcomes after 23-gauge and 25-gauge repair of diabetic TRD.1,22,23 Williams et al 22 found that a preoperative VA of 5/200 (logMAR 1.6) or better was the strongest predictor of improved VA. In a retrospective case series of 360 eyes by Thompson et al, 23 NVI was associated with an increased likelihood of a final postoperative VA of less than 5/200. Previously suggested prognostic risk factors from the literature that were not found in this study included age and significant preoperative vitreous hemorrhage.1,22,23 Our observation that insulin dependence and a longer reported duration of diabetes were associated with better visual outcomes are new findings, and we hypothesize this may indicate that patients with better diabetes control could have an opportunity for better visual recovery.
In addition to describing outcomes and identifying patient prognostic factors for surgical outcomes, this study sought to evaluate a preoperative grading system for diabetic TRD because there is no consensus on an optimal preoperative classification for DR or TRDs in the literature. 24 Although many classification systems for DR have been suggested, most do not sufficiently distinguish the degrees of severity in diabetic TRD and none was created as the clinical tool for estimating the surgical prognosis.
The early Airlie House classification was designed in the 1960s to assess photocoagulation outcomes and categorized DR only into proliferative versus nonproliferative types.24,25 In the 1980s the modified Airlie House system classified DR as “mild,” “moderate,” or “high risk,” while diabetic eyes with evidence of vitreoretinal traction or detachment were classified separately as “advanced.” 26 In 2003, the International Clinical Retinopathy Diabetic Severity Scale expanded on the modified Airlie House classification, adding “no retinopathy” and “PDR” (proliferative diabetic retinopathy) categories. 27
To our knowledge, the Kroll classification is the only proposed model to distinguish different types of diabetic TRD. In this system, stage A represented eyes with proliferative changes but no detachment, PDVR stage B represented eyes with vitreoretinal traction and shallow circumscribed extramacular detachments, and PDVR stage C indicated macular detachment involvement. 28 The Kroll classification has been shown to estimate the visual prognosis after surgical repair according to a previous analysis of 563 eyes that found that a postoperative VA improvement of 3 lines or more was more frequent in Kroll stage A (only proliferative changes) than in Kroll stage B and stage C (any evidence of detachment). 29
In our study, we focused only on eyes with the presence of significant vitreoretinal traction and detachment and further refined the Kroll stages B and C based on macular involvement and the extent of detachment. Our goal was to provide a grading scheme that can be used clinically to estimate the surgical prognosis. We did not use subdivisions and notations for each stage, as in the Kroll classification, which was designed to describe the pathogenesis and progression of PDR. 28
Our finding that visual recovery was worse in grade D cases (posterior pole detachment extending beyond the equator) than in cases with grade A, B, or C (vitreoretinal traction alone, extramacular detachment, macular detachment, respectively) appears to justify this additional severity category and its relevant distinction from diabetic eyes with milder degrees of macular involvement. Although we did not observe a stepwise decline in surgical outcomes in eyes with grade A, B, or C, we found similar anatomic and visual recovery in eyes in these groups, even with respect to achieving 20/40 postoperative VA or better.
Notably, there was no association between the grade of and risk for detachment, suggesting that visual impairment could be related to the chronicity of foveal detachment. This may imply that 27-gauge PPV is effective in repairing TRDs with macular involvement, extramacular involvement, or extensive traction alone with comparable outcomes. Furthermore, in our study macular involvement not extending beyond the equator did not appear to be a visual or anatomic prognostic risk factor after diabetic TRD repair with 27-gauge PPV and may indicate a less chronic disease. Future high-powered research is needed to better characterize this effect. Future studies might also consider comparing visual outcomes between grades A and B (no macular detachment) and grades D and C (macular detachment) given that preoperative macular status is a recognized predictor of outcomes in rhegmatogenous detachments.
This study was limited by its retrospective nature, variable follow-up time, and small sample. Only 79 patients of the original 110 patients identified as having primary diabetic TRD repair via 27-gauge PPV met the inclusion criterion of greater than 6 months of follow-up data. This was representative of the overall poor follow-up described in patients with diabetes 30 and was likely exacerbated by the COVID-19 pandemic. Thus, our study might not be adequately powered to draw specific conclusions about the population at large.
In addition, this study did not control for operative variables that can contribute to a poor final VA at 6 months, including the use of SO or retinotomy, given the overall low prevalence of these cases in the surgical cohort. Further follow-up may better characterize the prognostic factors identified in this study and expand the utility of the detachment severity classifications. Future higher powered work may also take into consideration other detachment parameters that could affect visual recovery, such as preoperative vitreous hemorrhage or rhegmatogenous components, to refine and propose a comprehensive grading system for diabetic TRD.
In conclusion, to our knowledge this is the largest analysis of 27-gauge PPV for diabetic TRD repair to date and supports the efficacy of this approach for diabetic TRD of varying severities. The primary reattachment rate was 89.9%, with SO being required in only 6% of cases. There was significant VA improvement, with a roughly 40% reduction in the number of eyes with severe visual impairment and 12% increase in eyes with good vision by the end of the study. Preoperative VA, insulin use, the duration of diabetes, the presence of NVI, and baseline posterior pole detachment extending beyond the equator may affect visual recovery.
Footnotes
Ethical Approval
Ethical approval of this reserach was granted via the University of Virginia Institutional Review Board and adhered to the tenets of the Declaration of Helsinki. Data collection was conducted in accordance with regulations set forth by the US Health Insurance Portability and Accountability Act.
Statement of Informed Consent
As this was a retrospective study with de-identified data, informed consent was deemend not necessary by the University of Virginia Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.