
Abstract
Keywords
Introduction
Rhegmatogenous retinal detachments (RRDs) are a common indication for vitreoretinal surgery. An RRD is considered complex when it is associated with proliferative vitreoretinopathy, a giant retinal tear, or ocular trauma or has a component of fibrosis, such as in combined RDs (static traction causing retinal break). 1 Such cases have a higher incidence of surgical failures of primary surgery despite complex maneuvers. 2
A key component of vitreoretinal surgery for RRD is the use of tamponade agents to keep the retina attached after surgery. This allows laser retinopexy and cryopexy to transform into strong chorioretinal adhesions around the retinal breaks.3–5 Conventionally used tamponade agents include silicone oil and gases.4,6 These necessitate relatively uncomfortable postoperative positioning and are not suitable in conditions such as aphakia, aniridia, a compromised cornea, and advanced glaucoma.6–9
Our group previously explored the tissue-adhesive properties of fibrin glue as an alternative to conventional tamponade in cases of simple, primary, fresh RRDs (GUARD [Glue-Assisted Retinopexy in Retinal Detachments] Study). 10 The use of fibrin glue in vitreoretinal surgery for simple RRD has also been reported by others and has been described in macular surgical procedures other than surgery for RRD.10–14
In the cases series presented here, application of fibrin glue as a surgical adjunct was successful in the management of complex RRDs. The isolated use of a conventional tamponade agent was not feasible in these cases because of the variable nature of the complex RRD or the anatomy of the eye.
Methods
In this a retrospective case series, informed consent for the procedure was obtained from all patients and approval was obtained from the institute ethics committee (ref no. LEC-BHR-R-06-23-1061). All patients were treated at a tertiary eye hospital in South India by the same surgeon (B.T.). Surgery was performed using a single pars plana vitrectomy (PPV) system that used pressurized infusion and built-in intraocular pressure (IOP) compensation (Constellation Vision System, Alcon).
Glue was applied according to the GUARD technique as previously described. 10 Briefly, fibrin glue was applied to seal retinal breaks after fluid–air exchange and laser retinopexy. The retinal surface was dried completely before fibrin glue (Tisseel, Baxter AG) was injected using a 1 mL syringe capped with a flute needle (a thick component followed by a thin component to avoid glue migration), and the fibrin glue coagulum was used to cover the breaks. In 4 of the 5 cases, the decision to apply glue was made before the surgery; in the other case, application of glue was necessary because of a surgical complication.
Results
Anatomic success was attained in all 5 cases (in 3 cases without a tamponade agent and in 2 with silicone oil). Epiretinal membranes formed in 2 cases and transient vitritis in another 2 cases, with increased IOP occurring in 1 of them. Table 1 shows the case details and reasons for glue application. The fibrin coagulum dissolved in all cases within 2 weeks.
Clinical Details, Reasons for Fibrin Glue Application, and Outcomes of Cases.
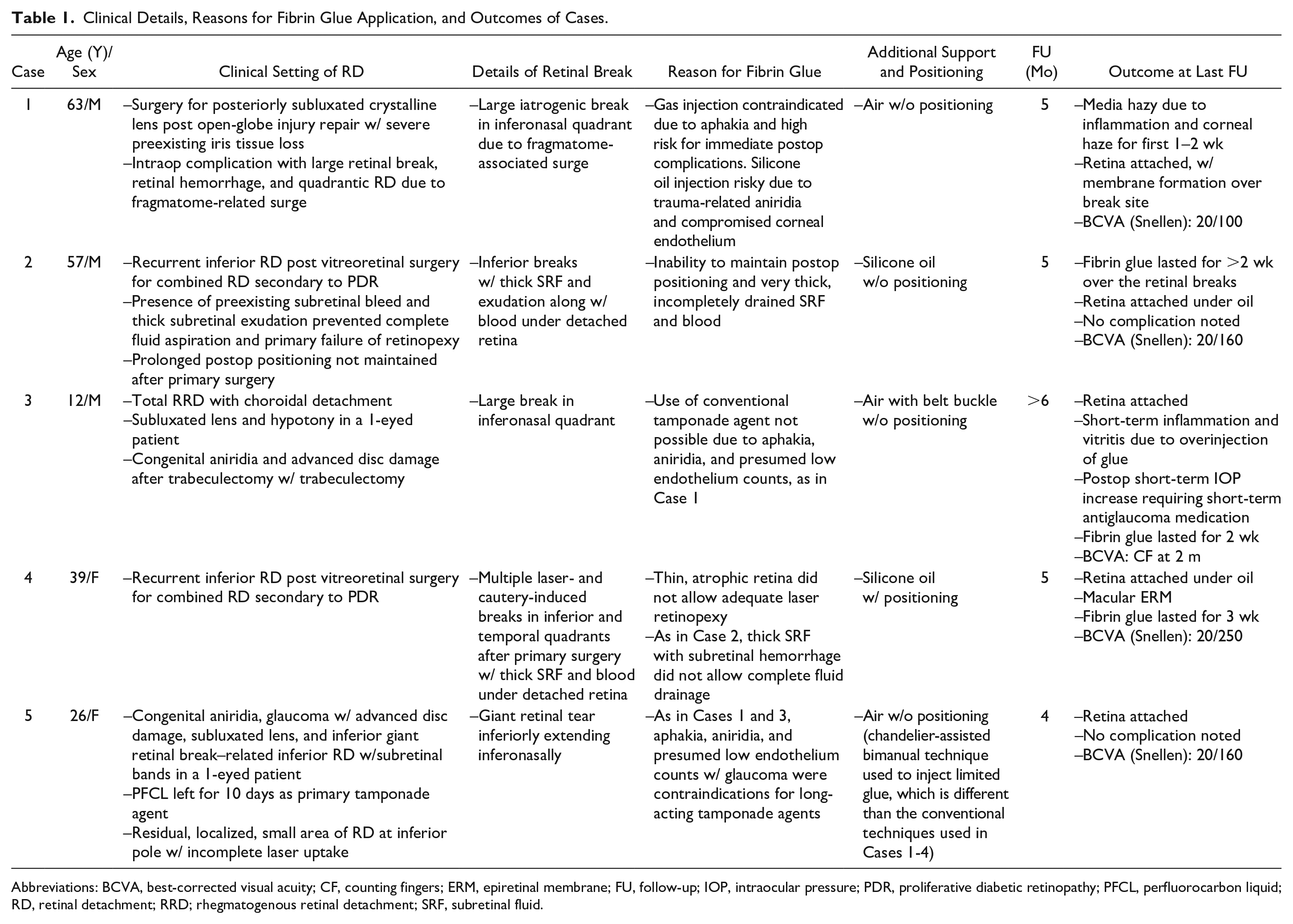
Abbreviations: BCVA, best-corrected visual acuity; CF, counting fingers; ERM, epiretinal membrane; FU, follow-up; IOP, intraocular pressure; PDR, proliferative diabetic retinopathy; PFCL, perfluorocarbon liquid; RD, retinal detachment; RRD; rhegmatogenous retinal detachment; SRF, subretinal fluid.
Case 1
A 63-year-old man had pars plana lensectomy (PPL) and PPV for a primary corneoscleral tear repair. The eye had severe iris tissue loss with a corneal scar at the time of presentation. Vitreous hemorrhage and posterior dislocation of the crystalline lens were confirmed preoperatively on B-scan ultrasonography (Figure 1A).
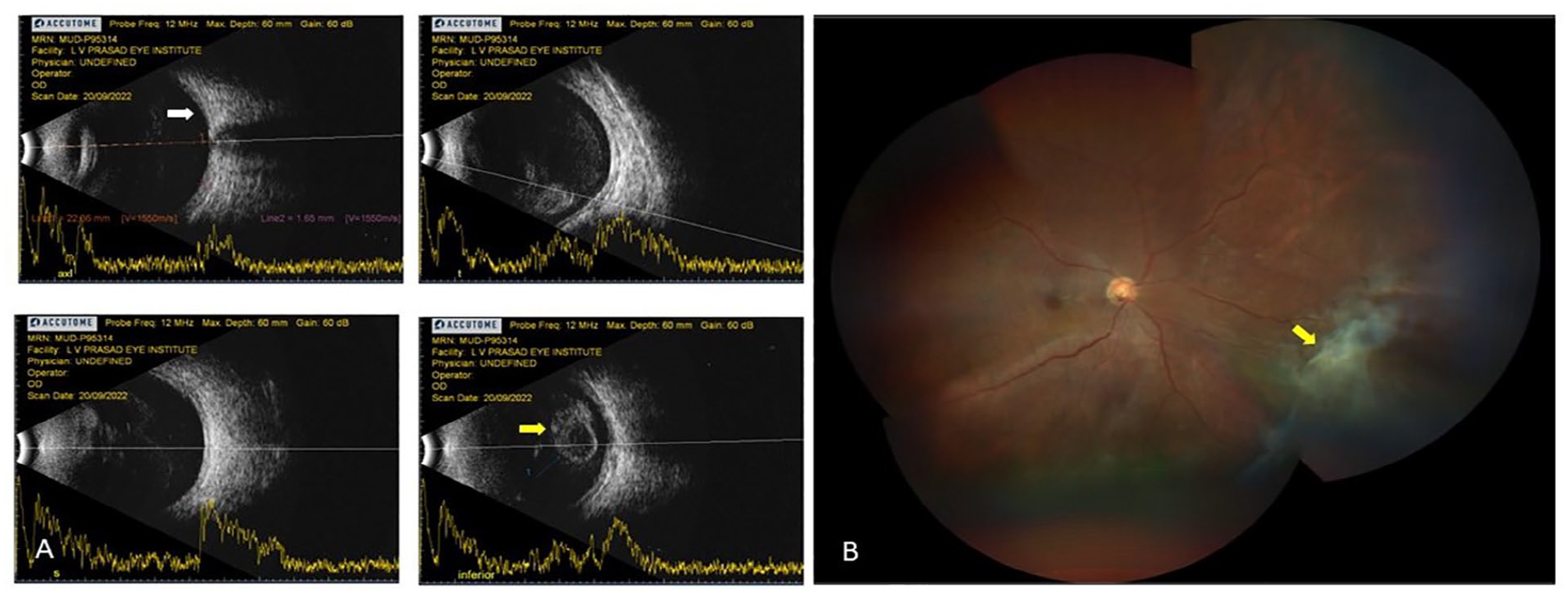
Images from Case 1. (A) Preoperative B-scan shows vitreous hemorrhage with a posteriorly dislocated crystalline lens (arrow in lower-right image) and an attached retina (arrow in upper-left image). (B) Fundus photograph 6 weeks after surgery with fibrin glue shows an attached retina with membranes surrounding the break nasally (arrow).
During surgery, a large iatrogenic break occurred secondary to a surge during phacofragmentation, resulting in a localized RD in the nasal quadrant and a retinal hemorrhage. After the bleeding was controlled and fragmentation completed, fluid–air exchange was done through the retinal break. Laser retinopexy was performed, and fibrin glue was used to cover the retinal break. This was done because injecting gas or silicone oil injection would likely lead to complications from glaucoma; silicone oil would also have caused corneal endothelial loss because of the aphakia and aniridia.
Successful reattachment was noted at all visits after a transient period of inflammation (Figure 1B). At the last follow-up visit 5 months after surgery, the retina was attached and the patient had a best-corrected visual acuity (BCVA) of 20/100. Retinal membranes were noted over the break during the first month after surgery but remained stable.
Case 2
Fibrin glue was used to manage a recurrent RRD in a case of combined RD secondary to proliferative diabetic retinopathy (PDR). A 57-year-old man had PPV with membrane peeling, endolaser application, and silicone oil injection as the primary surgery. During surgery, the presence of thick subretinal fluid (SRF) mixed with exudation and blood prevented adequate laser retinopexy.
The patient had persistent SRF 2 weeks after surgery with open breaks (Figure 2, A and B). Fluid–air exchange when possible, endolaser application around the break, fibrin glue application over the break, and silicone oil exchange were performed (Figure 2, C and D). Fibrin glue was used because the patient could not comply with postoperative positioning because of dyspnoea and because the thick SRF could not be drained well. The retina was attached at the last follow-up visit 4 months postoperatively, and the patient had a BCVA of 20/160 with isolated pockets of SRF.
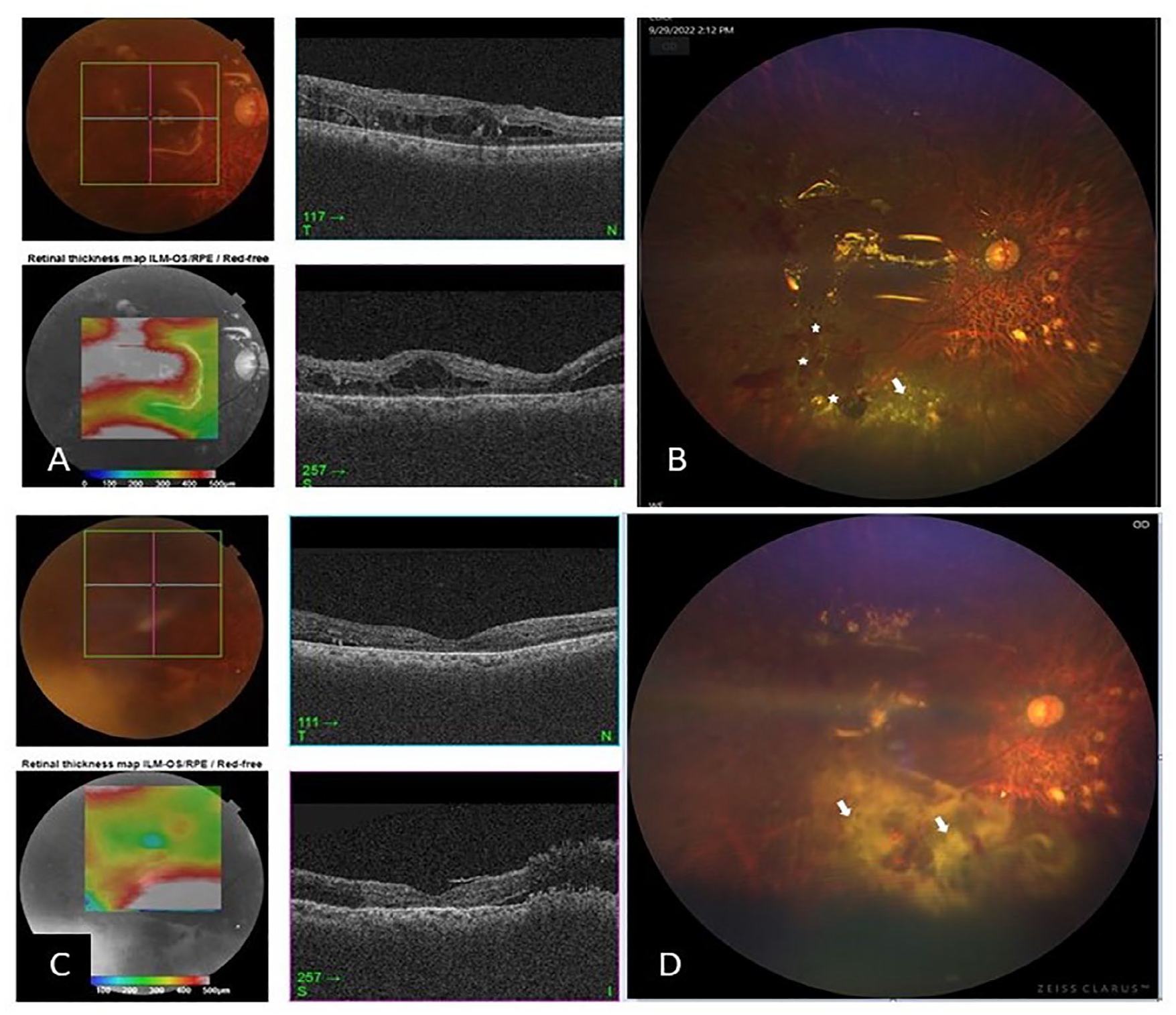
Images from Case 2. (A) SS-OCT and (B) fundus photograph 3 weeks after primary surgery shows a recurrent retinal detachment. Open breaks (stars) and subretinal exudation (arrow) are noticeable. (C) SS-OCT and (D) fundus photograph 2 weeks after repeat surgery with fibrin glue application (white arrows) shows an attached retina.
Case 3
Fibrin glue was used along with a belt buckle, PPV, endolaser application, external drainage, and air tamponade to manage RRD with choroidal detachment (Figure 3A) in a 1-eyed, 12-year-old boy with aniridia, a subluxated lens, a poor corneal surface from limbal stem cell deficiency, and advanced glaucomatous disc damage. The boy previously had trabeculotomy with trabeculectomy and presented with hypotony and a poor fundus view. After explant placement, PPL, PPV, and external fluid drainage, fibrin glue was used to avoid the conventional tamponade-associated risk to the already compromised cornea and optic nerve and to eliminate the need for postoperative positioning (Figure 3B).
Images from Case 3. (A) Preoperative B-scan shows the presence of a retinal detachment (arrows). (B) Fundus photograph 1 week after surgery shows fibrin glue application (arrows) and the high indent of the explant. The optic disc has glaucomatous atrophy. (C) Fundus photograph 1 month after surgery with fibrin glue shows an attached retina with glaucomatous optic atrophy.
At the last follow-up visit 4 months postoperatively, the retina was attached. The patient had a BCVA of counting fingers at 2 m, and the IOP was well controlled with medication (Figure 3C). The patient had developed short-term vitritis and elevated IOP in relation to excess injection of glue.
Case 4
Fibrin glue was used to manage a recurrent combined RD in a 39-year-old woman with PDR. The patient had PPV with membrane peeling, endolaser application, and silicone oil injection as the primary surgery. However, after 10 days the patient had recurrence of the inferior RD and laser-induced breaks in the inferior and temporal retina, which was very thin and atrophic (Figure 4A). The recurrent detachment had thick SRF and subretinal blood. Silicone oil exchange was performed. Fibrin glue was applied over the breaks, as in Case 2, to physically seal the breaks in the thin, atrophic retina that would otherwise limit retinopexy and internal fluid drainage (Figure 4B). At the last follow-up visit 5 months postoperatively, the retina was attached with the formation of macular membranes (Figure 4C) and the patient had a BCVA of 20/250.
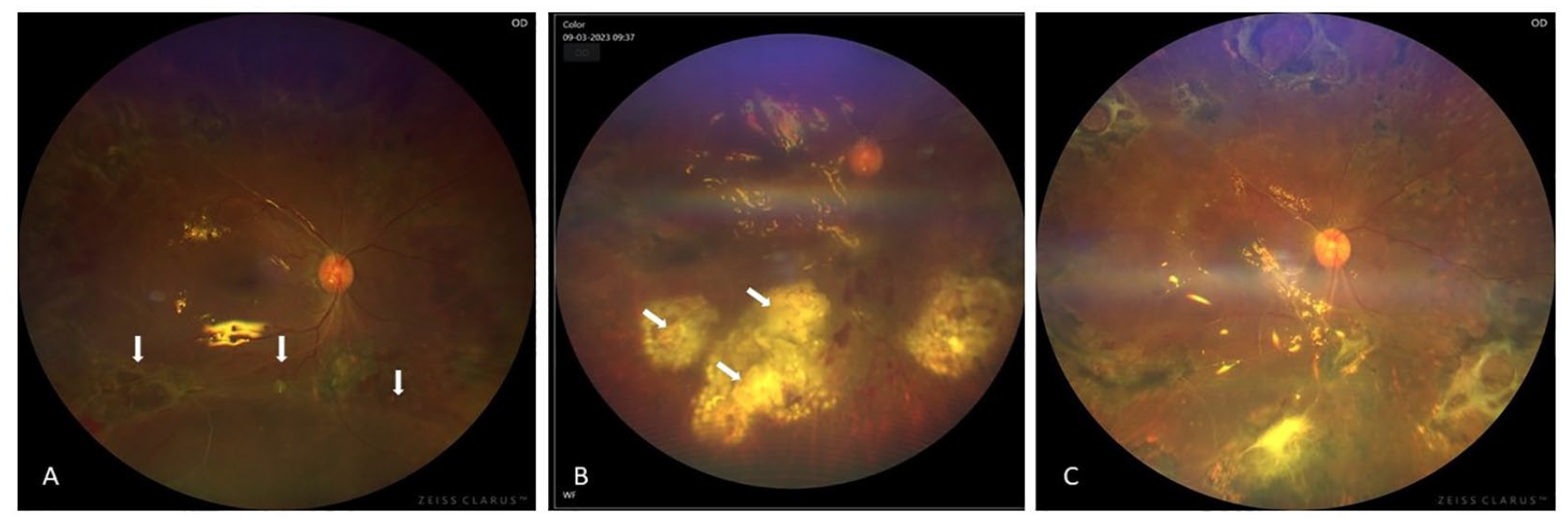
Images from Case 4. (A) Fundus photograph shows a detached inferior retina under silicone oil (arrows). (B) Fundus photograph 1 week after a second surgery with fibrin glue application (arrows). (C) Fundus photograph at 5 months shows absorbed fibrin glue from the sites below the arcade, an attached retina, and membrane formation at the macula.
Case 5
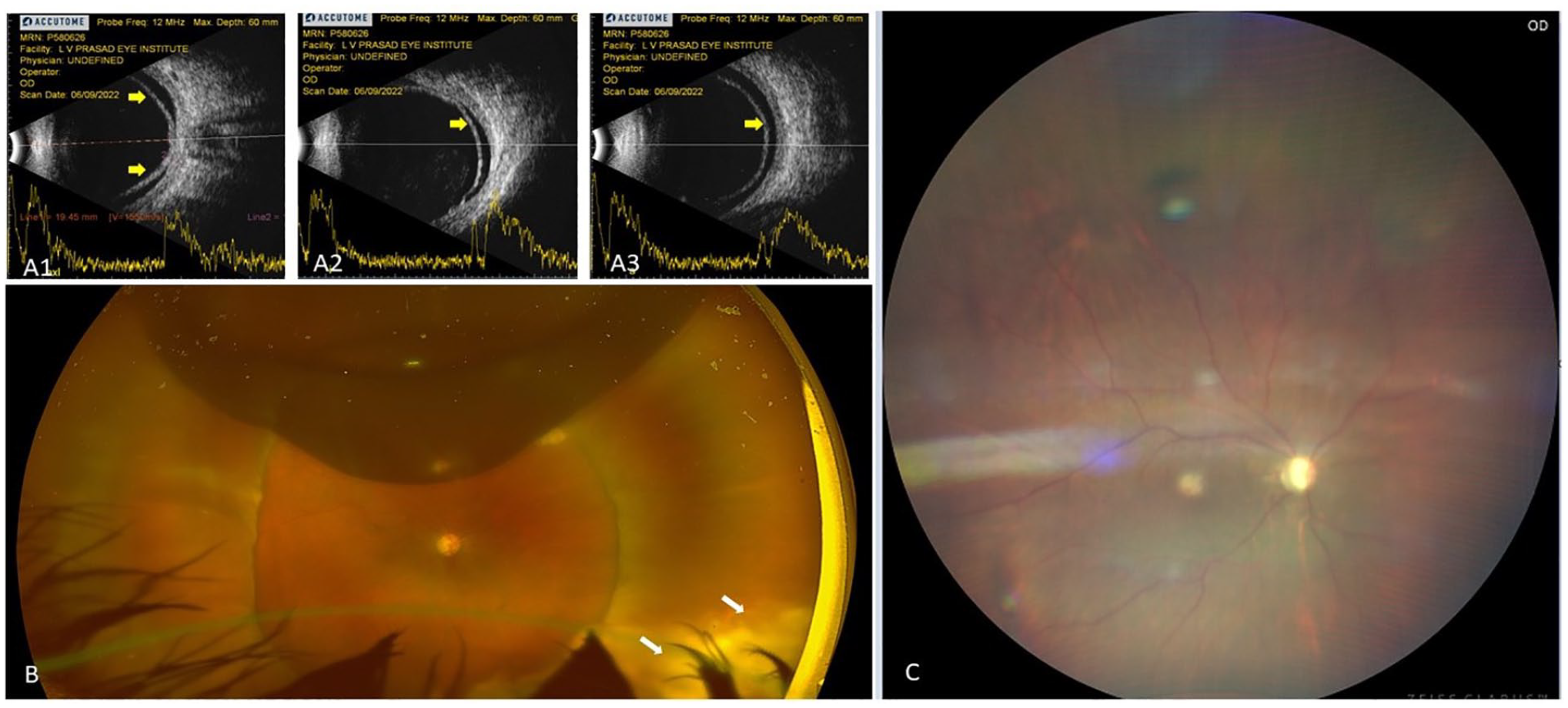
Fibrin glue was used to manage a case of lens subluxation with vitreous hemorrhage and RRD resulting from an inferior giant retinal tear in a 26-year-old 1-eyed woman with congenital aniridia, limbal stem cell deficiency, and advanced glaucomatous disc damage (Figure 5, A and B). The patient previously had Ahmed glaucoma valve implantation in both eyes to control the IOP.
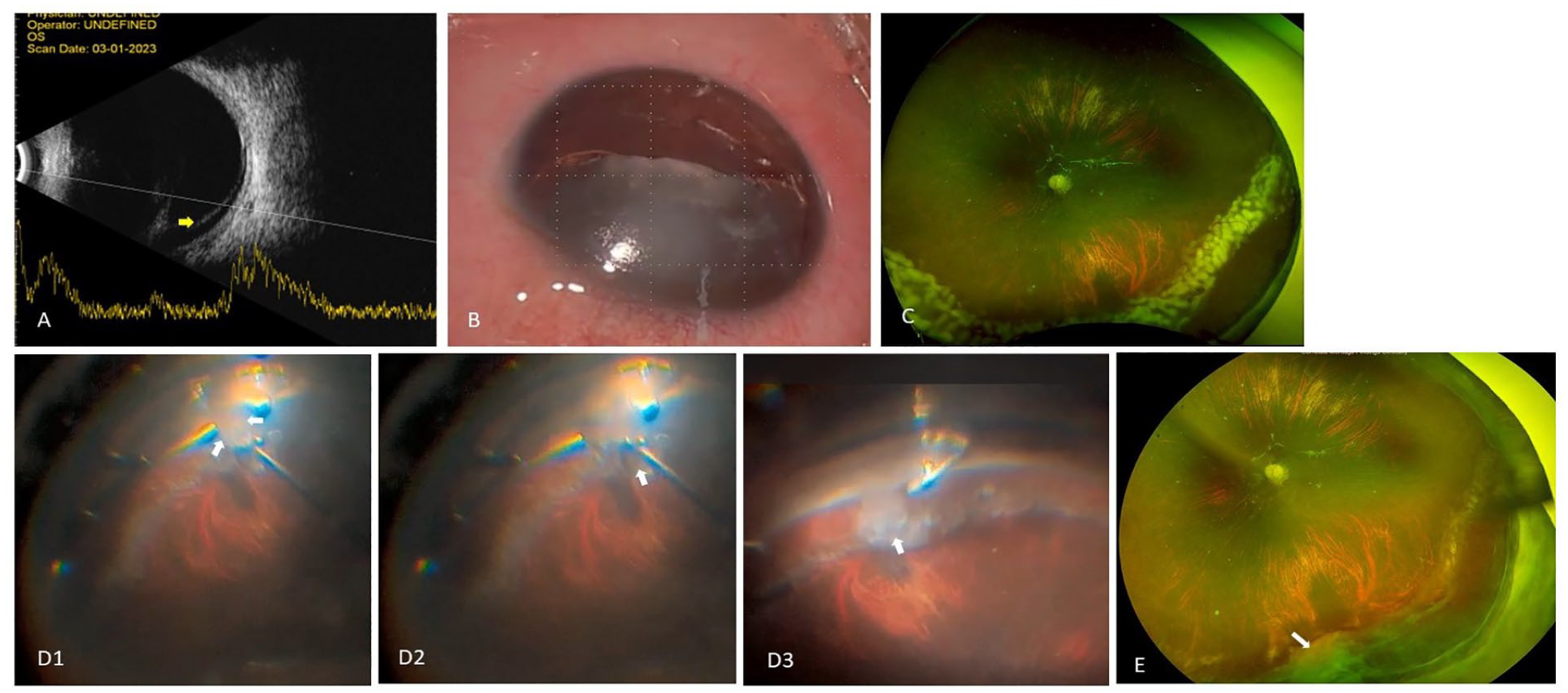
Images from Case 5. (A) Preoperative B-scan shows the presence of a retinal detachment (arrow). (B) Intraoperative photograph shows aniridia and a subluxated crystalline lens. (C) Fundus photograph 1 week later shows an attached retina under perfluorocarbon liquid with fresh laser marks. (D) Intraoperative photographs show the application of fibrin glue over the break using a chandelier-assisted bimanual technique (arrow). D1 shows the first injection of the thick component (arrow). D2 shows the immediate injection of the thin component over the thick component (arrow). D3 shows the formation of localized and controlled coagulum over the break within 1 minute (arrow). (E) Fundus photograph 2 weeks later shows an attached retina with glue coagulum at the break site (arrow).
The patient had PPL with PPV. During surgery, a preexisting giant retinal break was noted inferiorly with an inferior RD and subretinal bands. In the first surgery, fluid–air exchange was performed, dense laser treatment was applied, and the eye was left under perfluorocarbon liquid (PFCL) in view of the nature of RRD (Figure 5C). At 10 days, a localized small RD was noted inferiorly around the previous laser marks where laser uptake was poor. The PFCL was removed as planned, the RD was drained through a retinotomy, fluid–air exchange and laser augmentation were performed, and limited fibrin glue was injected over the break. To avoid excessive glue injection, the chandelier-assisted bimanual technique was used. A single, thick, drop of glue followed by a thin component of glue were applied almost simultaneously using a bimanual approach to prevent migration of the glue (Figure 5D).
Fibrin glue was used as in Cases 1 and 3 to avoid the risk for secondary glaucoma and corneal damage from the conventional tamponade agents (Figure 5E). At the last follow-up visit 4 months postoperatively, the retina was attached without obvious complications and the patient had a BCVA of 20/125, although with a subjectively limited visual field.
Conclusions
These cases show the safety and efficacy of fibrin glue as an adjunct to conventional tamponade agents in cases of complex RRDs. Successful attachment of the retina was attained in all cases in our series.
Tamponade agents require relatively uncomfortable head positioning in the postoperative period. Silicone oil is associated with an increased risk for glaucoma, hastened cataractogenesis in phakic patients, and the need for a second surgery to remove the silicone oil.6–8 Sulfur hexafluoride and perfluoropropane, apart from the risk for raised eye pressure, temporarily preclude the patient from air travel. In addition, these tamponade agents can prolong the time to visual recovery.6,9 The use of fibrin glue can help avoid these drawbacks, hence its value in surgery for RRD.
Several studies have assessed the use of alternative tamponade agents, including fibrin glue, in the surgical management of RRD.15–18 The use of biologic tissue adhesives in vitreoretinal surgery was first described by Coleman et al 19 in animal eyes and human eyes. They used a commercially available combination of bovine thrombin and pooled human fibrinogen. This was injected into the subretinal space in rabbit eyes and porcine eyes to achieve chorioretinal adhesions. In human eyes, the role of glue was shown in cases of macular holes with RD; however, concurrent gas tamponade was also used in these cases. 19
More recently, our group described the successful use of fibrin glue in the surgical management of fresh RRDs, 10 as did Wang et al 11 and Aydin et al 12 in separate case series. Tyagi and Basu 10 and Wang et al 11 describe a technique in which no additional tamponade agents were used and the globe was filled with a balanced salt solution at the end of surgery.
Our present case series further expands the indications for the surgical use of fibrin glue from primary RRDs to complex RRDs, for which the use of conventional agents alone may not be sufficient or should be avoided because of the high risk for complications. None of our cases required strict postoperative patient positioning. We used glue in the present series as the sole agent for tamponade. The possible use of glue as an agent for retinopexy is an interesting concept but requires further research.
Previously, Koreen et al 20 studied 285 vitrectomized eyes without preexisting glaucoma and without a risk for secondary glaucoma over the long term. They found that the overall incidence of glaucoma development was higher in nonphakic eyes (15%) than in phakic eyes (1.4%) (P = .001). In addition, cataract extraction before or at the time of vitrectomy was not associated with glaucoma. In contrast, in 3 cases in our series (Cases 1, 3, and 5), fibrin glue was used to avoid conventional tamponade agents given that the patients were aphakic, were without iris tissue, or had preexisting glaucoma. Furthermore, Case 3 and Case 5 had advanced preexisting glaucoma and had previous surgery to treat it. Therefore, we chose to avoid conventional tamponade agents in these eyes.
To conclude, fibrin glue is an effective and safe surgical adjunct in cases of complex RRD. It can effectively seal the retinal break and help prevent ocular fluid from entering the site of the break when the use of a conventional tamponade agent is not possible or might not be sufficient if used alone. Larger studies with multiple surgeons are required to establish the efficacy of fibrin glue as a tamponade agent in management of RRD before its acceptance as an alternative or adjunctive tamponade in primary and complex RRDs.
Footnotes
Ethical Approval
Ethical approval was not required.
Statement of Informed Consent
The patients consented to publication of the clinical history, findings, and images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. Desai, Bhopalka, Tyagi, and Takkar received funding from Hyderabad Eye Research Foundation. Dr. Takkar received funding from DBT Wellcome Trust India Alliance Clinical Research Centre grant (IA/CRC/19/1/610010) awarded to IHOPE.