
Abstract
Keywords
Introduction
A new ophthalmic solution of pilocarpine hydrochloride 1.25% received widespread attention after it was granted US Food and Drug Administration (FDA) approval in October 2021 as the first pharmaceutical treatment for patients with presbyopia. 1 Pilocarpine, a parasympathomimetic agonist at the postganglionic muscarinic receptors, was previously regarded as a standard treatment used to lower intraocular pressure (IOP) in patients with glaucoma. 2 Although its use in glaucoma treatment has largely been replaced by other similarly efficacious medications with fewer side effects, pilocarpine was reintroduced for the treatment of presbyopia. In addition to aiding aqueous outflow through morphologic changes, pilocarpine causes accommodation and miosis through the contraction of the ciliary body and iris sphincter muscles, ultimately improving near and intermediate visual acuity (VA). 3 Approval of pilocarpine followed two 30-day phase 3 randomized double-masked trials, GEMINI 1 and GEMINI 2, both of which found a statistically significant improvement of 3 or more lines in mesopic, high-contrast, binocular, distance-corrected near VA.1,4
Since its initial reported use as a glaucoma treatment in the late 19th century, pilocarpine has been associated with many well-documented ocular adverse effects, including miosis, accommodative spasm, frontal headaches, twitching eyelids, and conjunctival and ciliary injection. The GEMINI clinical trials reported similar side effects, including conjunctival hyperemia (7.08%), blurred vision (6.13%), eye pain (5.66%), and headache (15.57%). Additional rare, yet serious, adverse effects previously reported with pilocarpine use include cataract development, iris cysts, and retinal detachments (RDs).2,5 Although informational disclosures regarding the drug warn of an increased risk for RD with the use of miotics, no detrimental retinal findings or other serious adverse events were reported among 375 randomly selected participants who received treatment in the 2 trials.1,4
To our knowledge, there are 3 reports6–8 in the literature describing retinal tears or detachments occurring as a side effect of pilocarpine 1.25% since FDA approval of the drug for presbyopia. The 5 patients (6 eyes) in these reports were of varying ages, with symptoms and factors predisposing them to adverse retinal events, including retinal tears and detachments, possibly associated with the use of pilocarpine.
We report the case of a middle-aged emmetropic man with an acute onset of a horseshoe retinal tear and vitreous hemorrhage in his left eye soon after he instilled 1 drop of pilocarpine 1.25%. After a thorough review of the patient’s clinical and ophthalmologic history and a PubMed literature search, we compared our patient’s symptoms with ocular adverse events reported in the existing literature.
Case Report
A 62-year-old White man with a medical history of well-controlled hypertension presented to the clinic with reports of floaters, hazy vision, and a tired eye 2 days after instilling 1 drop of pilocarpine 1.25% in the left eye. He said the symptoms occurred within minutes of instilling the drop.
The patient’s most recent dilated fundus examination, performed 8 weeks previously, showed preexisting tortuous retinal vessels in both eyes; a stable, chronic, benign iris nevus in the left eye; and 1+ nuclear sclerosis in both eyes. He also had lattice degeneration in the right eye but no other significant history of ocular trauma, surgeries, or procedures.
The patient’s symptoms, initially consisting of eye pain and a halo of light in the left eye, started less than 10 minutes after he instilled 1 drop of pilocarpine. He subsequently developed a tired eye and diffuse floaters the next morning, prompting him to seek ophthalmologic evaluation at a retina clinic 2 days later. On initial testing in the clinic, the uncorrected distance VA was 20/20 OD and 20/20−2 OS. The pupils were equally round and reactive to light and accommodation, and the IOP was 16 mm Hg in both eyes. A slitlamp examination showed a stable iris nevus in the left eye and 1+ nuclear sclerosis of the lens in both eyes. A dilated fundus examination found a cup-to-disc ratio of 0.2 in both eyes and peripapillary atrophy in the left eye. Scleral depression showed a horseshoe retinal tear at 12 o’clock with a mild vitreous hemorrhage and a bridging blood vessel in the left eye and lattice degeneration at 6 o’clock in the right eye. The retinal vessels were tortuous bilaterally. Retinal optical coherence tomography confirmed a complete posterior vitreous detachment (PVD) in the left eye; therefore, laser retinopexy was performed in the clinic the same day (Figure 1).
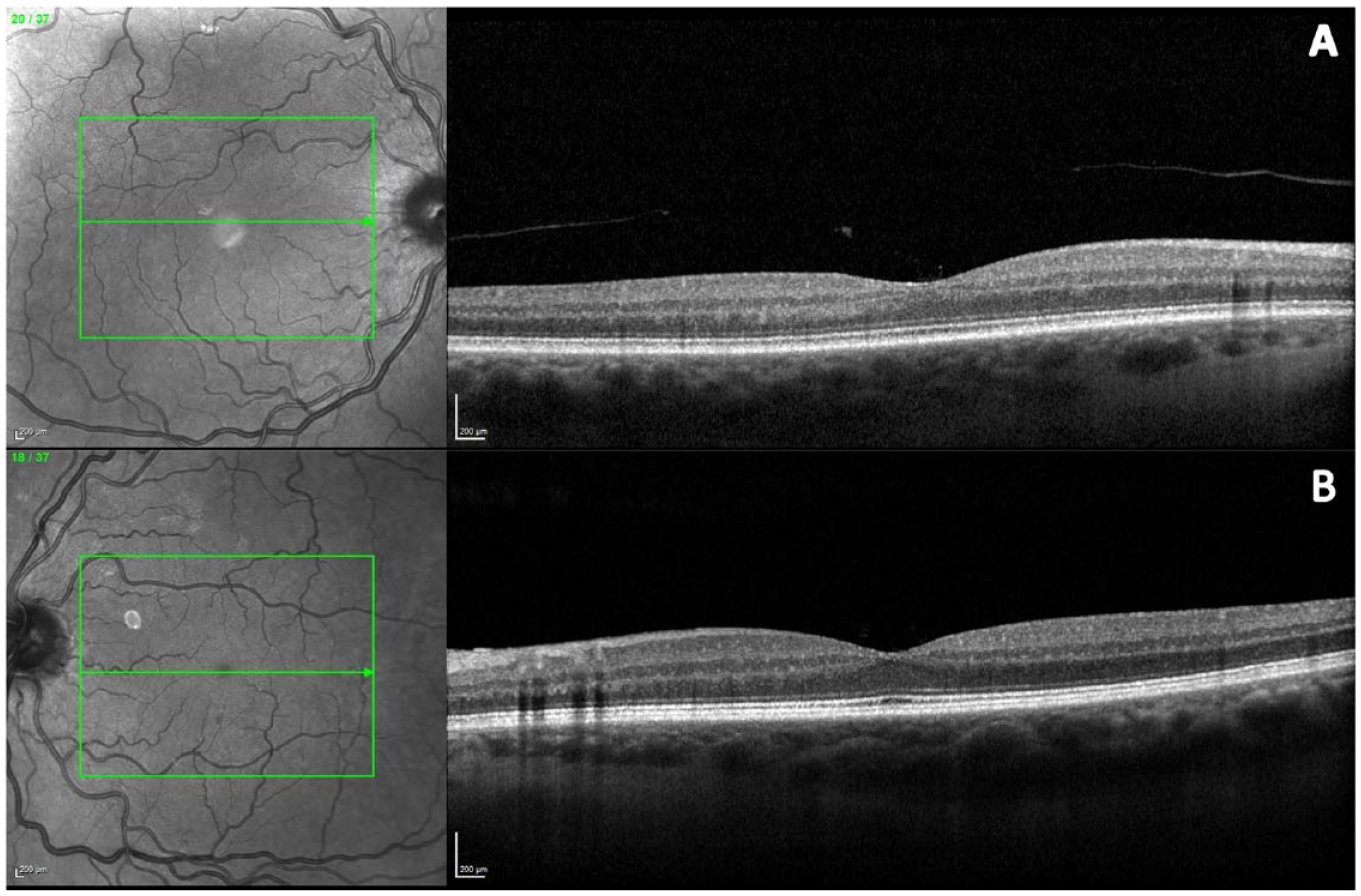
Infrared reflectance (IR) and optical coherence tomography status post pars plana vitrectomy (PPV) and endolaser of the left eye. (A) The right eye has a posterior vitreous detachment. (B) The left eye has a vitrectomized posterior pole with flat macular contour after PPV. Tortuosity of the retinal vessels is visualized bilaterally on IR images.
On day 13 after laser retinopexy in the left eye, the patient returned to the clinic because of decreased vision in his left eye caused by a “big blob” obstructing the central vision. The uncorrected distance VA remained 20/20 OD but was counting fingers at 2 ft OS. The dilated fundus examination was limited by a poor view resulting from a dense vitreous hemorrhage that developed in the left eye. A B-scan ultrasound of the left eye confirmed a PVD, vitreous hemorrhage, attached retina, and normal choroid contour.
Although the patient initially chose observation, he returned to the clinic 2 days later with worsening symptoms, including new flashes in the left eye that were central, discrete, and lasted seconds at a time. A pars plana standard core vitrectomy with endolaser was performed 4 days later, and the bridging blood vessel was cauterized with diathermy. The posterior hyaloid was detached, and the pathologic area was lasered without retinal or choroidal bleeding. The patient’s uncorrected distance VA in the left eye returned to baseline at 20/15−1. After the vitreous hemorrhage resolved, the patient had excellent vision.
Conclusions
To our knowledge, this report represents one of few studies in the literature documenting the rapid onset of adverse ocular symptoms, specifically a horseshoe retinal tear, within minutes of applying a single drop of pilocarpine hydrochloride 1.25% ophthalmic solution for presbyopic treatment. Previous reports have described various retinal complications associated with pilocarpine use for presbyopia, including retinal tears, RDs, and vitreofoveal traction.6–8 The patients’ demographics in those reports varied, ranging in age from 46 to 74 years with at least 3 of 6 eyes reported as being myopic or pseudophakic. The timing of symptom onset after initiating pilocarpine treatment was also variable, occurring between 10 minutes to 5 weeks after the initial use. Patients presented with diverse clinical symptoms, such as new-onset flashes and floaters, cloudy vision, and visual field defects. Four of 6 patients were noted to have PVDs. In addition, most cases had a significant ocular history comprising recent cataract surgery (with the most recent surgery occurring 3 months previously), a history of RDs requiring surgical management in the same eye, and lattice degeneration.6–8
Our patient similarly experienced vision disturbance that ultimately led to a diagnosis of a horseshoe retinal tear with a bridging blood vessel and PVD in the left eye. Consistent with 4 of the 5 patients previously reported, our patient was a man, possibly warranting further investigation of whether men are more likely to use pilocarpine or develop retinal tears or detachments with use of the drops.
Unlike at least half of the previously reported cases in which retinal pathologies developed in pseudophakic eyes, our patient’s eyes were phakic and he had not had previous eye surgery. In addition, the patient was emmetropic, with an axial length in the left eye of 24.22 mm measured using an IOLMaster biometer (Zeiss) and excellent VA (uncorrected distance VA 20/15 OS) before using pilocarpine for presbyopia. In contrast, at least 3 of 5 other patients were myopic, including 1 with myopia of −7.00 D. Only a single other case reported symptom onset within minutes of using pilocarpine eyedrops, similar to our patient. Furthermore, 5 of 6 previously reported cases had completely detached retinas, whereas our patient was diagnosed with a horseshoe retinal tear, vitreous hemorrhage, and PVD. Fortunately, prompt evaluation and treatment were provided to our patient within 3 days of medication use and symptom onset, underscoring the importance of educating patients about the warning signs of potential adverse effects associated with pilocarpine use for presbyopia.
Reports of retinal tears and detachments have long been associated with the use of topical pilocarpine. In 1979, a middle-aged woman with myopia and open-angle glaucoma who was treated with pilocarpine 1% developed visual symptoms within 24 hours as a result of a vitreous hemorrhage and horseshoe tears in both eyes. 9 The ora serrata and underlying choroid have been shown to move anteriorly with accommodation in response to pilocarpine, as does the posterior surface of the lens. This pharmaceutical effect suggests a pull mechanism caused by a disturbance of the anterior vitreous that may translate to the vitreoretinal interface, increasing the risk for a tear or detachment. 9
Most reports of miotic-associated RDs have occurred in myopic individuals, including those previously described after use of pilocarpine 1.25% for presbyopia. Myopic patients are predisposed to the development of an RD with the use of pilocarpine. 10 However, our patient was emmetropic; thus, myopia cannot explain why he developed a horseshoe retinal tear after the use of topical pilocarpine. Of note, myopic individuals were excluded in the GEMINI 1 and GEMINI 2 trials, which likely helped prevent any RDs from developing in the participants in the studies.
A few of our patient’s symptoms, including blurred vision, eye pain, and conjunctival hyperemia, were reported as treatment-related adverse events in the GEMINI trials. However, the studies did not report abnormal retinal findings. Only 1 of 163 participants treated with pilocarpine in the GEMINI trials reported vitreous floaters in the safety and efficacy GEMINI 1 study. 4 The clinical trials specifically focused on individuals aged 40 to 55 years, representing a significant portion of the presbyopic population who are potential candidates for topical miotic use. This age range may not encompass everyone who may be prescribed this medication, and limiting the age range to a maximum of 55 years could have potentially resulted in the underdetection of serious ocular events associated with the new formulation. In addition, the study’s follow-up of 30 days after the last use of pilocarpine may not have captured potentially related adverse effects, such as the case of vitreofoveal traction observed 5 weeks after initiating pilocarpine use for presbyopia management. 8
This report has limitations. Our patient may not have been an ideal candidate for pilocarpine use given the preexisting tortuous retinal vessels in both eyes and lattice degeneration in the left eye noted on his last dilated fundus examination. The patient also would not have met the inclusion criteria because he was 7 years older than the age range studied in the GEMINI safety and efficacy trials. Given these predisposing factors, it is possible that our patient could have coincidentally developed a horseshoe retinal tear and PVD without the use of pilocarpine minutes before the onset of symptoms.
Despite having mild preexisting retinal changes related to well-controlled hypertension and aging, this 62-year-old man affected by presbyopia represents a large portion of the targeted population—middle-aged, presbyopic individuals attracted to the possibility of using an eyedrop instead of reading glasses to improve their near VA. Patients are increasingly being prescribed pilocarpine for presbyopia; thus, our case and other reported cases may help identify previously reported and unknown risk factors that predispose patients to adverse retinal events associated with use of pilocarpine.
When prescribing topical pilocarpine for presbyopia, a comprehensive ophthalmic examination, including a dilated fundus examination, should be performed to screen for predisposing factors that may increase the risk for retinal tears or detachments. Patients at an elevated risk for developing vitreoretinal pathologies should be informed about the increased risk associated with the use of miotics, including pilocarpine. Even patients who are not considered at high risk should be educated about the potential adverse effects of pilocarpine use and be made aware of the warning signs of retinal tears or detachments. To confirm and establish the risks associated with the use of pilocarpine for presbyopia, future studies should compare and analyze the existing literature as well as findings that emerge after its FDA approval.
Footnotes
Ethical Approval
Ethical approval was not required for this case report.
Statement of Informed Consent
The patient provided written informed consent to access and publish his medical information and records before their review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded in part by the Retina Research & Development Foundation.