
Abstract
Introduction
Nocardia is aerobic, gram-positive, weakly acid-positive, filamentous, branching bacillus that is ubiquitous in the environment; it is found in the soil, soil-contaminated water, deep sea sediments, and desert habitats.1–4 In humans, Nocardia species can cause infections of the skin, lungs, and central nervous system (CNS) as well as systemic nocardiosis, especially in immunocompromised patients. 1 In the eye, Nocardia can cause keratitis, keratoconjunctivitis, scleritis, dacryocystitis, orbital cellulitis, and endophthalmitis (both exogenous and endogenous).1,3
Postoperative Nocardia endophthalmitis has a delayed onset of infection after cataract surgery and usually carries a guarded visual prognosis.1–4 Here, we report a case of postoperative Nocardia endophthalmitis that proved to be challenging.
Case Report
A 64-year-old hypertensive woman presented reporting diminished vision and redness in the right eye 1 month after uneventful cataract surgery. The patient had good vision early in the postoperative period. On postoperative day (POD) 12, she noticed decreased vision, pain, and redness in the right eye. The best-corrected visual acuity (BCVA) was hand motions OD and 6/7.5
An examination of the right eye found conjunctival and circumciliary congestion with exudates in the anterior chamber over the pupillary area and with no view of the fundus. The examination of the left eye was essentially normal. Ultrasonography showed multiple dot and membranous vitreous echoes with an attached retina in the right eye. The patient was diagnosed with postoperative endophthalmitis and had a vitrectomy. Intraoperatively, exudates were found to be more concentrated around the intraocular lens (IOL); therefore, IOL explantation was planned. Treatment comprised intravitreal (IVT) vancomycin and ceftazidime.
A vitreous aspirate and the IOL were sent for culture, with samples inoculated into brain heart infusion broth for aerobic isolation and thioglycolate medium for anaerobic growth. After 48 hours of incubation, granular growth was observed in the brain heart infusion broth. Filamentous, gram-positive, acid-fast bacilli were noted on the smear with application of Ziehl-Neelsen staining. Dry, white, wrinkled nonhemolytic colonies were grown on the blood agar subculture (Figure 1A). Based on these characteristics, a presumptive identification of Nocardia species was made. Speciation of Nocardia was performed with 16S rRNA gene polymerase chain reaction–based sequencing using the ABI 3130 genetic analyzer (Applied Biosystems). Based on the homology match in the National Center for Biotechnology Information database, Nocardia puris, a bacterium sensitive to amikacin, vancomycin, moxifloxacin, gatifloxacin, trimethoprim–sulfamethoxazole, tobramycin, and ciprofloxacin, was identified.
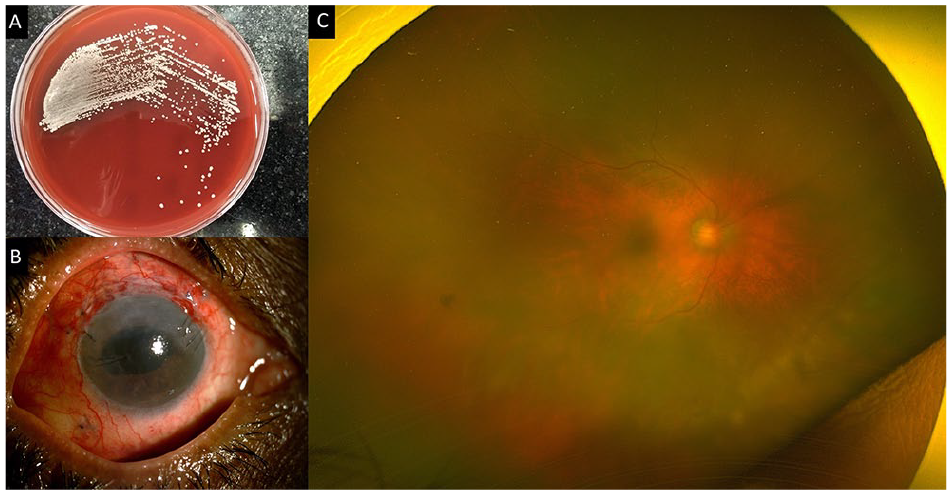
(A) A subculture of the liquid medium (brain heart infusion broth) inoculated with the intraocular lens onto blood agar shows dry, white, wrinkled nonhemolytic colonies, suggestive of Nocardia species. (B) Slitlamp images and (C) fundus images on postoperative day 4 show no exudates in the anterior chamber, with a clearing vitreous cavity and attached retina.
The patient was treated with intravenous amikacin (250 mg twice a day) and intracameral amikacin (125 µg/0.1 mL), with vancomycin (1 mg in 0.1 mL) with proper dilution on alternate days. On POD4, no exudates were seen in the anterior chamber, with an improving view of the fundus and an attached retina (Figure 1, B and C). However, on POD6, multiple intraretinal hemorrhages and whitening of the posterior pole were seen (Figure 2A), suggestive of an amikacin-induced macular infarction. Fundus fluorescein angiography confirmed the findings (Figure 2, B and C). IVT injections were deferred, and the patient was started on oral ciprofloxacin (500 mg twice a day) and observed closely for 3 to 4 days. On POD10, clinical improvement was seen, with no iris nodule, hypopyon, or vitreous haze. There was no recurrence of infection or inflammation.
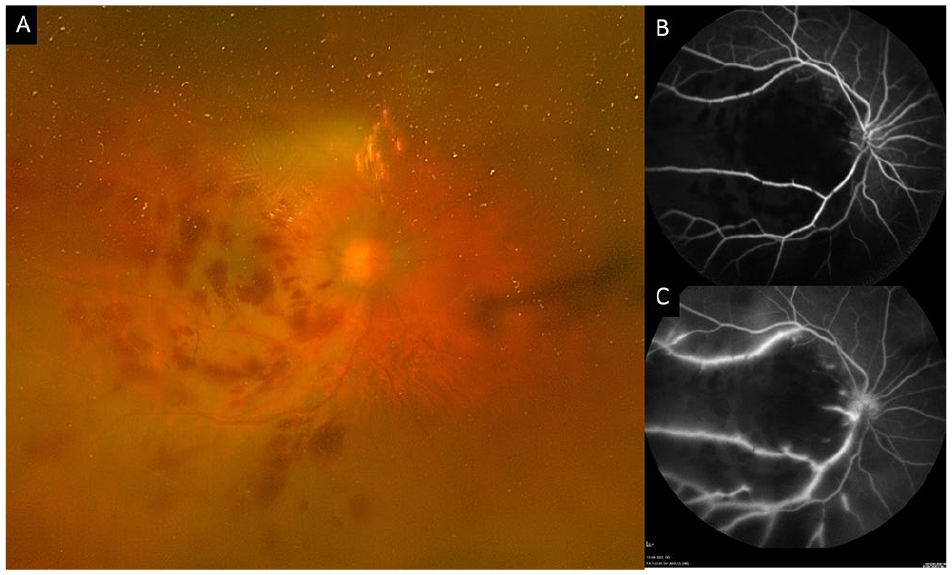
(A) Ultra-widefield image and (B and C) fundus fluorescein images on postoperative day 6 depict retinal hemorrhages and a macular infarction resulting from treatment with amikacin.
For personal reasons, the patient opted to follow up weekly with her primary ophthalmologist. She presented at the 1-month follow-up visit with a recurrent infection in the form of an iris nodule and vitritis (Figure 3A) and was restarted on intracameral ciprofloxacin injections. In light of the inadequate response to treatment, an infectious disease specialist was consulted, and the patient was started on oral trimethoprim–sulfamethoxazole (double strength, 800/160 mg twice a day) and moxifloxacin (400 mg twice a day). Based on experience with the management of systemic nocardiosis, the infectious disease specialist insisted that systemic treatment should be continued for a prolonged time (roughly 6 months). The iris nodules regressed in size (Figure 3B), and no new lesions were noted on close subsequent follow-up. There was no recurrence of infection at the patient’s 2-month follow-up (Figure 4, A and B) and 6-month follow-up (Figure 4, C and D). The BCVA was counting fingers at 50 m as a result of the macular infarction. The patient was instructed by the infectious disease specialist to continue moxifloxacin and trimethoprim–sulfamethoxazole for an additional 3 months.
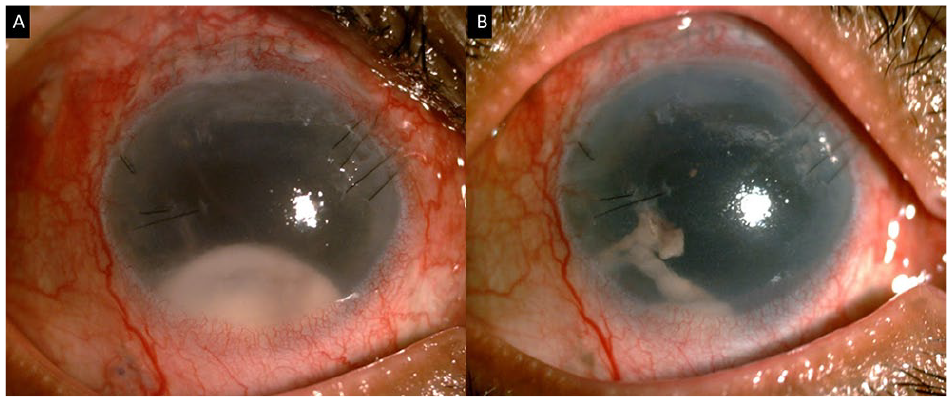
(A) Recurrence of infection (iris nodule) at the 4-week follow-up. (B) Reduction in the size of the iris nodule at the 6-week follow-up, 2 weeks after the patient began systemic treatment with trimethoprim–sulfamethoxazole and moxifloxacin.
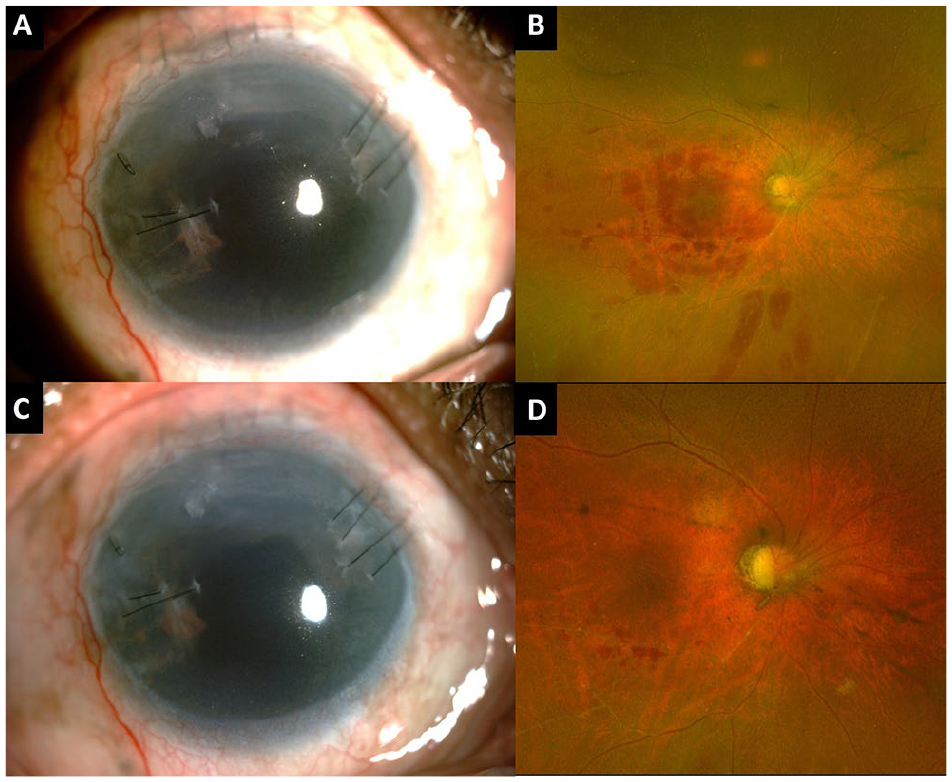
Slitlamp and ultra-widefield images at (A and B) the 3-month follow-up and (C and D) the 6-month follow-up show the absence of recurrent infection (no anterior chamber exudates or iris nodule, clear vitreous cavity, attached retina). By the 6-month follow-up, the retinal hemorrhages have also decreased in size.
Conclusions
Nocardia endophthalmitis is rare, occurring exogenously (after surgery or as a result of trauma) or endogenously. In general, it is associated with poor visual outcomes. 3 Postoperative Nocardia endophthalmitis usually presents as a delayed infection; however, some studies reported an early presentation.1–4 The pathognomonic findings of Nocardia endophthalmitis include fluffy exudates in the anterior chamber with iris nodules, as seen in our case. 3 A fibrinous membrane surrounding the IOL is typically described. 3 Although IVT ceftazidime and vancomycin are the first-line empirical drugs for suspected endophthalmitis cases in India, these are not effective for Nocardia endophthalmitis. Because amikacin has been reported to have the highest antibiotic sensitivity for Nocardia species (90% to 100%), it has been considered the first-line treatment for Nocardia endophthalmitis.1–6
Although macular ischemia is a rare complication after IVT amikacin injection, it has been reported after vitrectomy with IVT injection as well as after the IVT injection alone.2,3 Macular ischemia should be differentiated from hemorrhagic occlusive retinal vasculitis associated with vancomycin, 7 which is characterized by sectoral intraretinal hemorrhages in areas of nonperfusion (often along venules), typically in the peripheral retina. 7 In amikacin toxicity, the macula is commonly involved, whereas peripheral retinal vascular occlusion is unusual. 7 In contrast, peripheral involvement is common in hemorrhagic occlusive retinal vasculitis, with more severe cases exhibiting macular ischemia and whitening. 7 Factors contributing to amikacin-induced retinal toxicity include dilution errors, increased intraocular pressure after IVT injection, variation in the liquefaction status of the vitreous humor, supine position after injection, and individual susceptibility. 2 Although the exact predisposing factor for macular infarction in this case is unclear, it may be that the treatment was repeated too soon. Caution must be exercised when using IVT amikacin, and injections should not be repeated every 48 hours, especially in vitrectomized eyes.
Structures in the anterior chamber (eg, iris, ciliary body, and IOL) can harbor elements of Nocardia, and this deep infiltration can lead to complications such as persistent intractable infection, resulting in phthisis. 3 Such chronic intraocular Nocardia infections respond very poorly to any form of treatment, even though isolates show in vitro drug sensitivity.3,5 We suspect that this patient could have had such a deep-seated infection (probably behind the iris and/or ciliary body) that was initially indolent (showing early transient improvement) but persisted, leading to late recurrence. The disease course was more suggestive of a persistent smoldering infection rather than of a repeat infection. Use of iris hooks in patients with endophthalmitis who have IOL explantation is important because it provides proper visualization of the retroiridal space, thereby minimizing recurrences by ensuring complete removal of the capsular bag and exudates. In addition, this case emphasizes the importance of close and frequent follow-up in cases of Nocardia endophthalmitis.
In our case, treatment comprised trimethoprim–sulfamethoxazole, which is the most common drug used in systemic nocardiosis, especially when the CNS is involved. 8 Combination therapy, including trimethoprim–sulfamethoxazole with amikacin or meropenem or linezolid, is typically preferred in severe cases.8,9 Based on the sensitivity report, trimethoprim–sulfamethoxazole and moxifloxacin were suggested for our patient. Several reports propose that pulmonary and soft tissue infections be treated for at least 6 months and that disseminated disease should be treated for 6 to 12 months, with the exact duration dependent on the response to therapy and resolution of disease. 9 Based on this, prolonged systemic therapy (6 to 9 months) was recommended for our patient and helped control the infection, as did frequent follow-up visits to monitor for recurrence.
In cases of suspected Nocardia endophthalmitis, obtaining a microbiological diagnosis with sensitivity is essential followed by the careful selection of antibiotics. Clinicians should use caution when using IVT amikacin and should clearly explain to the patient the potential for a poor visual prognosis, the need for aggressive treatment, and the need for a prolonged follow-up. In addition, recurrences should be anticipated and managed similarly, with changes as needed to other IVT or systemic antibiotics to which Nocardia is sensitive.
This case report presents the challenges involved in managing Nocardia endophthalmitis. Delays in diagnosis may lead to a chronic infection state, resulting in recurrences and poor visual outcomes; hence, prolonged treatment with systemic antibiotics and frequent follow-up are required.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a US Health Insurance Portability and Accountability Act–compliant manner.
Statement of Informed Consent
The patient provided informed consent, including permission for publication of all photographs and images included herein.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.