
Abstract
Keywords
Introduction
Step therapy is a treatment approach often required by health insurers with the intent of controlling costs. The approach typically requires initial treatment with a lower cost medication, and only after that treatment proves ineffective is the physician allowed to switch to an alternative medication. 1 The goal of such a strategy is to pursue cost savings without sacrificing treatment efficacy. However, unintended consequences might include restricting the treating physician’s ability to select the most efficacious and expedient treatment for the patient, adding additional administrative and clerical burdens, and delaying patient improvements. Despite these concerns, the step therapy treatment algorithm is increasingly mandated by payers across various medical specialties and is commonly applied in the treatment of hypertension, diabetes, cancer, and other medical conditions. Concerns regarding its potential for long-term harm to the patient have led some to view it as “fail first” therapy.2,3
Step therapy is increasingly relevant to retina specialists and their patients with the growing armamentarium of intravitreal (IVT) antivascular endothelial growth factor (anti-VEGF) compounds. Aflibercept (Eylea 2 mg) and Eylea-HD (8 mg) (Regeneron, Inc), ranibizumab (Lucentis, Genentech, Inc), faricimab (Vabysmo, Genentech, Inc), and ranibizumab biosimilars have been approved by the US Food and Drug Administration (FDA) for the treatment of diabetic macular edema (DME).
In Diabetic Retinopathy Clinical Research Network (DRCR) Protocol T, aflibercept 2 mg and ranibizumab were found to be superior to bevacizumab (Avastin, Genentech, Inc), which has been used off-label and at a lower cost. 4 Persistent DME was also more likely with bevacizumab than with aflibercept or ranibizumab. 5 DRCR Protocol AC studied a simulated step therapy clinical scenario for the treatment of DME, comparing a bevacizumab-first group with an aflibercept-monotherapy group over 2 years; sub-responders in the bevacizumab-first group could be switched to aflibercept beginning at week 12 based on predefined criteria. 4 Protocol AC reported similar visual acuity (VA) gains and improvements in central subfield thickness in both arms at the 2-year timepoint, although the aflibercept monotherapy group responded more rapidly. The mean VA improvement at 2 years was 14.0 letters in the bevacizumab-first group and 15.0 letters in the aflibercept-monotherapy group. Significantly, 70% of eyes in the bevacizumab-first group required a switch to aflibercept by the end of 2 years. 6
Based on Protocol AC, the DRCR Retina Network suggested that step therapy with bevacizumab could be cost saving in the treatment of DME. In a follow-up analysis, the DRCR Retina Network compared modeled costs from the bevacizumab-first arm of Protocol AC to the aflibercept-monotherapy arm and found a 47.4% reduction in costs ($26,504 vs $13,929). 7 Although their analysis found that bevacizumab-first treatment may be cost saving compared with aflibercept monotherapy in a research setting, these findings may not be applicable to real-world clinics given that a similar intensive protocol of treatment is unlikely to be feasible.
The purpose of this analysis was to model the relative cost of protocol-mandated DME treatment with bevacizumab-first treatment in Protocol AC vs real-world DME treatment that reflects physician choice.
Methods
This study compared modeled costs derived from published data of DRCR Protocol AC with real-world costs from the Vestrum Health retina database (Vestrum Health, LLC). The retina database is an aggregated, longitudinal database of electronic medical records from a demographically and geographically diverse patient sample, which was obtained from a panel of retina specialists in the United States. The names of the treating physicians and practices had been removed from the data. All patient information was de-identified in accordance with the regulations of the US Health Insurance Portability and Accountability Act of 1996. The current study was considered exempt from institutional review board review because the research involved the collection of retrospective and de-identified data. All research was conducted in accordance with the Declaration of Helsinki.
Real-world costs were modeled from the Vestrum Health retina database for a cohort of treatment-naïve eyes with DME with at least 2 years of follow-up. Included eyes had a VA of 20/50 to 20/320 at the baseline visit with a diagnosis of DME at presentation, similar to the inclusion criteria in Protocol AC. A secondary analysis also matched vision gains in the real-world cohort and those in Protocol AC by progressively excluding eyes with the lowest vision improvements (or highest vision loss). Eyes with a diagnosis of age-related macular degeneration, retinal vein occlusion, or myopic choroidal neovascular membrane at any point during the 2-year follow-up were excluded. They were also excluded if they received IVT or periocular steroids or focal laser treatment during the study period. Only eyes that started receiving treatment in 2016 were included; this year was deliberately selected to incorporate the influence of the 2015 Protocol T results, 8 which showed increased efficacy of aflibercept compared with bevacizumab, while minimizing the effects of more recent increases in step therapy mandates that restrict physician choice.
For the Protocol AC cost analysis, the number of visits, images (fundus photographs and optical coherence tomography [OCT]), and injections as well as the percentage of bevacizumab treatments vs aflibercept treatments were as published. 4 Although this study focused on a cost comparison between the real world vs the Protocol AC bevacizumab-first arm, the cost of the Protocol AC aflibercept-only arm was also analyzed. The real-world analysis was based on actual utilization data harvested from the Vestrum database, including the number of visits, images (fundus photographs and OCT), and injections as well as the percentage of bevacizumab treatments vs aflibercept treatments vs 0.3 mg ranibizumab treatments.
For both Protocol AC and the real-world analysis, the model assumed 1 initial new comprehensive evaluation and management (E/M) code (99204) per eye, with the remaining appointments billed with comprehensive established E/M codes (99214). Imaging use in Protocol AC included OCT (CPT 92134) at every visit and annual fundus photographs (CPT 92250) as published, while OCT and fundus photograph use in the real-world setting was based on actual Vestrum data. The study model included the allowable cost of each visit, injection, drug administered, and OCT and fundus photograph. The most up-to-date cost data at the time of this analysis were used from the 2022 Centers for Medicare and Medicaid Services fee schedule (nonfacility setting, national payment amount) and the December 2022 Medicare Part B Drug and Biological Average Sales Price (Table 1). 7
Cost of Modeled Professional Fee and Drug Components.
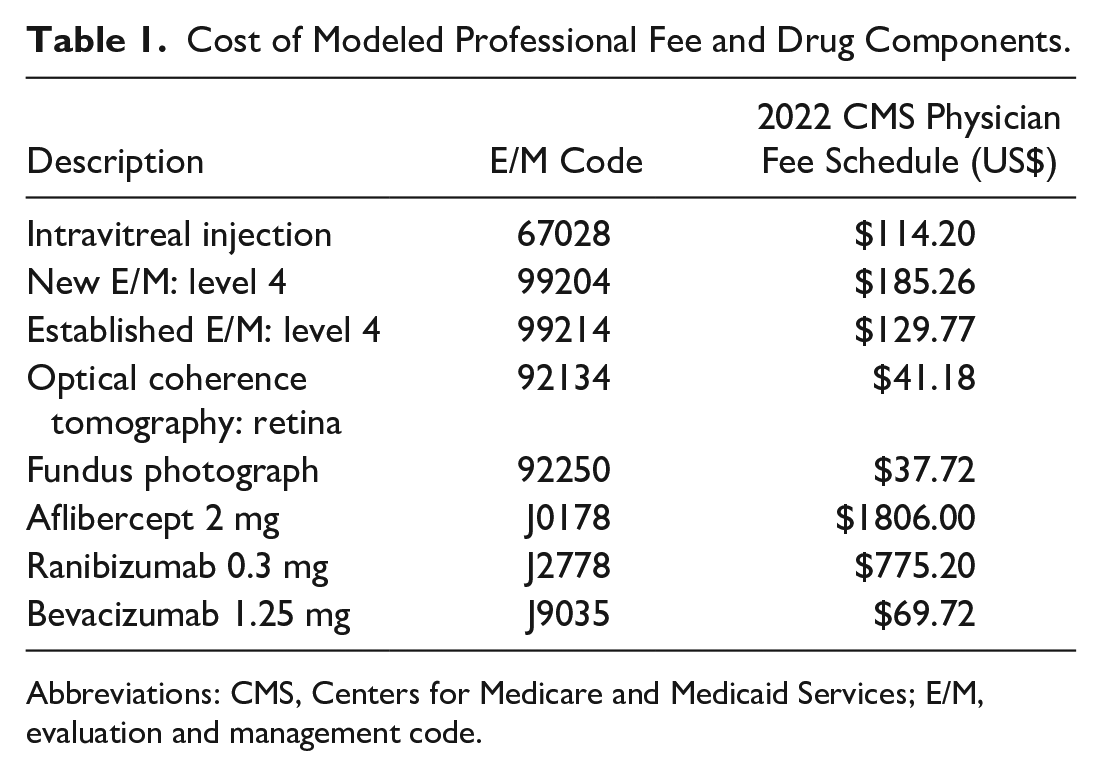
Abbreviations: CMS, Centers for Medicare and Medicaid Services; E/M, evaluation and management code.
The primary cost analysis was performed assuming that an examination was billed with each injection (ie, 100% use of modifier 25 billed with the injection). The primary analysis also assumed that fundus photographs could be billed along with OCT images at the same visit. One-way sensitivity analyses were also performed, removing these assumptions such that an E/M code would not be billed if an injection was performed and fundus photographs would not be billed at the same visit with OCT (ie, removing the cost of fundus photographs from the model).
Results
Protocol AC included 154 eyes in the bevacizumab-first arm and 158 eyes in the aflibercept-only arm, as published. 6 The median patient age was 61 years and 60 years, respectively. The median baseline VA was 60 letters in the bevacizumab-first arm and 61 letters in the aflibercept-only arm (~20/63 Snellen equivalent) and improved to a median of 73 letters and 72 letters (20/40 Snellen equivalent), respectively, at 2 years, representing a mean gain of 14 letters in the bevacizumab-first group and 15 letters in the aflibercept-only group. The bevacizumab-first arm received a mean of 16.1 injections (over a mean of 22.5 visits) compared with 14.6 injections in the aflibercept-monotherapy arm (over 22.5 visits). In the bevacizumab-first arm, 70% of eyes were switched to aflibercept by year 2, with an overall proportion of 57% bevacizumab injections (mean, 9.1) and 43% aflibercept injections (mean, 6.9) by year 2. 4 In the aflibercept-only arm, 100% of injections (mean, 14.6) were aflibercept during the study.
The real-world Vestrum analysis identified 1556 eyes that initiated anti-VEGF treatment in 2016 for DME with a 20/50 to 20/320 baseline VA. Of these, 494 eyes were excluded because they received treatment with IVT steroids and/or laser in addition to anti-VEGF therapy during the 2-year follow-up. This analysis included the remaining 1062 eyes with treatment-naïve DME that were treated with anti-VEGF monotherapy and followed over 2 years.
The mean age of the real-world cohort was 61.7 years, with 53% men and 47% women. The mean VA at the time of diagnosis in this cohort was 53.9 letters (~20/80 Snellen equivalent) and improved to 59.8 letters (~20/63 Snellen equivalent) at year 2, representing a gain of 5.8 letters. The proportion of injections in the 2-year treatment period was 42% bevacizumab, 45% aflibercept, and 13% ranibizumab (mean, 13.8 visits and 8.6 injections over 2 years).
After modeling the cost of each examination, drug, IVT injection, and imaging (OCT and fundus photographs), the real-world 2-year cost of DME treatment was $11,459 (Table 2). The real-world cost was 39.5% lower than the modeled Protocol AC bevacizumab-first cost ($18,952) (Table 2) and 64.2% lower than the modeled Protocol AC aflibercept-monotherapy cost ($31,964).
Modeled Protocol AC Bevacizumab-First Costs vs Real-World Costs Over 2 Years.
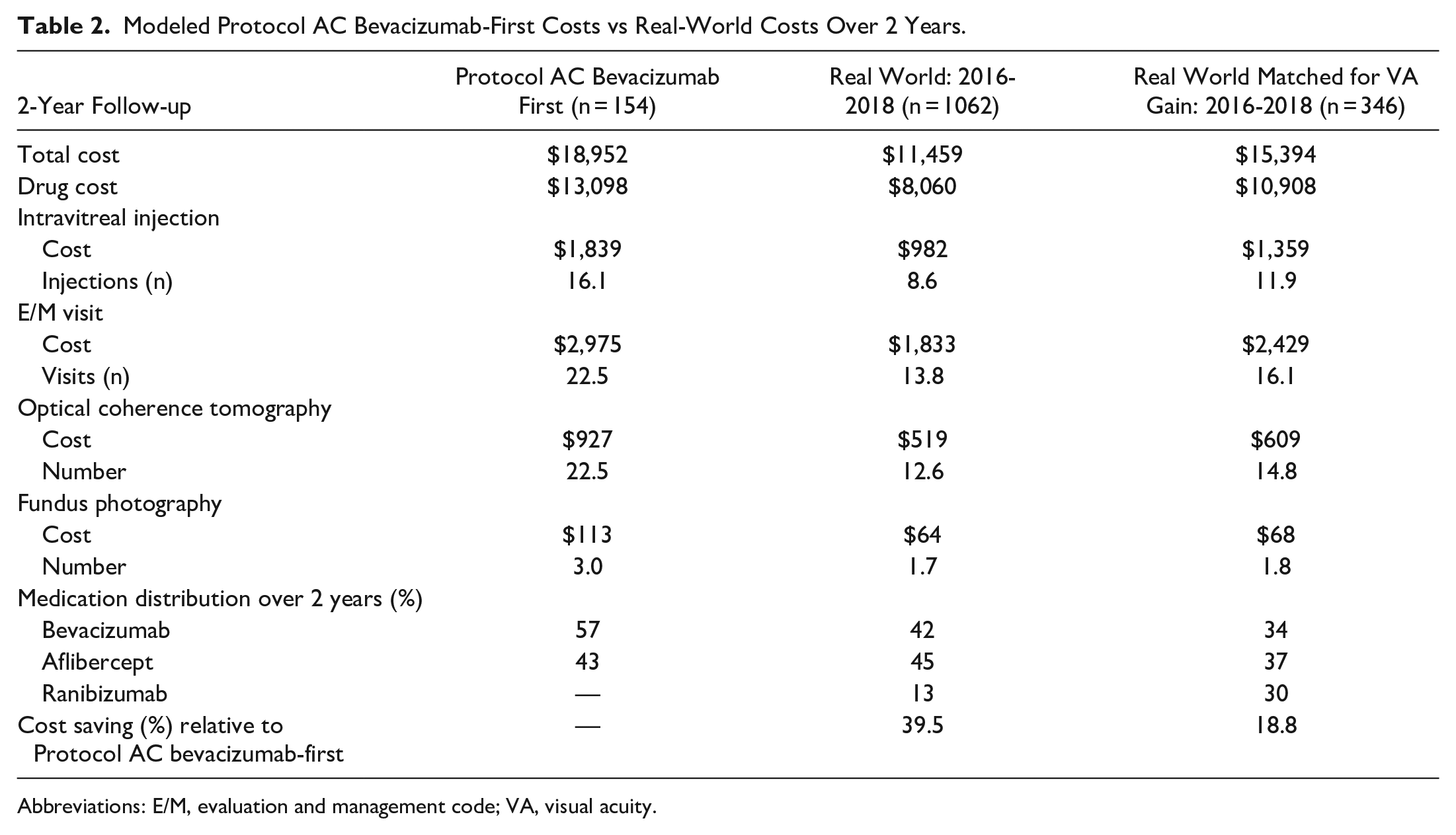
Abbreviations: E/M, evaluation and management code; VA, visual acuity.
Given the variability in the use of modifier 25 to bill for an E/M service separate from the injection procedure, a sensitivity analysis modeling cost was performed without using modifier 25 (ie, removing the cost of the E/M code when an injection was performed). The impact of bundling fundus photographs with OCT (ie, removing the cost of fundus photographs) was also modeled. These modifications, even combined, had a minimal impact on the modeled cost savings in the real-world cohort vs the Protocol AC bevacizumab-first arm (−38.7%; $10,236 vs $16,694) and vs the Protocol AC aflibercept-only arm (−65.8%; $10,236 vs $29,901).
Given the discrepancy in VA outcomes in the real-world cohort (5.9 letters) vs Protocol AC (14-15 letters), a secondary cost analysis was performed for a subset of the real-world cohort selected for a mean 2-year VA gain of 14.2 letters (n = 346) to match the VA outcomes in Protocol AC. This secondary cohort had a similar baseline VA of 57.2 letters compared with 57.2 letters in the bevacizumab-first group and 58.8 letters in the aflibercept-monotherapy group. Even in this secondary cohort, which was matched for both baseline VA and VA outcomes over the 2-year period, the real-world costs ($15,394) were still 18.8% lower than the modeled 2-year cost in the bevacizumab-first arm in Protocol AC (Table 2).
In the subgroup of patients whose VA gains were matched, sensitivity analyses removing the use of modifier 25 (ie, removing E/M costs at injection visits) and accounting for the impact of bundling fundus photographs with OCTs (ie, removing the cost of fundus photographs) had a minimal impact on the modeled cost savings, with the real-world cost being 19.6% lower than that of the Protocol AC bevacizumab-first treatment ($13,422 vs $16,694).
Conclusions
The current study compared the cost of DME treatment with anti-VEGF monotherapy in the real world vs the bevacizumab-first arm in DRCR Protocol AC. 4 The authors of the current study were not DRCR Retina Network investigators, and this study is not a product of the DRCR Retina Network.
We found that the 2-year treatment cost was 40% lower in real-world practice than in the Protocol AC bevacizumab-first arm in treatment-naïve eyes matched for baseline VA. When the real-world cohort was further matched for VA gain over the 2-year period, real-world costs were still 19% lower than in the Protocol AC bevacizumab-first arm. One-way sensitivity analyses accounting for differences in the use of modifier 25 and bundling of images supported the robustness of the model. Real-world treatment of DME was less costly than the Protocol AC bevacizumab-first treatment regimen.
The DRCR Retina Network published a follow-up cost analysis from Protocol AC comparing their bevacizumab-first arm and their aflibercept-monotherapy arm. Their analysis identified a 47.4% cost savings of bevacizumab-first therapy vs aflibercept monotherapy despite equivalent vision outcomes at 2 years, and the authors concluded that the bevacizumab-first approach may confer “substantial cost savings on a societal level.” However, these findings must be interpreted cautiously and in context. DRCR Protocol AC was a highly controlled clinical trial with aggressive monthly treatment, close surveillance, and opportunities for escalation of care based on anatomy and vision. Patients receiving bevacizumab required more frequent follow-up visits than those receiving aflibercept. Real-world data suggest that such an intensive treatment and follow-up interval is often not possible. Indeed, the frequency of Protocol AC follow-up visits was much greater than observed in our real-world cohort, even when accounting for similar vision improvement over 2 years.
Visit frequency is a concern that is especially pertinent for patients with diabetes, who are often of working age, have a limited number of sick days, may have difficulty driving because of their vision, might require caretakers to help with transportation, and/or have numerous coexisting conditions that make it more difficult for them to adhere to frequent follow-up visits. This real-world population is not well-reflected in a clinical trial setting in which selection bias favors compliant and non-underrepresented populations. Missed or delayed follow-up visits in clinical practice could result in failure to identify vision loss early and initiate a switch in therapy. 9 In the Protocol AC bevacizumab-first arm, 70% of eyes required a switch to aflibercept over 2 years because of a suboptimal response with bevacizumab. Prompt identification of a suboptimal response in a clinical trial setting might not be possible in the real world. Conclusions from Protocol AC should not be extrapolated to the real world unless the same intensive, and likely unachievable, guidelines were applied.
In the real world, highly trained retina specialists use their expertise to select optimal treatment programs for each individual patient to maximize therapeutic effectiveness as quickly as possible and decrease treatment burden. The current analysis shows that real-world treatment patterns, which reflect physician choice, allow significant cost reduction compared with Protocol AC, even when matched for vision outcomes.
The current analysis at 2 years likely underestimates the cost saving of the real world compared with Protocol AC. Only the direct costs of patient care were included in this model, which did not include indirect costs or societal costs, such as loss of productivity, patient-time costs, unpaid caregiver-time costs, and transportation costs, all of which would likely be greater in Protocol AC than in the real world given the more intensive visit requirements. Extrapolation of these results beyond 2 years would likely further increase these relative cost differences, as has been modeled by others. 10 The current model also did not include recently approved and pipeline therapies that may have longer durations of action and further reduce the number of required injections, which might further increase differences between Protocol AC and real-world treatments.
We acknowledge several limitations of the current analysis. The costs reflect modeling and were not actual costs, and the accuracy of the modeling depends on assumptions made. The modeled costs were higher than those modeled in the previously published DRCR Retina Network cost analysis of Protocol AC, 7 which could be the result of cost differences attributed to different assumptions. For example, the current analysis assumed a level 4 E/M code for each visit, reflecting the complexity of decision-making inherent in treatment of DME, while the DRCR analysis assumed a lower level 3 E/M code. Along the same lines, the current analysis assumed use of modifier 25 to include the cost of the visit and the same-day injection procedure, while the DRCR analysis only accounted for the cost of visits apart from an injection day. However, the 1-way sensitivity analyses removing the level 4 E/M codes and fundus photographs did not significantly alter the cost differential and the bevacizumab-first arm was still similarly more expensive than the real-world model. Finally, the DRCR cost analysis included participants with only 1 study eye enrolled, resulting in fewer eyes and visits than reported in the original Protocol AC dataset, which was used for this analysis. Although these different assumptions resulted in different absolute cost estimates, the relative difference of $12,575 between the bevacizumab-first arm and aflibercept-only arm modeled in the DRCR analysis was similar to the modeled difference of $13,012 in the current study. These different assumptions likely would not have a meaningful effect on the cost differences identified in this study.
Real-world modeling was based on analysis of the Vestrum database, which lacks the granularity and precision of data, including imaging data, that are available in a clinical trial dataset. The model was limited to new patients for whom treatment was initiated; however, it is possible that some patients may have received previous treatment elsewhere. In the Vestrum analysis, it was not possible to determine whether some visits were for reasons other than treatment of the study eye, and the findings may have included visit costs for the fellow eye and therefore underestimated cost savings in the real-world model vs Protocol AC. Unlike in Protocol AC, which had a set of strict inclusion and exclusion criteria (eg, exclusion of patients with advanced proliferative diabetic retinopathy), the real-world analysis matched only baseline vision and vision outcomes in the setting of a DME diagnosis; unmeasured differences in populations may have influenced the outcomes and cost. This model included only aflibercept, 0.3 mg ranibizumab, and bevacizumab; cost-effectiveness data for other FDA-approved agents, such as faricimab, 8 mg aflibercept, and biosimilars, are currently lacking. With the introduction of pharmacotherapies that may have a longer duration of action, the number of required visits might be further reduced, increasing real-world cost savings over time.
Drug selection in Protocol AC was based on prespecified treatment and switch criteria. In the real-world analyses, it was not possible to ascertain the reasons for drug selection, which may have been influenced by non-patient factors, including insurance requirements, practice and/or physician preferences for FDA-approved vs off-label drug use, concerns over silicone oil bubbles in the syringes, and repackaging concerns. The 2016 timing for the initiation of treatment in this real-world analysis was purposefully selected to account for likely increased real-world aflibercept use after the 2015 publication of DRCR Protocol T results, which show the superiority of aflibercept for DME treatment. 11 This time period also permitted us to minimize the effect of more recent step therapy mandates by insurance carriers requiring initial bevacizumab use in the real world. We were interested in current costs; therefore, the most recent published fee schedules (2022) were used.
There are undoubtedly long-term economic concerns associated with increasing anti-VEGF use, which coupled with the large treatment and surveillance burden, motivate cost-effectiveness analyses. 12 Insurance carriers have increasingly used step therapy, with lower cost treatments required first as a purported cost-saving mechanism despite the absence of real-world data supporting its clinical equivalency for the treatment of retinal diseases. The DRCR Retina Network Protocol AC showed equivalent 2-year vision outcomes and a lower cost of DME treatment with bevacizumab-first therapy than with aflibercept monotherapy; however, these findings were in the setting of a strict clinical trial protocol. The current analysis identified significantly higher costs with bevacizumab-first treatment than with real-world treatment. Retina specialists incorporate their expertise and clinical judgment, personalized for the treatment of each individual patient, and protocols that interfere with physician choice should be thoroughly considered and evaluated before implementation.
Footnotes
Authors’ Note
Presented at the annual meeting of the American Society of Retina Specialists, July 28–August 1, 2023, Seattle, WA, USA, and the annual meeting of the American Academy of Ophthalmology, November 3–6, 2003, San Francisco, CA, USA.
Ethical Approval
No human subjects were involved; therefore, institutional review board approval was not required.
Statement of Informed Consent
No human subjects were involved; therefore, informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Grewal: Genentech (consultant); Regeneron (consultant). Dr. Niles: Regeneron (consultant). Dr. Kolomeyer: Alimera (consultant); Apellis (consultant); Biogen (speaker, consultant); Genentech (speaker, consultant); IvericBio/Astellas (speaker); Regeneron (speaker, consultant). Dr. Kim: Genentech/Roche (advisory board); Outlook Therapeutics (advisory board); Regeneron (advisory board). Dr. Hahn: Adverum (consultant, advisory board); Alimera (advisory board); EyePoint (speaker, consultant, advisory board); Genentech (speaker, consultant, advisory board). None of the other authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.