
Abstract
Keywords
Introduction
Macular hole (MH) surgery has evolved since the publication of an initial study in 1991 by Kelly and Wendel. 1 Although pars plana vitrectomy (PPV) can achieve anatomic and functional recovery of MHs, vitreoretinal surgeons are continuously striving to achieve higher anatomic closure rates and better visual acuity (VA). Internal limiting membrane (ILM) peeling, first described by Eckardt et al, 2 has improved the closure rate of idiopathic MHs by more than 90%. Subsequently, indocyanine green (ICG) was introduced as the first vital dye to stain the ILM, helping surgeons visualize and peel the ILM. 3 Other vital dyes, such as brilliant blue G and trypan blue, have also been shown to be effective staining agents. 4 However, surgeons must consider the safety of the vital dyes, especially ICG.
In 2009, Michalewska et al 5 described an inverted ILM flap technique that increased the closure rate of large MHs (>400 μm). Since then, multiple modifications to techniques have been made to achieve better surgical outcomes for different types of MHs. However, potentially toxic vital dyes carried by the ILM flap may spread to the photoreceptor layer around the MH and the retinal pigment epithelium (RPE) layer beneath the MH.6,7 In recent years, there have been limited attempts to prevent vital dyes from making direct contact with the MH and the underlying RPE.8,9
To our knowledge, few recent studies have investigated how to create a nonstained (potentially nontoxic) ILM flap that covers the MH when the inverted flap technique is used. This study evaluated a modified technique using triamcinolone acetonide and ICG sequentially during PPV to create a nonstained ILM flap that covers a large idiopathic MH.
Methods
This study was approved by the Institutional Review Board, Zhongshan Ophthalmic Center of Sun Yat-sen University (#2022KYPJ021), and was performed in accordance with the Declaration of Helsinki. Consecutive eligible patients were prospectively included. All participants provided written informed consent.
Patients who had been diagnosed with an idiopathic MH with a minimum linear diameter greater than 400 μm were included in the study. Patients who had been diagnosed with concomitant retinopathies or maculopathies, who had previous vitreoretinal surgeries, or who had an axial length (AL) greater than 26.5 mm were excluded from the study.
Data on age, sex, best-corrected VA (BCVA), and intraocular pressure (IOP) were collected for all patients. Snellen VA was converted to logMAR notation for statistical analysis.
Surgical Technique
All surgeries were performed by the same experienced surgeon (Z.Z.). In all cases, 25-gauge PPV was performed with a valved trocar–cannula. Endoillumination was adjusted to less than 35% to reduce the phototoxicity and photoactivation of the ICG. A core vitrectomy was performed, followed by induction of a posterior vitreous detachment (if absent) with the aid of triamcinolone acetonide (40 mg/mL). After the central vitreous was shaved off and no vitreous or epiretinal tissue remained around the MH (Figure 1A), a droplet of triamcinolone acetonide (40 mg/mL) was injected onto the MH and its surrounding area (diameter of approximately 2 optic discs) (Figure 1B), preventing direct contact with the ICG. The valved trocar–cannula is essential at this step because it prevents the droplet of triamcinolone acetonide from being washed away from the posterior pole as a result of the turbulence created by the infusion of balanced saline solution.
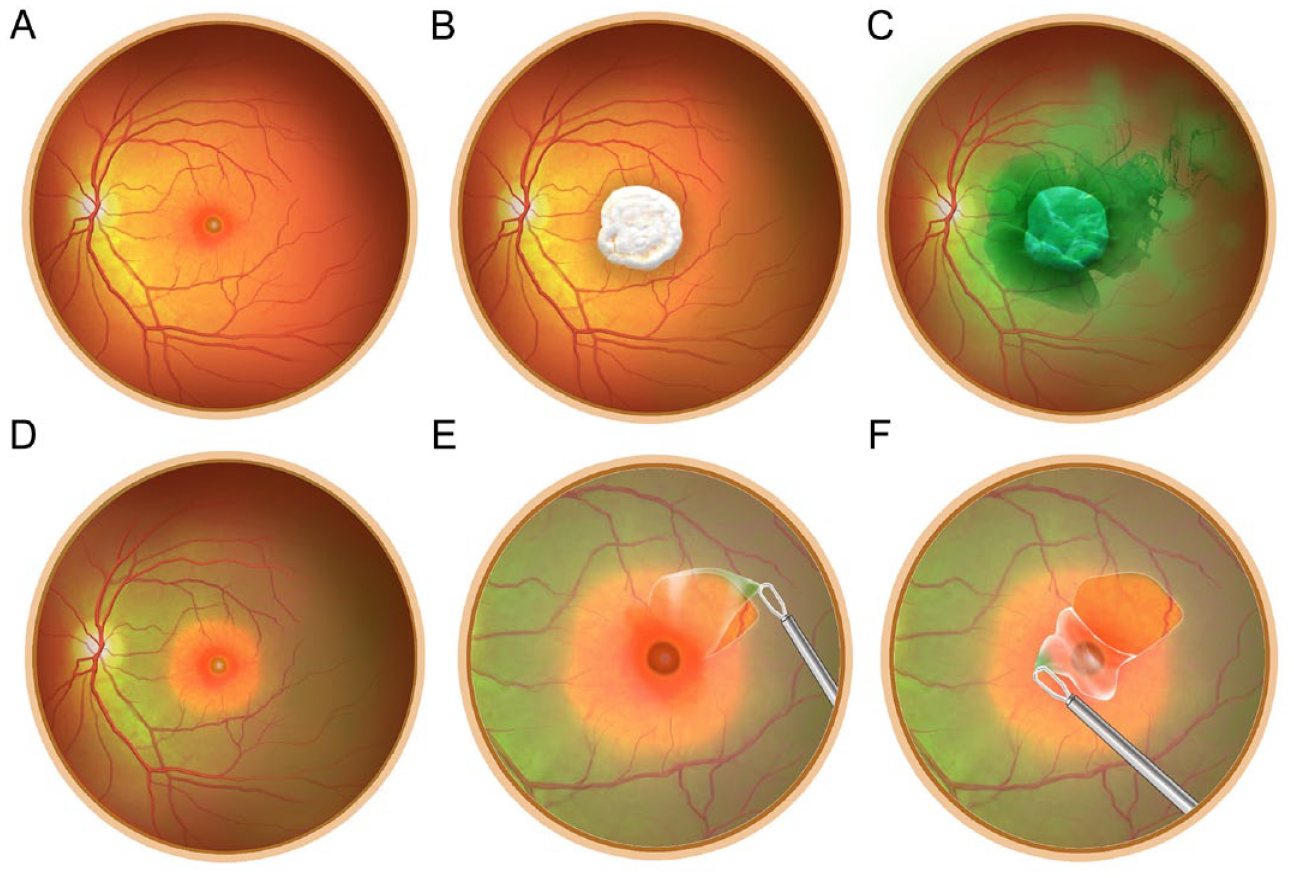
Key steps of the Yin-Yang ILM staining technique. (A) After the posterior vitreous and central vitreous are removed, the vitreous cavity is filled with balanced saline solution. (B) A droplet of triamcinolone acetonide is injected onto the posterior pole to cover the MH and its surrounding area. (C) Dextrose-diluted ICG is injected around the triamcinolone acetonide–covered area for ILM staining. (D) After sequential clearance of the ICG and triamcinolone acetonide, the area covered by the triamcinolone acetonide droplet is not stained by the ICG, while the peripheral area of ILM is well stained. (E) A pinch-peel technique is used to create an ILM flap from the stained area. (F) The wide-base flap is inverted with an intraocular forceps to cover the MH with its nonstained central part.
The ICG was then diluted to 2.5 mg/mL, and 5% dextrose was administered to the area around the triamcinolone acetonide droplet (Figure 1C). The specific gravity of the ICG solution was greater than that of the balanced saline solution, preventing it from floating over the vitreous cavity. Next, a flute needle was used to aspirate the ICG first and then to aspirate the triamcinolone acetonide. A vitrectomy probe was then used to aspirate the residual triamcinolone acetonide and ICG in the vitreous cavity. After the triamcinolone acetonide and ICG were cleared, the staining of the area surrounding the MH was well visualized (Figure 1D).
An ILM flap was created using a pinch-and-peel technique with an end-grasping forceps from the temporal stained region (Figure 1E). The ILM flap was then inverted to cover the MH (Figure 1F). The stained edge of the ILM flap was trimmed off using a vitrectomy probe, leaving the wide base of the ILM flap anchored at the temporal border of the MH. The other portion of the ILM was further peeled off from the stained region. After it was confirmed that the inverted ILM flap was covering the hole, fluid–air exchange and long-acting gas (12% perfluoropropane) were used to complete the surgery. The Supplemental Video shows the modified technique. Postoperatively, all patients were required to remain in a face-down position for at least 12 hours a day for 2 weeks.
If a regular and continuous hyperreflective line corresponding to the external limiting membrane (ELM) or ellipsoid zone (EZ) was seen on the postoperative optical coherence tomography (OCT), the layers of the MH were considered intact. MH closure after surgery was defined by the integrity of the retinal layer in the macular area without bare RPE seen on OCT. (Flat-open and elevated-open closure types were not considered successful hole closures.)
Imaging
OCT scans were performed before the MH repair and postoperatively at 1 month, 3 months, and 6 months. The minimum linear diameter and base diameter of the MHs were measured before surgery but did not account for AL. The foveal configuration and integrity of the outer retinal layers, including the ELM and the EZ, were assessed at each postoperative follow-up visit.
Statistical Analysis
All tests in this study were 2-sided, with statistical significance set at P ≤ .05. Statistical analysis was performed using Prism software (version 9.5, GraphPad). Mean values are ± SD.
Results
The study included 24 women (77.4%) and 7 men (22.6%) with a mean age of 59.6 ± 6.6 years (range, 47-71). The mean preoperative logMAR BCVA was 1.06 ± 0.30 (Snellen range, 20/60-20/600−).
At the 1-month follow-up, the mean logMAR BCVA had improved to 0.84 ± 0.33 (Snellen range, 20/30-20/500), which was statistically significantly better than preoperatively (P < .001). The mean logMAR BCVA at the 3-month follow-up was 0.66 ± 0.32 (Snellen range, 20/25-20/400), which was statistically significantly better than at the 1-month follow-up (P < .001). At the 6-month follow-up, the mean logMAR BCVA was 0.56 ± 0.31, a significant improvement from the BCVA at the 3-month follow-up (P = .002).
Twenty-eight eyes (90.3%) had achieved primary MH closure by the 1-month follow-up. No reopening of the MH was observed at the 6-month follow-up. In addition, no obvious changes in the RPE were observed in any case. Twelve eyes (38.7%) had a U-shaped macular contour, and 9 eyes (29.0%) had a V-shaped macular contour at the 6-month follow-up. In the 3 cases (9.7%) in which the hole failed to close by the 1-month follow-up, the MH remained flat-open at the 6-month follow-up; no secondary surgery was performed. The mean minimum linear diameter of the MHs was 593 ± 119 μm (range, 406-818) and of the base diameter, 1082 ± 242 μm (range, 631-1601).
Except for a transient IOP elevation after surgery, no obvious intraoperative or postoperative complications were observed. At the 1-month follow-up, the ILM flap over the foveal area was visible in 26 eyes (83.9%) (Figure 2). Figure 3 shows the integrity of the outer retina, specifically the ELM and the EZ, at the follow-up visits.
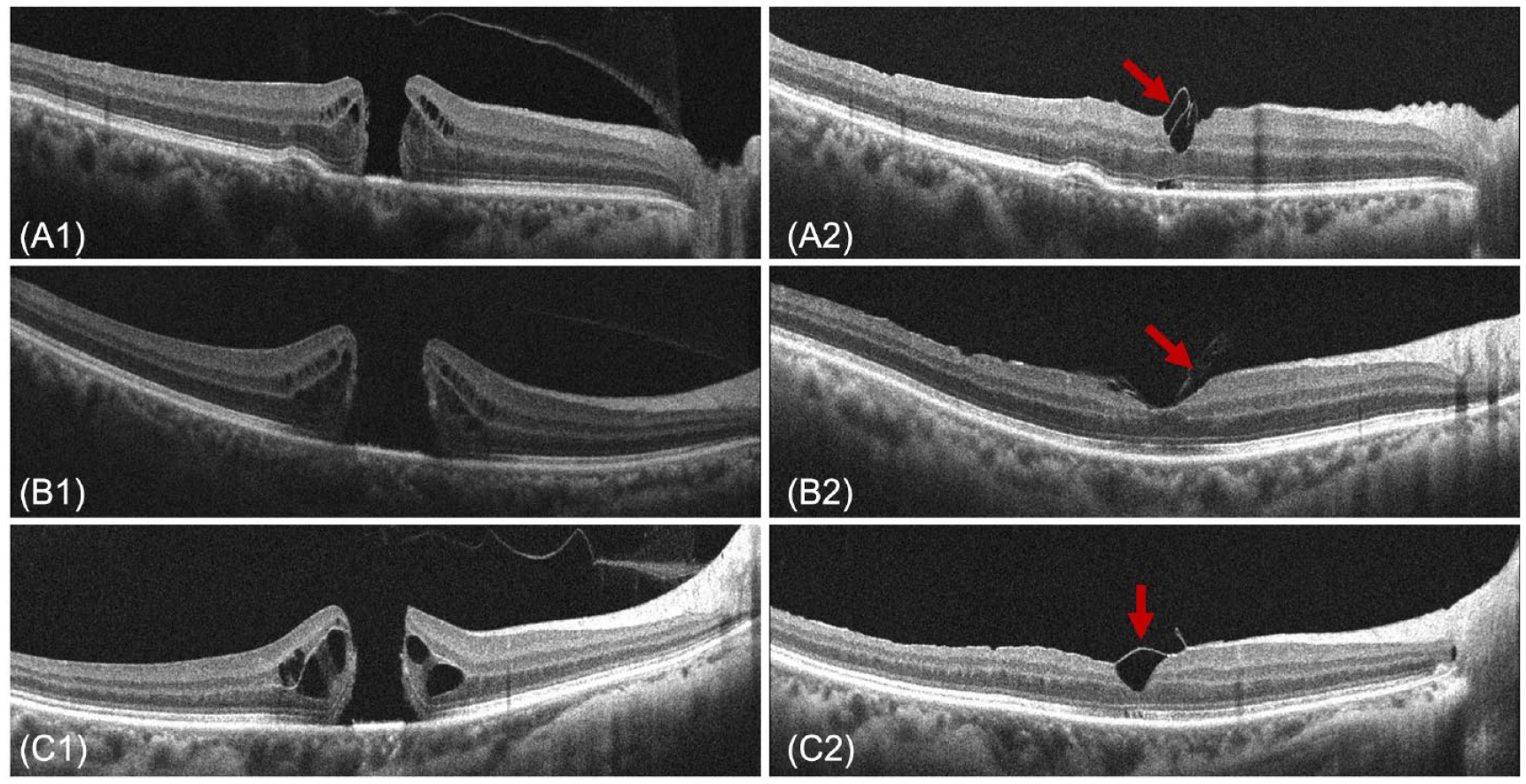
Preoperative optical coherence tomography images and different stages of the ILM flaps, macular contour, and integrity of the outer retina 1 month postoperatively. (A1 and A2) The MH has regained a V-shaped closure, the ILM flap does not completely cover the foveal area (red arrow), and the ELM is intact; however, the EZ still shows slight discontinuity. (B1 and B2) The MH has regained a U-shaped closure, the ILM flap is visible (red arrow), and the outer retina has almost realigned. (C1 and C2) The MH has regained a V-shaped closure, the ILM flap completely covers the foveal area (red arrow), and the outer retina has almost realigned.
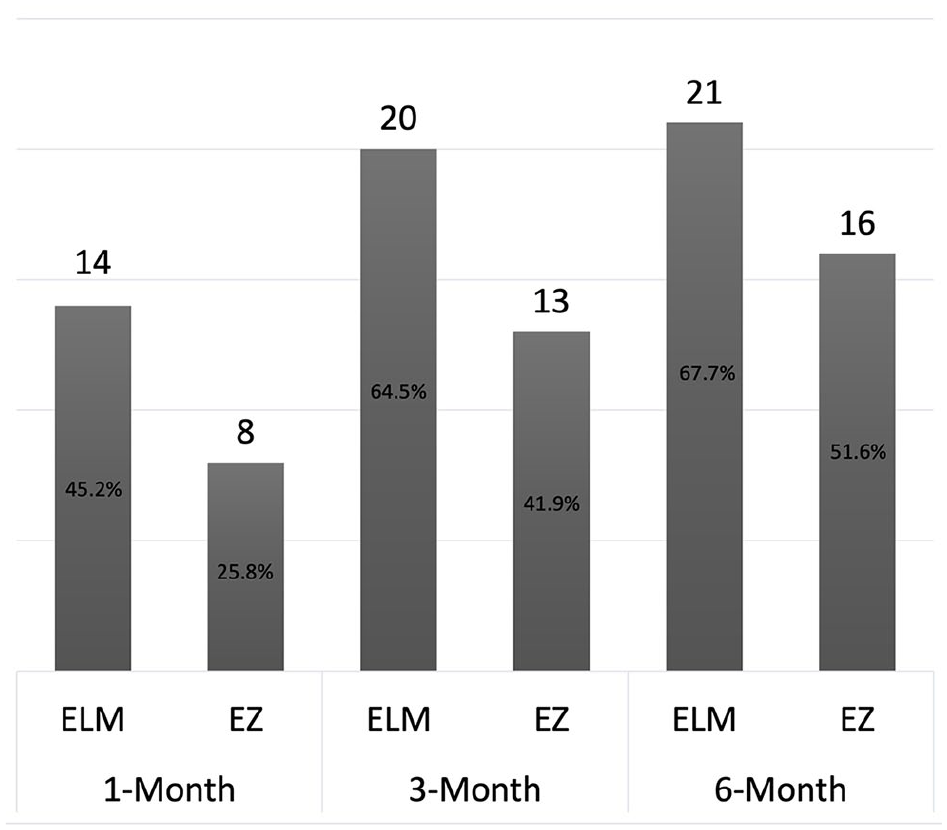
Number and percentage of patients with realignment of the external limiting membrane (ELM) and ellipsoid zone (EZ) 1 month, 3 months, and 6 months postoperatively.
Conclusions
This study introduced a modified technique that involves using triamcinolone acetonide and dextrose-diluted ICG sequentially for Yin-Yang (negative-positive) ILM staining to create a nonstained flap to cover MHs with a minimum linear diameter greater than 400 μm. The MH closure rate was 90.3%, with a significant improvement in VA at all postoperative follow-up visits. This outcome is better than that in previous reports.5,10 –12
During surgery, the Yin-Yang staining technique effectively prevented the MH and its surrounding area from coming into direct contact with the ICG. However, the stained area was well visualized by the surgeon for initiating the pinching and peeling steps. No slippage of the ILM flap was observed in any case.
One month after surgery, the effective coverage of the ILM flap could still be seen on OCT in most patients (26 of 31). The large base of the ILM flap played a crucial role in achieving this positive outcome. 12 The current technique uses a valved trocar–cannula, resulting in a slower trocar flow rate than when an open, nonvalved trocar–cannula is used. The slower flow rate likely prevented the droplet of triamcinolone acetonide from being washed away by the turbulence created by infusion of the balanced saline solution.
Another essential step of this technique is dilution of the ICG with 5% dextrose, which has 2 advantages. First, the ICG solution, which has a higher specific gravity than the balanced saline solution, remains on the posterior pole and is easily aspirated by the flute needle. Second, the ICG solution is closer to being iso-osmolar, potentially making it safer in terms of toxicity to the retina. 13
Considering the possibility of retinal toxicity caused by ICG, attempts have been made to provide better protection of the photoreceptor layer and RPE layer. Although experimental and clinical studies found that brilliant blue G is safer than other vital dyes, cases of toxicity have been reported in the literature. Another problem is that brilliant blue G may not be readily available in certain regions and institutions. In contrast, ICG is still widely used by many surgeons, as indicated in recent publications.
Despite efforts to mitigate toxicity, current ILM staining techniques share a common problem; that is, the MH is inevitably exposed to vital dyes. Modified techniques, such as injecting perfluorocarbon liquid and using autologous whole blood, have been proposed to create a mechanical barrier and prevent the ICG from coming into direct contact with the MH.8,9,13 However, a few recent reports describe modifications of ILM staining methods. To our knowledge, no randomized clinical trial has compared the anatomic and functional outcomes between stained ILM techniques and nonstained ILM techniques when the inverted ILM flap is used to cover the MH. Because ILM techniques have been successfully used to treat large and complex MHs, exploring how to harvest a nonstained (potentially toxic-free) ILM flap would be a useful and interesting topic for further exploration.
In recent years, it has been noted that inserting the ILM into the MH can prevent realignment of the outer retina and hinder visual recovery.10,11 Therefore, the current study used the nonstained ILM flap to cover the MH. Although the exact mechanism is not well understood, it is speculated that creating a small, closed space over the MH allows for better restoration of the ELM and EZ. In our study, the postoperative outer retina realignment and macular contour were good, which may be attributed to several factors. The ILM flap had a wide base anchored on the margin of the MH, preventing slippage; the flap did not come into direct contact with the ICG, making it potentially more elastic; and no residual ICG was carried by the flap, reducing the risk for toxicity to the retina.
The current study has several limitations. It was not a randomized controlled trial, and the sample was not sufficiently large. Other types of vital dyes were not available to us; therefore, only ICG was used to evaluate the staining technique. The current method used a large amount of triamcinolone acetonide to cover the MHs, and its potential toxicity might lead to RPE changes, which could be a potential drawback. Another concern with the current technique is the lack of published reports regarding stained ILM flaps carrying toxicity to the retina or RPE. Microperimetry was not performed because our department does not have the necessary equipment. Further studies with control groups and larger samples will be able to provide a more in-depth investigation of this technique.
In conclusion, the Yin-Yang ILM staining technique using triamcinolone acetonide and ICG sequentially is safe and effective for creating a nonstained ILM flap that covers the MH. Despite the potential toxicity of ICG, the current technique may be an ideal option for MH closure.
Footnotes
Authors’ Note
Drs. Ni and Xing contributed equally to this work.
Ethical Approval
The study protocol was reviewed and approved by the Institutional Review Board, Zhongshan Ophthalmic Center of Sun Yat-sen University (#2022KYPJ021), and conformed to the tenets of the Declaration of Helsinki.
Statement of Informed Consent
All patients provided written informed consent, including permission for publication of all photographs and images included herein.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.