
Abstract
Introduction
Cytomegalovirus (CMV) is a ubiquitous virus of the family Herpesviridae, which can cause various ocular diseases, including anterior uveitis, corneal endotheliitis, and retinitis.1,2 Although CMV anterior uveitis most commonly affects immunocompetent patients, CMV retinitis is typically observed in immunosuppressed individuals.1–3
The majority of CMV retinitis occurs in patients who are unable to mount an adequate T-cell–mediated response against the pathogen, including patients with acquired immunodeficiency syndrome (AIDS), organ and bone marrow transplant recipients, and individuals receiving chemotherapy for a malignancy. In addition, CMV retinitis has been reported in patients with a relative immunocompromised state, such as diabetes mellitus (DM).1,4,5 Furthermore, several reports have found infections in immunocompetent individuals treated with intravitreal (IVT) steroids, suggesting a causative mechanism of local immunosuppression.6–8 However, to our knowledge only 2 cases of polymerase chain reaction (PCR)–positive CMV retinitis in adults have been published in the setting of immunocompetence without local immunosuppression.6,9 The details are limited because in 1 report, the patient was part of a case series in which information was grouped together. 6
Here, we describe a case of PCR-positive CMV retinitis in an immunocompetent patient without local immunosuppression who was followed for 3 years. Informed consent was not required for this case report because it contains no personal identifying information.
Case Report
A 47-year-old woman presented with a new-onset paracentral scotoma in the left eye. Visual acuity (VA) was 20/20 OD and 20/20 eccentrically OS. The intraocular pressure (IOP) was 15 mm Hg OD and 30 mm Hg OS. Examination of the right eye was unremarkable; the left eye had diffuse fine keratic precipitates with 2+ anterior chamber cells and 1+ anterior vitreous cells and haze. Dilated examination showed a focal area of retinal whitening temporal to the fovea with no other lesions in the periphery (Figure 1A). Fundus autofluorescence showed abnormal hyperautofluorescence of the lesion (Figure 1B), while fluorescein angiography showed increased hyperfluorescence of the lesion (Figure 1C) with localized angiographic macular edema. Optical coherence tomography (OCT) showed increased inner retinal hyperreflective changes with associated outer retinal attenuation just temporal to the fovea (Figure 2).
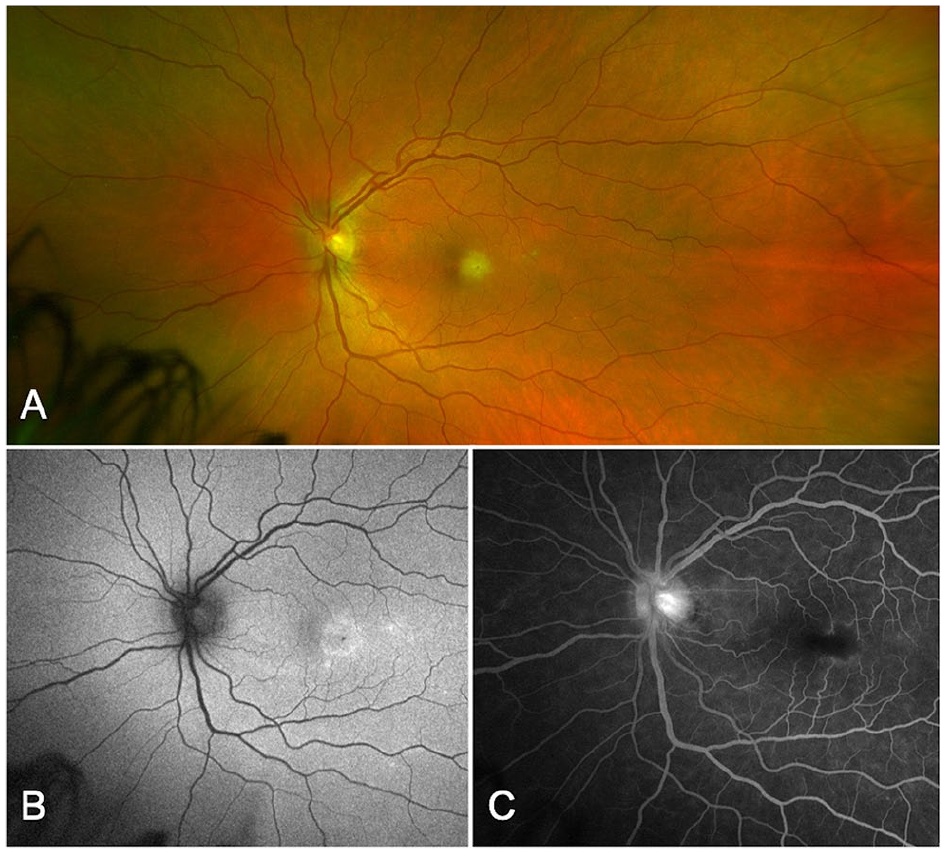
(A) Fundus photograph of the left eye shows foveal retinitis. (B) Fundus autofluorescence of the left eye shows increased hyperautofluorescence temporal to the fovea. (C) Late-stage fluorescein angiography shows hypofluorescence of the lesion with localized angiographic macular edema.
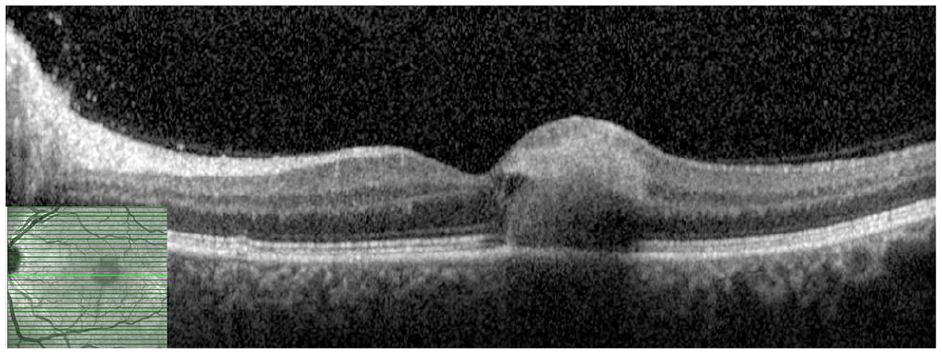
Optical coherence tomography of the left eye at initial presentation shows inner retinal hyperreflective changes with outer retinal attenuation just temporal to the fovea.
The patient denied previous medical, oncologic, ocular, or surgical history. She was followed annually by her primary care physician; routine bloodwork (comprehensive metabolic panel, blood counts, cholesterol levels) was unremarkable. She had recently traveled to North Carolina but denied significant outdoor exposure, bug bites, or consumption of contaminated or undercooked food and water. She had no recent illnesses or use of steroids by any route, and a review of systems was unremarkable other than a resolving erythematous papule on the left wrist.
An anterior chamber paracentesis was performed given the concern for infectious retinitis. The results showed a positive quantitative CMV PCR, while herpes simplex virus (HSV) 1 and 2, varicella zoster, and toxoplasmosis PCRs were negative. Additional serologies obtained were broadly negative, including antineutrophil antibodies, anti-dsDNA, lupus anticoagulant antibodies, antineutrophil cytoplasmic antibodies, rheumatoid factor, anticyclic citrullinated peptides, angiotensin-converting enzyme, lysozyme, serum interleukin-2 receptor, syphilis antibodies, QuantiFERON Gold, and HIV. No underlying abnormalities were found on a pan-computed tomography scan of the chest, abdomen, and pelvis.
Treatment was initiated with oral valganciclovir 900 mg twice daily as well as adjuvant IVT ganciclovir (2 mg) and foscarnet (1.2 mg) injections twice weekly for 3 weeks. The patient was also treated with topical prednisolone acetate and IOP-lowering drops. She was followed closely by an infectious disease specialist over the course of her treatment. At 3 months, the retinitis was inactive with resolution of the intraocular inflammation. At 1 year, a shared decision with the infectious disease specialist was made to stop the valganciclovir. OCT images at 1 year and 2 years showed cavitary loss of the neurosensory retina at the location of the lesion (Figure 3, A and B). There was no reactivation of the disease while the patient was off valganciclovir. At her 3-year follow-up, no disease activity was seen and she remained stable without therapy. In addition, she did not develop evidence of systemic illness leading to an immunocompromised state, malignancy, or other traditional risk factors for CMV retinitis.
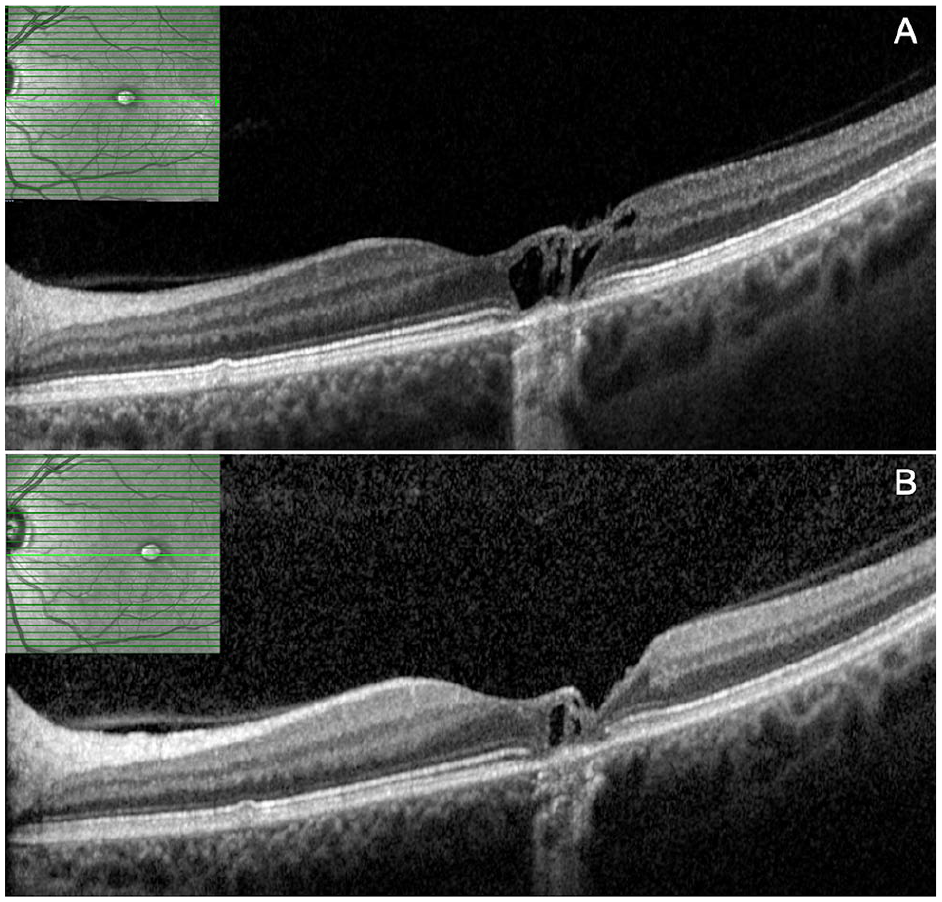
(A) One year after presentation, optical coherence tomography shows macular atrophy with a large cystic cavity. (B) Two years after presentation, there is further consolidation of the cavity.
CMV titers would have helped understand the burden of systemic involvement; however, the patient had no systemic symptoms. CMV serologic testing was not pursued by the infectious disease specialist because at the time of the patient’s initial consultation, she had been on medications for approximately 2 months.
Conclusions
This case describes the long-term follow-up of an immunocompetent patient with CMV retinitis. After approximately 3 years of follow-up, good health had been maintained with no development of any underlying cancer or immunosuppressive disease. CMV retinitis is most commonly associated with HIV, in patients with CD4+ T-cell counts less than 50 cells/µL. With the advent of highly active antiretroviral therapy, the incidence of HIV-associated CMV retinitis has decreased. It is now commonly seen in patients who have had solid organ or allogeneic bone marrow transplantation or who are receiving systemic immunosuppression. 1 These patients may experience reactivation of CMV after medical immunosuppression for their transplants.
There are several cases reported of CMV retinitis in the absence of systemic immunosuppression; however, the patients were receiving local (ocular) corticosteroids.6–8 CMV retinitis can masquerade as a noninfectious panuveitis, which may not be recognized until there is significant clinical worsening with local corticosteroids. 10 It is also possible that in certain cases, localized immune suppression from periocular or IVT steroids may lead to reactivation of CMV. Thus, clinicians must be diligent to include an infectious etiology on the differential when the clinical examination worsens with local corticosteroids.
CMV retinitis can occur in seemingly healthy patients with no evidence of systemic or local immunosuppression,4,9,11,12 including a 67-year-old man who developed CMV retinitis after complicated cataract surgery. 4 However, the patient had a history of DM type 2 complicated by bilateral proliferative diabetic retinopathy as well as treatment with topical corticosteroids after cataract surgery. Thus, there may be confounding in this case, given the diabetic-induced relative immunosuppression and the topical corticosteroids, which could allow for reactivation of the virus.
Another case report describes a 68-year-old immunocompetent woman with no known predisposing factors who developed bilateral CMV retinitis. 9 She first presented with diffuse retinitis in the right eye. A workup and anterior chamber tap revealed PCR-positive CMV. She was treated with valganciclovir but ultimately developed a rhegmatogenous retinal detachment. She was lost to follow-up and presented again 2 years later with extensive retinitis in the left eye. The aqueous fluid was again PCR-positive for CMV. The patient had an extensive serologic workup that was unremarkable. She was treated with intravenous ganciclovir for 2 weeks and twice-weekly IVT ganciclovir injections for 1 week. She was transitioned to 900 mg daily oral valganciclovir for 6 months, then had a recurrence of retinitis while off the valganciclovir. The patient ultimately had an improvement in VA to 20/100 in the left eye while remaining on maintenance therapy of 900 mg valganciclovir. 9
CMV typically causes retinitis in immunocompromised individuals. Briefly, CMV is a ubiquitous virus that, after the primary infection, lies dormant in CD 34+ myeloid progenitor cells and is effectively shielded from the immune system. 1 These infected myeloid progenitor cells differentiate into circulating macrophages and dendritic cells. On activation of the immune system in the setting of routine infections, the virus can reactivate and begin production in various epithelial surfaces of the body. The virus is neutralized by various T-cell–mediated inflammatory pathways in patients with intact immune systems. 1 In patients who lack a robust CD4+ and CD8+ T-cell response, however, reactivation of CMV can lead to end organ complications. In rare circumstances of individuals with normal immune statuses, local immunosuppression (ie, steroid use) can lead to a decreased T-cell response, which may allow CMV to proliferate.
To our knowledge, our patient was healthy with no previous history of medical illness. She denied any surgical intervention and had no history of systemic or local corticosteroid therapy. An initial extensive serologic evaluation as well as an evaluation by an infectious disease specialist and pan CT scan of the chest, abdomen, and pelvis showed no underlying abnormalities. At the 3-year follow-up, the patient had no new medical illness. In such cases, it may be reasonable to consider lifelong prophylaxis with valganciclovir or monitoring the patient off therapy in the event that he or she is cured of a transient opportunistic infection. Given the significant adverse effects of valganciclovir (ie, myelosuppression), we decided (along with the patient and infectious disease specialist) to trial observation off therapy while keeping in mind that any recurrence may necessitate lifelong therapy.
In conclusion, we present the long-term follow-up of an immunocompetent patient without known risk factors for immunosuppression who developed acute CMV retinitis. In patients with retinitis, the diagnostic use of aqueous PCR is critical, especially in cases of atypical presentations that may be CMV.
Footnotes
Ethical Approval
Ethical approval was not required for this case report.
Statement of Informed Consent
Informed consent was not sought for this case report because it contains no personal identifying information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.