
Abstract
Keywords
Introduction
The intravitreal (IVT) sustained-release dexamethasone implant (Ozurdex, Allergan) has been used for the past several years as an effective treatment for diabetic macular edema (DME), macular edema (ME) secondary to retinal vein occlusion (RVO), and intraocular inflammation associated with noninfectious posterior uveitis.1–3 Endophthalmitis is a dreaded, rare complication of IVT injections and can result in permanent vision loss. IVT steroid injections may confer an increased risk for endophthalmitis compared with antivascular endothelial growth factor (anti-VEGF) injections, with 1 study reporting an almost 7-fold increased risk, possibly related to larger wound tracts from the needles used for steroid injections and a local immunosuppressive effect. 4 Large studies have reported endophthalmitis rates between 0.10% and 0.14% after dexamethasone injections.5,6
Given its rarity, there are limited case reports documenting endophthalmitis after dexamethasone implantation, with most patients presenting early after the injection, between 2 and 12 days.7–12 A recent series included 3 patients with atypical symptoms of painless vision loss with mild to no conjunctival injection at 7 days, 18 days, and 35 days after the injection; 2 of these 3 cases were managed conservatively with topical steroid and antibiotic therapy alone. 13 None of the cases was confirmed with positive cultures, and the authors postulated that these cases may have represented noninfectious intraocular inflammations.
No guidelines regarding the management of endophthalmitis after dexamethasone implantation have been clearly established, with cases documenting clinical improvement after IVT antibiotic injection, pars plana vitrectomy (PPV), and removal of the dexamethasone pellet.6,9,10 The purpose of this series is to highlight the clinical features and management of unusually delayed-onset acute infectious endophthalmitis after dexamethasone injection.
Methods
The Institutional Review Board, West Virginia University, approved this retrospective case series. The research adhered to the tenets of the Declaration of Helsinki and was conducted in an ethically responsible manner. Informed consent was not sought for the current study given its retrospective nature and lack of identifying information. A retrospective chart review was performed of cases of endophthalmitis after administration of an IVT dexamethasone implant between January 2019 and June 2024.
Patients were evaluated and managed in the emergency department, inpatient unit, and/or our outpatient clinic under the care of 1 of 2 retina specialists (N.P., G.G.). Two of 3 cases had a dexamethasone injection at an outside facility, and details of the injection technique are unknown. The case that had a dexamethasone injection at West Virginia University received antisepsis with 5% povidone–iodine solution; 10% povidone–iodine was used to swab the eyelids, lashes, and fornices before injection. For topical anesthesia, proparacaine hydrochloride 0.5% ophthalmic solution and lidocaine 3.5% gel were administered. Injections were performed with nonsterile gloves and an eyelid speculum. No antibiotic drops were given before or after the procedure. The dexamethasone applicator was inserted 3.5 mm posterior to the limbus inferotemporally and injected in a beveled fashion, initially advancing parallel to the limbus before redirecting perpendicular to the sclera to inject the dexamethasone pellet.
After the diagnosis of acute endophthalmitis, an aqueous or vitreous tap was performed and sent for Gram stain analysis. Aerobic, anaerobic, and fungal cultures were also taken.
Results
Case 1
A 72-year-old man with a history of branch RVO in the right eye and cystoid ME only partially responsive to anti-VEGF IVT injections had an IVT dexamethasone injection at West Virginia University Eye Institute. The patient’s baseline best-corrected visual acuity (BCVA) was 20/60. Twelve days later, he presented with reports of redness, discomfort, and reduced vision for 5 days. The BCVA was 20/100 with examination findings notable for localized temporal injection. There was no evidence of anterior chamber or vitreous cells. The dexamethasone implant was visualized inferiorly in the vitreous cavity. He was diagnosed with episcleritis and recommended to initiate artificial tears and oral ibuprofen.
Four days later (16 days postinjection), the patient returned with a 1-day duration of rapid vision loss and worsening pain. The visual acuity (VA) was hand motions (HM). An examination now revealed 3+ conjunctival injection, chemosis, 4+ anterior chamber cells, fibrinous membrane overlying the pupil, and a hypopyon. There was no view posteriorly. An anterior chamber tap was performed and sent for culture. IVT vancomycin (1.0 mg), ceftazidime (2.0 mg), and voriconazole (100 µg) were administered. Treatment was initiated with topical moxifloxacin 0.5% 4 times a day, prednisolone acetate 1% 4 times a day, and cyclopentolate 1% 3 times a day.
The next day, the patient’s vision and examination were unchanged. Two days later, his pain had resolved, yet his VA was still HM. An examination was notable for a trace, resolving hypopyon, anterior chamber fibrin, and dense vitritis. The decision was made to proceed with a 25-gauge PPV with anterior chamber washout. Intraoperatively, retinal hemorrhages, whitening throughout the posterior pole, and subretinal infiltrates were noted. The dexamethasone implant could not be visualized. A vitreous sample was sent for microbiologic analysis, and IVT vancomycin (1.0 mg), ceftazidime (2.0 mg), voriconazole (100 µg), and dexamethasone (400 µg) were administered. Postoperatively, both the anterior chamber and vitreous cultures returned positive for Staphylococcus aureus.
One week postoperatively, the patient’s VA improved to counting fingers (CF) at 5 feet. There was marked improvement in the anterior chamber and vitreous inflammation; however, an inferior macula-involving retinal detachment was noted. Therefore, a 25-gauge PPV was again performed with endolaser application and a silicone oil (SO) tamponade. Postoperatively, the retina remained attached. After SO removal 3 months later, the BCVA returned to 20/100. The patient’s ME has since been managed with aflibercept injections alone without additional administrations of dexamethasone.
Case 2
A 68-year-old man with ME secondary to severe nonproliferative diabetic retinopathy received an IVT dexamethasone implant in the left eye from an outside retina specialist. Exactly 5 weeks later, he presented to the emergency department with 2 days of progressive, painless vision loss in the left eye. The patient’s VA was reduced from 20/70 before dexamethasone implantation to CF at face. An examination was notable for noninjected conjunctiva, a 2.0 mm hypopyon, and 4+ anterior chamber cells, with dense vitritis obscuring the view of the posterior pole (Figure 1). An anterior chamber tap was performed and sent for culture. IVT injections of vancomycin (1.0 mg), ceftazidime (2.0 mg), and voriconazole (100 µg) were administered. Treatment was started with topical moxifloxacin 0.5% 4 times a day, prednisolone acetate 1% every 2 hours, and cyclopentolate 1% 3 times a day.
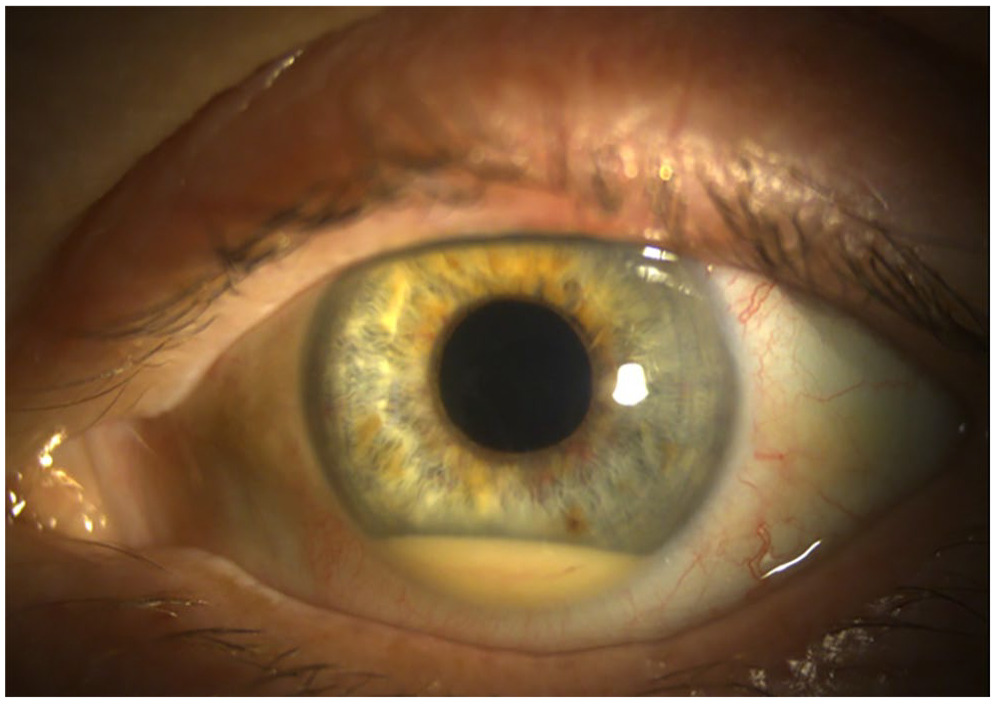
Slit lamp photograph of the left eye of Case 2 5 weeks after injection of an intravitreal dexamethasone implant shows unusually mild injection and a 2.0 mm hypopyon with mixed white and red blood cells.
The next day, the patient’s vision and examination were unchanged. The following day, the VA and examination were stable except for new anterior chamber fibrinous material. An injection of IVT dexamethasone (400 µg) was administered. A vitrectomy was performed the next day, during which the patient had a vitreous biopsy, anterior chamber washout, and IVT injection of vancomycin (1.0 mg), ceftazidime (2.0 mg), voriconazole (100 µg), and dexamethasone (400 µg). The dexamethasone implant could not be identified in the vitreous cavity.
On postoperative day (POD) 1, the patient’s VA had improved to 20/100 with 2+ anterior chamber cells, resolved hypopyon, and mild residual vitreous debris. By POD 5, the VA improved further to 20/60. The initial aqueous tap yielded no isolate. One of the 2 vitreous fluid cultures collected from the vitrectomy sample yielded no isolate, while the other returned positive for rare Staphylococcus epidermidis. The patient subsequently returned to the care of his local ophthalmologist.
Case 3
A 67-year-old woman with a history of ME secondary to posterior uveitis received an IVT dexamethasone implant in both eyes from an outside ophthalmologist. She then presented to our emergency department 18 days later with a 1-day duration of reduced vision and pain in the right eye.
The VA was HM only, with examination findings of 1+ injection and 4+ cells with a fibrinous plaque overlying the pupil and no view posteriorly. B-scan ultrasonography showed vitritis. Given that the patient’s examination findings were consistent with acute endophthalmitis, a vitreous tap was performed along with IVT injections of vancomycin (1.0 mg), ceftazidime (2.0 mg), voriconazole (100 µg), and dexamethasone (400 µg). The patient was admitted to the hospital for monitoring as a result of transportation issues. Treatment was initiated with moxifloxacin 0.5% 4 times a day, prednisolone acetate 1% every 2 hours, and cyclopentolate 1% 3 times a day.
The patient was evaluated the next day with unchanged vision and a stable examination except for a newly formed 1.0 mm hypopyon. The decision was made to proceed with a PPV (Figure 2). A vitreous biopsy for repeat cultures was performed along with IVT injections of vancomycin (1.0 mg), ceftazidime (2.0 mg), voriconazole (100 µg), and dexamethasone (400 µg). The dexamethasone implant was not removed at the time of surgery.
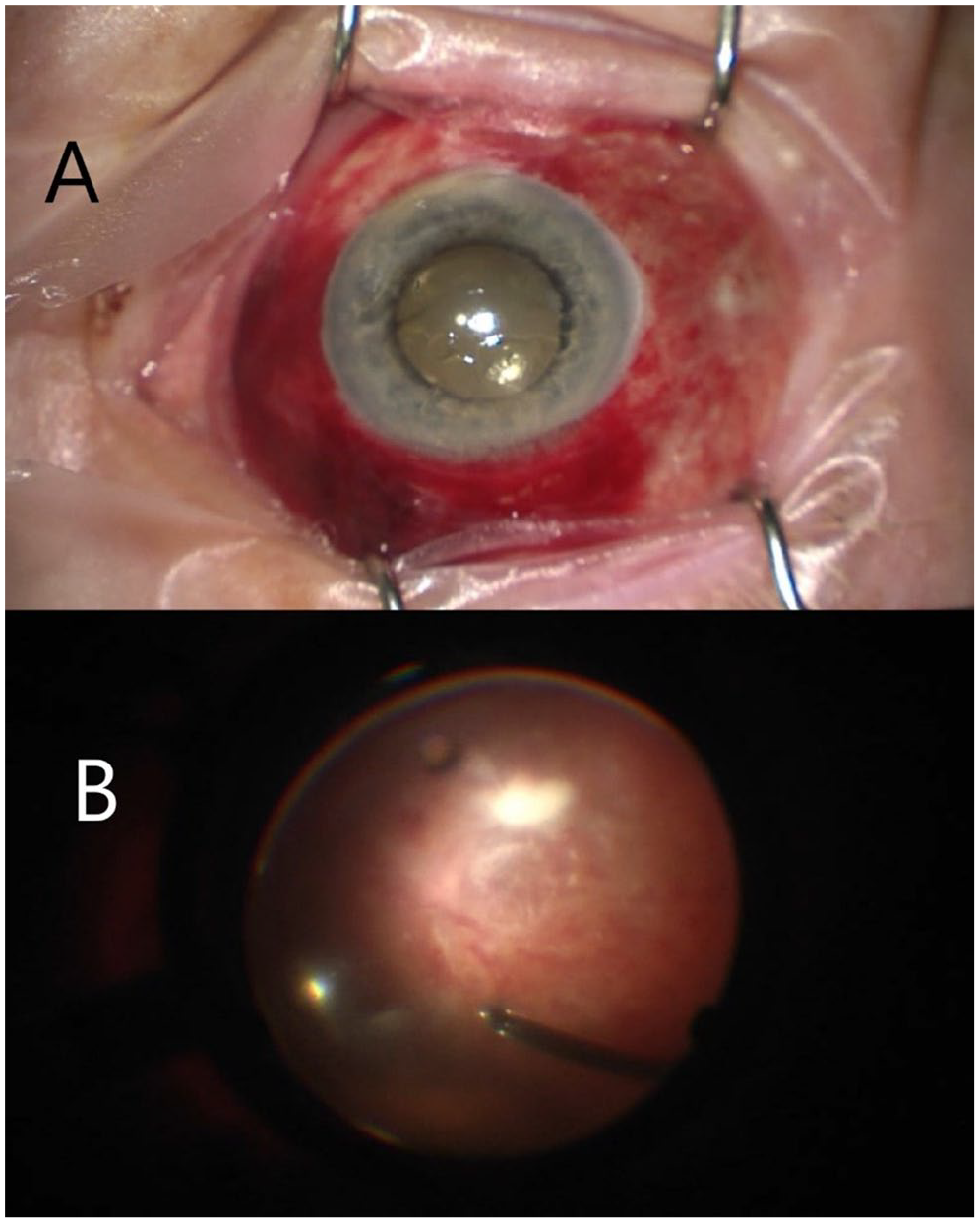
(A) External view of the right eye of Case 3 under operating microscope visualization shows diffuse subconjunctival hemorrhage and injection, corneal edema, and a small inferior hypopyon. (B) Intraoperative view of the vitreous cavity during pars plana vitrectomy shows diffuse hemorrhages scattered across the posterior pole with a fluffy white retinal infiltrate inferior to the inferotemporal arcade.
On POD 1, the patient’s VA remained HM with corneal edema, improving anterior chamber inflammation, and a hazy but improved view of the posterior pole showing macular hemorrhages and white infiltrates. The culture from her initial vitreous tap ultimately was positive for Granulicatella adiacens. She was discharged home and elected to follow up with an outside ophthalmologist for further care. Further documentation of her follow-up is limited; however, she was examined at postoperative week 2 and her VA had improved to CF at 2 feet in the right eye with no residual inflammation.
Conclusions
Endophthalmitis after administration of the IVT sustained-release dexamethasone implant is a rare, yet devastating complication, with some data suggesting its incidence may be higher than endophthalmitis after anti-VEGF injection.4,5 Physicians should be mindful of this when electing to augment IVT anti-VEGF therapy with the use of the sustained-release dexamethasone implant. The applicator’s larger gauge needle acted as a conduit for intraocular bacterial penetration, postinjection wound leak, hypotony, and local immunosuppressive effects of the steroid, all contributing to endophthalmitis risk.
Although general recommendations for endophthalmitis after other procedures such as cataract surgery have been established over recent decades, there are no evidence-based guidelines regarding the appropriate management of endophthalmitis after dexamethasone injection. 14 Published cases have documented successful management with vitreous tap-and-inject (T&I) and PPV with or without removal of the dexamethasone pellet; a recent publication has documented success even with topical therapy alone, although these cases more likely represented noninfectious uveitis.12,13,15,16 All 3 of our cases were managed with an initial T&I (aqueous or vitreous) followed by PPV without pellet removal with a subsequent improvement in VA.
At present, there are no data on the benefits of immediate vitrectomy vs initial vitreous T&I; in practice, the latter is often performed first because of limitations in operating room and staff availability as well as the desire to minimize the time from infection onset to initial IVT antibiotic administration. In our practice, we frequently perform an initial T&I at the bedside on presentation, with subsequent PPV and additional IVT antibiotic administration in the early postinfection period (ie, within 1 week of presentation), as seen in the cases reported here.
Several instances of endophthalmitis after dexamethasone implantation have been documented, with presentation commonly between 2 days and 5 days, the typical window for acute postinjection endophthalmitis.7–10,15,16 However, a phenomenon of more delayed, acute endophthalmitis after dexamethasone injection has been seen. A case reported by Goel 12 described an instance of infectious endophthalmitis presenting 12 days postinjection. A recent series by Chin et al 13 also documented 3 cases of possible endophthalmitis presenting 7 days, 18 days, and 35 days after injection. Similarly, 3 patients in our series diagnosed with acute endophthalmitis presented 16 days, 18 days, and 35 days postinjection.
None of the cases in the Chin et al series 13 were culture positive, and they discuss the possibility that their cases represent a sterile endophthalmitis given their late presentation and atypical features with minimal pain or redness. Conversely, Case 1 in our series was positive for Staphylococcus aureus from both aqueous and vitreous samples collected at different times. Case 2 was positive for S epidermidis. Case 3 was positive for G adiacens, which previous case reports have shown to be a rare cause of postinjection endophthalmitis.17,18 Case 1 and Case 3 also presented with pain characteristic of infectious endophthalmitis. Those cases also had white retinal infiltrates intraoperatively or postoperatively, which would be unlikely in the setting of sterile inflammation. We believe that these are likely cases of true infectious acute endophthalmitis that presented unusually late because of the local immunosuppressive effect of the dexamethasone implant.
Notably, there have been documented cases of delayed, culture-positive endophthalmitis after anti-VEGF injection, presenting even up to 7 weeks later.19,20 In addition, a later onset of bacterial endophthalmitis after IVT triamcinolone acetonide injection has been documented (up to 2 weeks postinjection), which likewise may be affected by the immunosuppressive effect of the corticosteroid. 21
A sustained high clinical suspicion beyond the immediate postinjection period is advocated given the potential for a delayed presentation of endophthalmitis. Future studies may shed light on the efficacy of vitrectomy alone vs vitrectomy with pellet removal (which is often challenging in the immediate postinjection period before the implant has started to degrade, resulting in fragmentation). 22 Although a potential nidus for infection, if left in place after IVT antibiotic delivery, the implant may in fact prove beneficial in quieting the inflammatory response of endophthalmitis.
Footnotes
Ethical Approval
This research was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a US Health Insurance Portability and Accountability Act–compliant manner.
Statement of Informed Consent
Informed consent was not required given the retrospective nature of this case series.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.