
Abstract
Introduction
Vitreous floaters, also referred to as vitreous opacities, develop from progressive degeneration, including collapse and liquefaction of the vitreous gel (synchysis) and aggregation of the vitreous collagen fibrils (syneresis).1,2 Additionally, separation of the peripapillary fibroglial tissue during complete posterior vitreous detachment (PVD) can result in a denser, larger, and more central vitreous opacity referred to as a Weiss ring. These anatomic changes result in the perception of mobile, variably opaque vitreous opacities, which may appear curvilinear, circular, or as cloud like shapes.
Although many patients find floaters to be mild, transient, and tolerable without treatment, others report them as severely disruptive to daily activities and quality of life, which is sometimes referred to as vision-degrading myodesopsia. 3 In 1 survey, 76% of participants reported experiencing floaters, and 33% reported that the floaters caused visual impairment.2,4 Similarly, another study found a significant correlation between ultrasound-based quantification of vitreous floaters and quality of life, as measured by the National Eye Institute Visual Function Questionnaire. 5 Common effects of floaters on daily activities include difficulty with computer work and reading (particularly with light backgrounds), the need to close the affected eye to focus on visual tasks, and difficulty driving as a result of mistaking vitreous opacities for oncoming objects, pedestrians, or other vehicles. Beyond the subjective perception of bothersome vitreous opacities, 2 additional visual function parameters that may be affected are straylight and contrast sensitivity. Straylight refers to light scattering by opacities within an optical media, resulting in symptoms of hazy vision, glare with night driving, and impaired facial recognition. 6 Prior studies have demonstrated reduced contrast sensitivity and increased straylight in eyes affected by vitreous floaters.5,7 Furthermore, improvements in straylight measures, contrast sensitivity, and National Eye Institute Visual Function Questionnaire scores have been reported following vitrectomy for floaters.8,9
We recommend observation and patience for most patients with symptomatic vitreous floaters, counseling that floaters may become less bothersome with time. However, some patients do not successfully adapt to their persistent floaters. 10 These patients face a difficult choice between living with persistent, visually impairing floaters that affect their quality of life and pursuing therapeutic options, including PPV and laser vitreolysis, that are associated with potential vision-threatening complications.
This study aims to assess a noninvasive, therapeutic alternative for persistently symptomatic vitreous floaters: topical, low-dose 0.01% atropine eye drops. Anecdotal reports suggest patient satisfaction with this treatment; however, to our knowledge, no published studies have evaluated its efficacy to date. In adults, 0.01% atropine produces mild but clinically significant short-term effects on pupil size, lasting at least 24 hours after application. 11 Theoretically, the slight pupillary dilation induced by atropine could reduce the intensity of the shadows cast by floaters or potentially mask them completely. Based on a Fourier optics model of the human eye, key parameters determining the optical effect of vitreous floaters include pupil diameter, opacity size, and the distance of the opacity from the retinal plane. Smaller pupil size was found to strongly influence the reduction in relative intensity, a measure of vitreous opacity severity. 12 If a therapeutic effect is established, low-dose atropine could be a safe treatment option for symptomatic floaters.
Methods
Design
This retrospective case series was conducted at the Retina Group of Washington. Adult patients with persistent symptomatic vitreous floaters were included. Patients either had no PVD or had a history of stable PVD for at least 3 months. Exclusion criteria included acute PVD within 3 months, significant vitreoretinal pathology or media opacity limiting best-corrected visual acuity (BCVA), anatomic narrow angles (assessed by the Van Herick method), history of angle-closure glaucoma, and prior PPV.
A modified National Eye Institute Visual Function Questionnaire was administered to patients presenting with symptomatic vitreous floaters. Compounded low-dose 0.01% atropine eye drops were prescribed for once-daily application over 7 consecutive days. The same National Eye Institute Visual Function Questionnaire was sent to patients after 1 week of drop use, and they were asked to complete it a second time (Supplemental File).
The primary outcome measure was improvement in general impression and satisfaction scores following drop use, as measured by the National Eye Institute Visual Function Questionnaire. Questions assessing the primary outcome included: “How satisfied are you with the results of applying drops for troubling vitreous floaters?” and “With your experience in mind, would you continue to apply these drops for troubling vitreous floaters?” Secondary outcomes included changes in scores on specific dimensions of self-reported health status related to general health and vision, difficulties with activities and driving, behavior, and adverse effects.
Statistical Analysis
Statistical analysis was performed using the Fisher exact test or χ2 test for independent proportions and t test for independent samples. Statistical significance was set at P ≤ .05. Mean values are ± SD.
Results
Baseline Characteristics
A total of 44 patients were prescribed 0.01% atropine eye drops for daily application to 1 or both eyes, and 22 patients completed at least 7 consecutive days of use. The mean age of these 22 patients was 60 ± 9.9 years, and 9 (40.9%) were female (Table 1). The reported duration of floater symptoms was 3 to 6 months for 6 patients, 6 to 12 months for 2 patients, 1 to 2 years for 1 patient, 2 to 4 years for 4 patients, and more than 4 years for 7 patients. Eleven patients applied the drops to both eyes, 9 applied them to the right eye only, and 2 applied them to the left eye only, resulting in 20 (60.6%) of 33 right eyes receiving treatment. Iris color was brown in 8 (36.4%) of 22 patients, blue in 7 (31.8%) of 22 patients, and green/hazel in 7 (31.8%) of 22 patients. Mean logMAR BCVA was 0.0 ± 0.001 (Snellen equivalent, 20/20). Twenty-two (66.7%) of 33 eyes were phakic, and 22 (66.7%) of 33 eyes had PVD (Table 1).
Baseline Subject Characteristics.
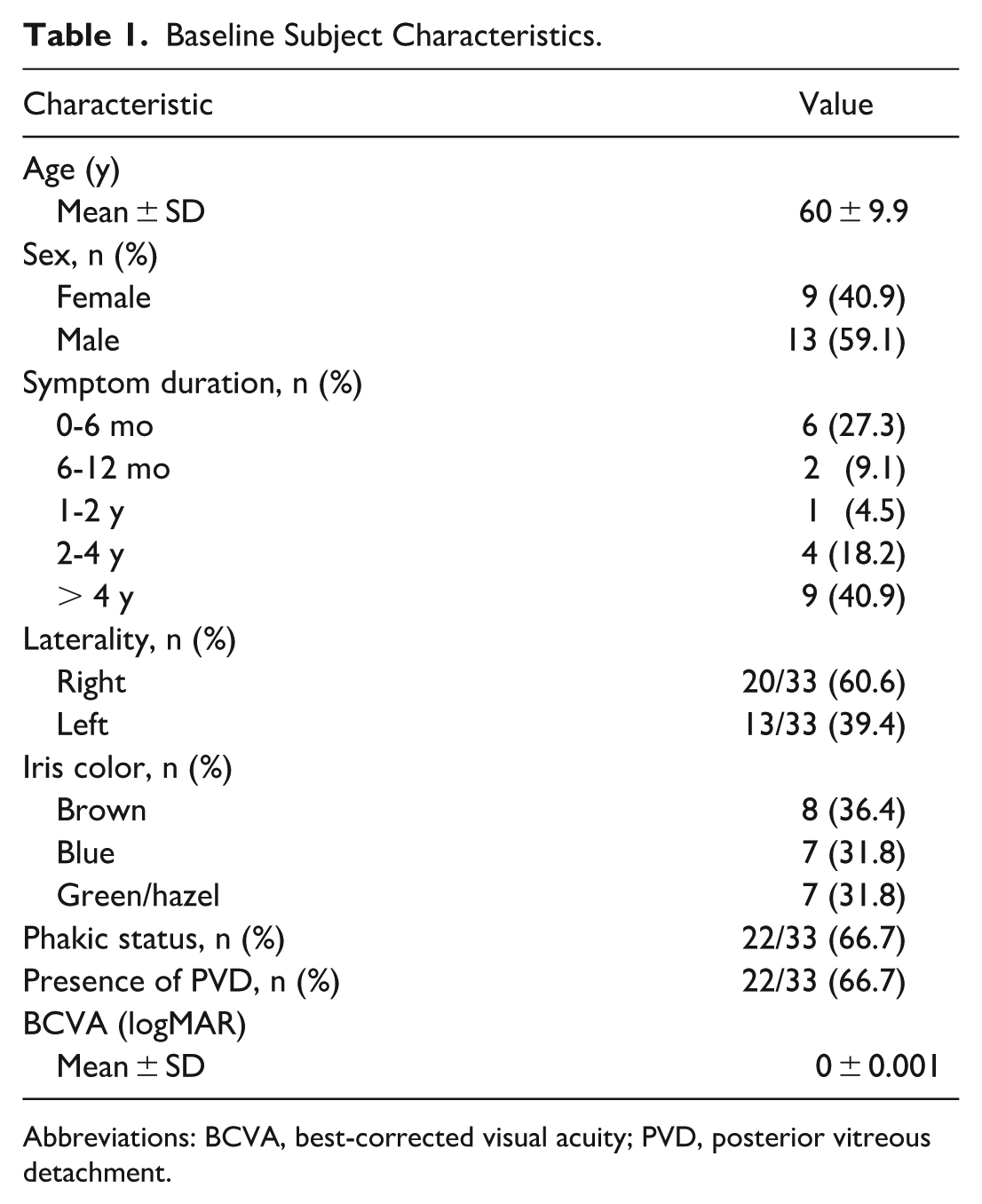
Abbreviations: BCVA, best-corrected visual acuity; PVD, posterior vitreous detachment.
Primary Outcomes
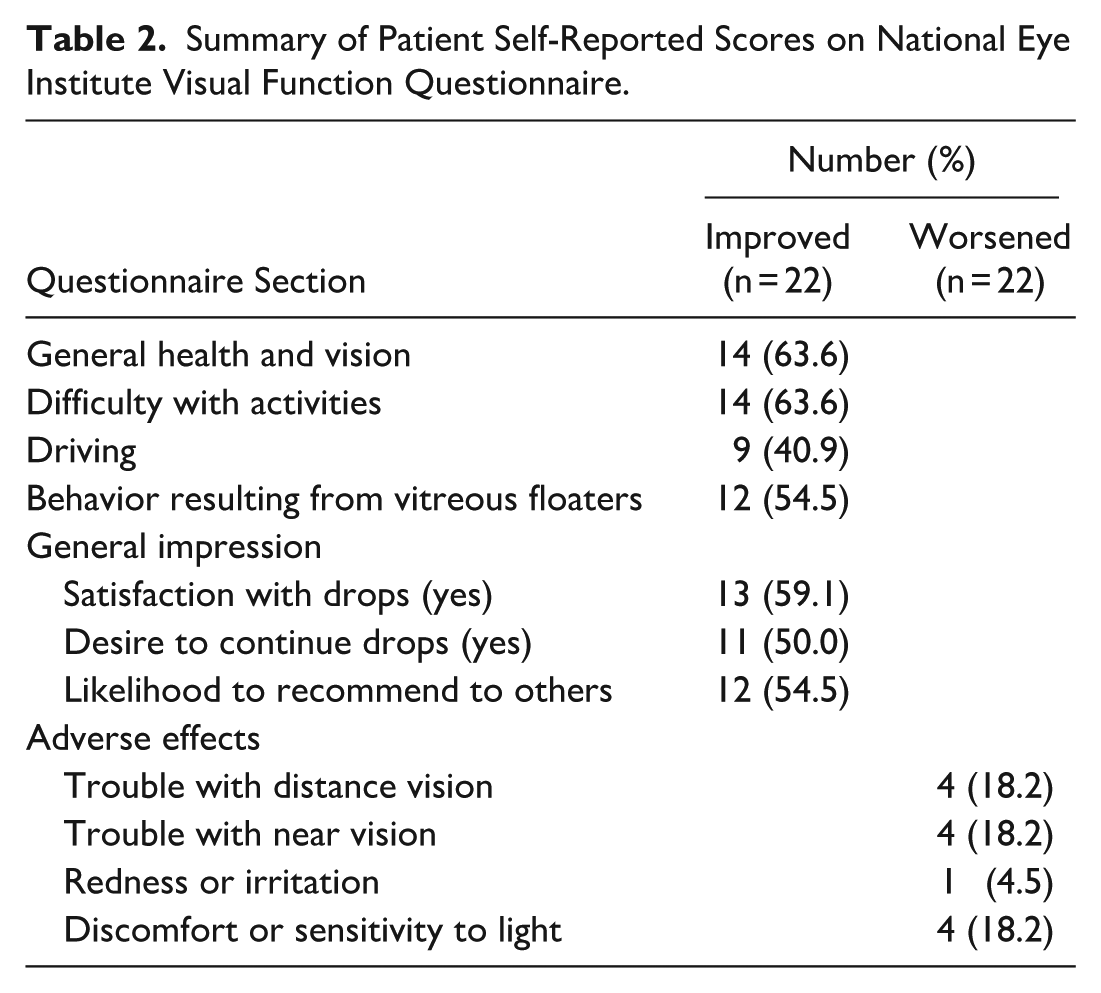
Of the 22 patients who completed 7 consecutive days of drop use and returned the National Eye Institute Visual Function Questionnaire, 13 (59.1%) reported being “satisfied” or “very satisfied” with the drops, and 11 patients (50%) reported that they would continue using the medication (Table 2). Considering all patients who received the medication, and assuming that discontinuation before 7 days resulted from dissatisfaction, 13 (29.5%) of 44 patients were “satisfied” or “very satisfied” with the drops, and 11 (25%) of 44 patients indicated they would continue use. The mean age of satisfied and unsatisfied patients was 60.7 ± 10.5 years and 59 ± 9.5 years, respectively (P = .703). There was no significant relationship between iris color (blue vs non-blue) and drop satisfaction (P = .648). There was no significant relationship between phakic status and either satisfaction (P = .520) or desire to continue drop use (P = .730). The presence or absence of PVD was not significantly associated with satisfaction (P = .520) or desire to continue drop use (P = .730). Among patients who trialed the drops, 1 underwent laser vitreolysis, and 4 underwent vitrectomy for floaters during the follow-up period of 8.9 ± 2.5 months.
Summary of Patient Self-Reported Scores on National Eye Institute Visual Function Questionnaire.
Secondary Outcomes
Scores on specific dimensions of self-reported health status, as measured by the modified National Eye Institute Visual Function Questionnaire, showed that of the 22 patients, 14 (63.6%) reported improvement in “general health and vision,” 14 (63.6%) in “difficulties with activities,” 9 (40.9%) in “driving,” and 12 (54.5%) in overall “behavior” (Table 2). The most commonly reported adverse effects were worsened near vision in 4 patients (18.2%), worsened distance vision in 4 patients (18.2%), and light sensitivity in 4 patients (18.2%). Of the 4 patients who reported worsened distance vision, 2 remained satisfied overall and indicated they would continue the drops. Of the 4 patients who reported worsened near vision, 3 were still satisfied overall and indicated they would continue the drops. Of the 4 patients who reported worsened photophobia, 3 were still satisfied overall and indicated they would continue the drops.
Conclusions
To our knowledge, this is the first study to demonstrate that low-dose 0.01% atropine eye drops can be effective in alleviating persistently symptomatic vitreous floaters. A substantial proportion of patients reported being “satisfied” or “very satisfied” with the drops—29.5% of all patients prescribed the medication (including those who did not complete the modified National Eye Institute Visual Function Questionnaires, with nonresponse presumed to indicate dissatisfaction), and 59.1% of those who did complete the questionnaires. We now counsel patients that the efficacy of low-dose atropine may range from 30% to 60%. We consider it a reasonable, noninvasive therapeutic alternative for patients with persistently symptomatic vitreous floaters, regardless of PVD or iris color. It may serve as a long-term solution, a pro re nata treatment, or a temporizing measure while more invasive options such as vitrectomy and laser vitreolysis are considered, or until symptoms (or the patient’s adaptability to their symptoms) improve over time.
Patients may benefit from having additional therapeutic options for floaters, as the only established treatments—laser vitreolysis and PPV—may be associated with potentially vision-threatening complications. Vitrectomy success rates are reported to be high, based on improvements in symptoms assessed by questionnaires and measures of contrast sensitivity and straylight, with reported satisfaction rates of up to 96% and normalization of contrast sensitivity function by 1 week postoperatively.9,13 Studies on laser vitreolysis report varying rates of symptomatic improvement, from 38% to 54%.14 –16 However, both surgical and laser interventions carry a risk of significant complications. Perioperative complications of vitrectomy include retinal tears or detachment, changes in intraocular pressure, cataract formation, and endophthalmitis. 17 Complications associated with laser vitreolysis include retinal damage, crystalline lens or posterior capsule damage, and open-angle glaucoma. 14
Conversely, topical low-dose atropine has fewer potential adverse effects, carries a negligible risk of severe vision loss, and is an established treatment for myopia progression in children.18,19 As a nonselective muscarinic antagonist, its adverse visual effects primarily relate to pupillary dilation and impaired accommodation. The most common adverse effect in children is dose-dependence and may include symptoms such as photophobia, reduced near visual acuity, and allergic conjunctivitis. 20 In children treated with low-dose atropine, no serious treatment-associated adverse reactions have been reported.21,22
A study of adult myopic patients found no significant negative effect of 0.01% atropine on contrast sensitivity. 23 Loss of accommodation and photophobia are minimal, as pupil dynamics are largely preserved and the medication exerts only a small effect on accommodation. Therefore, low-dose atropine is typically safe and well-tolerated. In our study, although 18.2% of patients reported worsening of distance vision, near vision, or photophobia with drop use, most of these patients remained satisfied and indicated they would continue treatment, reporting that the symptoms were not a major deterrent. Lack of or minimal improvement in floater symptoms was a more common source of patient dissatisfaction and the primary reason for discontinuation.
Clinicians may have anecdotal experience observing the effects of dilation drops on vitreous floaters. For example, it is not uncommon for patients who are dilated during an examination to report that their floaters have diminished since receiving the dilation drops. Further research should explore whether the in-clinic response to full-strength dilation drops (typically 2.5% phenylephrine and 1% tropicamide) can predict satisfaction with low-dose atropine eye drops.
Despite our positive experience with low-dose atropine, we continue to recommend observation and patience for most patients with symptomatic vitreous floaters. We restrict the use of low-dose atropine to those without narrow angles (as assessed by the Van Herick method) and those with persistently symptomatic floaters lasting more than 3 months following onset of PVD symptoms. Specifically, we do not prescribe low-dose atropine to those patients with an acute PVD, as we do not want to mask their perception of increased floaters that could alert them to the possibility of a new retinal break, retinal detachment, or vitreous hemorrhage.
In patients who have tried low-dose atropine and have vitreous syneresis without a complete PVD, we do not offer PPV as a therapeutic option, reserving this option only for those patients with complete PVD. A patient’s positive or negative response to low-dose atropine does not influence our decision to offer vitrectomy for patients without complete PVD. Conversely, the response to low-dose atropine may affect our decision to offer vitrectomy to those patients with a complete PVD. For those who have a positive response to low-dose atropine, the surgeon and patient may be less inclined to proceed to a vitrectomy, and for those with a lack of response to low-dose atropine, they may be more inclined to proceed to a vitrectomy. Further research on the role of low-dose atropine in influencing surgical decision-making would be beneficial.
Limitations of our study include its retrospective design, short duration, and small sample size. Several patients prescribed low-dose atropine eye drops did not complete a full 7-day course of treatment or complete the National Eye Institute Visual Function Questionnaire. The reasons for discontinuation or nonresponse remain uncertain. For our statistical analysis, we presumed that these patients were dissatisfied with the drops. Therefore, we report the efficacy of low-dose atropine drops in 2 ways: (1) all patients prescribed the drops, counting nonresponders as dissatisfied (yielding a 29.5% satisfaction rate), and (2) only patients who completed the questionnaires (yielding a 59.1% satisfaction rate). Additionally, the period between drop use and questionnaire completion could not be controlled and may influence recall bias. The absence of a control group constitutes another limitation, as patients may report positive findings resulting from acquiescence bias.
Finally, the sample size did not allow for an adequate analysis of whether clinical characteristics, such as hyaloid status or phakic status, were associated with treatment efficacy, or whether factors like age and iris color may have impacted the rate of side effects related to pharmacologic dilation and loss of accommodation. Efficacy of low-dose atropine for myopia progression in children has been reported to depend on iris color; however, in the adult population, no significant difference in pupillary dilation was found for blue and non-blue irises.11,24
Future studies may be improved in a few ways. Larger, prospective studies with a control group would help minimize sources of bias and better characterize the patient populations most likely to benefit from low-dose atropine drops. Long-term follow-up studies are needed to assess sustained efficacy and potential adverse effects. The Vitreous Floaters Functional Questionnaire is another self-administered questionnaire designed to assess the impact of floaters on quality of life, scored on a 100-point scale. 25 Although the Vitreous Floaters Functional Questionnaire is a more recently developed assessment compared with the National Eye Institute Visual Function Questionnaire, it has been shown to correlate with vitreous structure and visual function, with significantly greater magnitude of improved scores following limited vitrectomy compared to the National Eye Institute Visual Function Questionnaire. The use of this questionnaire may be considered a useful outcome measure in future studies. Ultrasound data were not included in this study but should be considered in future studies to correlate with qualitative assessments. Objective measures of vitreous echodensity using quantitative ultrasound have been previously shown to correlate with both contrast sensitivity and quality of life in patients with floaters, and may help guide patient selection. 5
Our study shows that low-dose atropine can be an effective and low-risk treatment option for select patients with persistently symptomatic vitreous floaters. These drops can be considered in patients who are not interested in or are not suitable candidates for more invasive interventions such as PPV or laser vitreolysis.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264251364819 – Supplemental material for Low-Dose 0.01% Atropine Eye Drops for Symptomatic Vitreous Floaters: A Noninvasive, Safe, and Effective Therapeutic Option
Supplemental material, sj-docx-1-vrd-10.1177_24741264251364819 for Low-Dose 0.01% Atropine Eye Drops for Symptomatic Vitreous Floaters: A Noninvasive, Safe, and Effective Therapeutic Option by Jeanette Du, Osama Sabbagh, Brian K. Do, Jason M. Huang, Joshua D. Levinson, Alexander Melamud, Mohammed K. Barazi and Mohsin H. Ali in Journal of VitreoRetinal Diseases
Supplemental Material
sj-docx-2-vrd-10.1177_24741264251364819 – Supplemental material for Low-Dose 0.01% Atropine Eye Drops for Symptomatic Vitreous Floaters: A Noninvasive, Safe, and Effective Therapeutic Option
Supplemental material, sj-docx-2-vrd-10.1177_24741264251364819 for Low-Dose 0.01% Atropine Eye Drops for Symptomatic Vitreous Floaters: A Noninvasive, Safe, and Effective Therapeutic Option by Jeanette Du, Osama Sabbagh, Brian K. Do, Jason M. Huang, Joshua D. Levinson, Alexander Melamud, Mohammed K. Barazi and Mohsin H. Ali in Journal of VitreoRetinal Diseases
Footnotes
Ethical Approval
The study received ethical approval from the WCG Institutional Review Board (#1-1699888-1) on September 28, 2023.
Statement of Informed Consent
This is an institutional review board–approved retrospective study; all patient information was de-identified, and patient consent was not required. Patient data will not be shared with third parties.
Declaration of Conflicting Interests
The author(s) declared no conflict of interest with respect to the research, authorship, and/or publication of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.