
Abstract
Keywords
Introduction
Posterior vitreous detachment (PVD) is a phenomenon that occurs most often due to aging. Normal vitreous can be thought of as a uniform elastic gel capable of a fairly equal distribution of forces along the vitreoretinal interface. 1 Over time, the vitreous gel undergoes a process of liquefaction (termed synchysis) and shrinking (termed syneresis). These changes are produced by the consolidation of collagen-hyaluronic acid meshwork fibers and the coalescing of the resultant liquefied vitreous.1–3 Notably, this creates 2 separate volumes with differing viscosities and, therefore, differing biomechanics. 2 Due to the pattern of collagen aggregation, liquefied vitreous typically coalesces near the center of the posterior chamber. 2 The creation of a biphasic vitreous gel disrupts the uniformity of elastic forces throughout the vitreous. This contributes to tractional forces at vitreoretinal attachment sites and dramatically alters vitreous biomechanics.1,4 Eventually, these forces become great enough to separate the vitreous and retina. The detachment typically occurs in order of perifovea, vascular arcades, fovea, mid-periphery, and optic nerve head. 5
Occurring in over 50% of individuals 70 years old and above,6,7 a PVD is often benign and results in complete separation of the posterior hyaloid and the internal limiting membrane of the retina. However, in an incomplete PVD, anterior-posterior vitreous traction may develop prior to the weakening and complete separation at the vitreoretinal interface. 8 The term vitreomacular adhesion (VMA) is used in the absence of foveal contour changes. Conversely, the presence of foveal changes secondary to tractional forces is termed vitreomacular traction (VMT). The most significant complication of VMT is perhaps the development of a full-thickness macular hole, with more focal vitreoretinal adhesions putting patients at greater risk of macular hole formation. 7
Current treatment options for patients experiencing VMT include observation, surgery, enzymatic vitreolysis, and pneumatic vitreolysis. A report of VMT release induced by ocular massage has been rarely reported. 9 Observation is seen as a reasonable first option in many cases. One recent study found that over a follow-up course of 23 months, 30% to 57% of VMT cases spontaneously released, depending on the severity of the traction. 10 The most common surgical treatment for VMT is detachment of the vitreomacular interface via pars plana vitrectomy with or without peeling of a concurrent epiretinal membrane. Reported success rates following this procedure range between 66% and 75%. 11 Surgery is generally reserved for cases with a macular hole, poor visual acuity, metamorphopsias, or other worsening symptoms of traction. 12 Medical management has shown limited success, with the enzymatic vitreolysis agent ocriplasmin (Jetrea) pulled from the market in 2020 following poor sales and concerns of adverse effects.13,14 Similar safety concerns regarding pneumatic vitreolysis have been raised by Baumann et al 15 who found that patients undergoing this procedure may be at risk of persistent macular hole, formation of new macular hole, or retinal detachment. Another study evaluating pneumatic vitreolysis in the treatment of VMT was terminated early citing higher-than-expected rates of retinal detachment and retinal tears. 16
One rarely explored treatment technique for VMT is the use of head motion to accentuate forces in the vitreous chamber and at the vitreoretinal interface. Such forces are experienced repeatedly by military pilots due to the maneuverability of modern combat aircraft. The vector of G forces placed on a pilot is dependent on the direction of acceleration in three-dimensional space. For example, a pilot applying right lateral acceleration experiences a relative left lateral G force. 17 The phenomenon is analogous to a car passenger’s relative leftward force experienced during an abrupt right turn. In contrast to a car, however, the direction of acceleration and corresponding force vectors during flight can be experienced along 3 planes rather than 2. This difference allows for potential force exertion in all vectors perpendicular to the vitreoretinal interface. Commercial flight simulators are a more accessible option and expose operators to said force vectors without the dangers of excess G force seen in modern military aviation.18,19 The following case describes an instance of VMT resolution achieved following a commercial flight experience in a patient who deferred a vitrectomy procedure after a comprehensive discussion of the benefits and risks of surgery, but was interested in exploring non-invasive options.
Case Report
A 66-year-old woman presented with worsening vision in the left eye (OS). She reported a past ocular history of posterior scleritis OS, which was managed with meloxicam 7.5 mg/day and prednisone 5 mg/day, epiretinal membrane OS (Figure 1, A), cataract extraction with posterior chamber intraocular lens placement in both eyes (OU) 1 year prior, and retinal holes status post laser retinopexy OU. The right eye (OD) also previously developed a macular hole treated successfully with pars plana vitrectomy and membrane peel 2 years prior. The best corrected visual acuity (BCVA) OS was 20/60. On optical coherence tomography (OCT) OS, the development of VMT was observed (Figure 1, B).
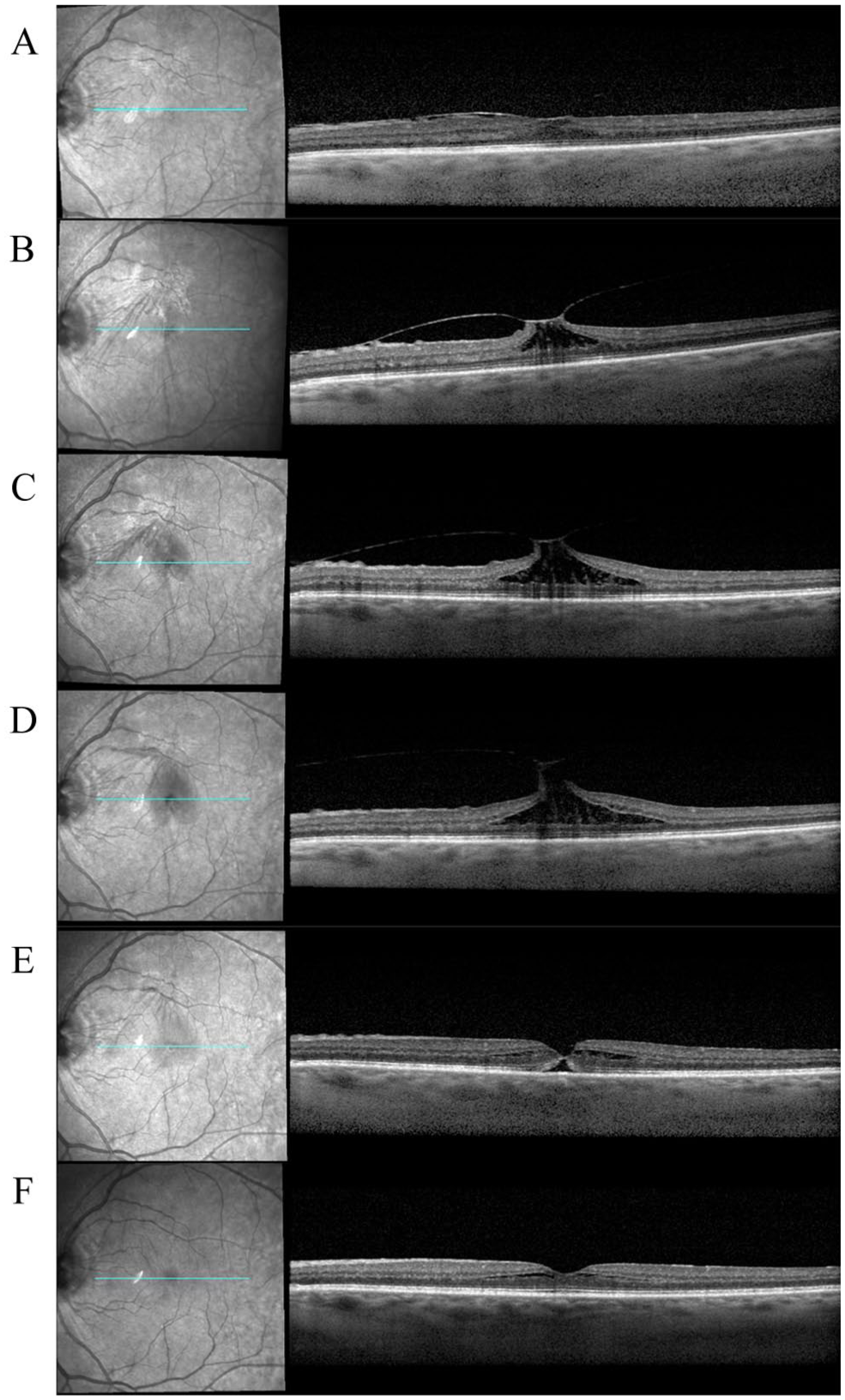
Optical coherence tomography (OCT) scans of the vitreomacular traction in the left eye prior to (A-D) and following (E-F) flight simulation. OCT shows a mild vitreomacular adhesion at (A) 3 months prior to the flight simulator experience. Vitreomacular traction progression is observed during follow-up at (B) 4 weeks prior, (C) 3 weeks prior, and (D) 2 weeks prior. Following the commercial flight experience, improvement is observed with OCT that shows findings consistent with an impending macular hole at (E) 1 week following, with resolution at (F) 3 months following the flight simulator.
Observation was elected initially in anticipation of possible PVD development, leaving a vitrectomy as a future possibility. The patient was started on topical ketorolac to conservatively manage the VMT-associated cystic/intraretinal fluid rather than proceeding to surgery immediately, as the patient reported ocular dysesthesia following her prior surgery OD. Over the ensuing 3 months, the patient’s VMT further progressed as shown on OCT (Figure 1, C and D). The patient’s vision remained unchanged, and she was interested in pursuing other non-invasive therapies.
A flight simulator at the Strategic Air Command & Aerospace Museum in Ashland, Nebraska provides an immersive simulated aviation experience for riders including sudden jerking movements and barrel rolls. 20 The patient was interested in trialing this experience with a pilot familiar with flight simulation in an attempt to relieve her VMT, and was asked to return for follow-up in 3 weeks.
Following the simulator ride, resolution of VMT was confirmed on OCT (Figure 1, E) with improvement in foveal contour. However, OCT showed evidence of an impending macular hole. Subsequent follow-up 1 month later showed the patient’s visual acuity improved to a BCVA of 20/25, and vision remained stable at 6-month follow-up. Further improvement of the foveal contour was demonstrated by OCT at 3-month follow-up (Figure 1, F).
Discussion
Our patient’s unique case prompts the question of the role of head motion in PVD development. Several factors contribute to the contour at the vitreoretinal interface and associated visual acuity change. These include proteins (laminin, fibronectin, collagen) that bind the posterior hyaloid to the internal limiting membrane. In addition, the vitreous humor produces both anterior and posterior forces, along with tangential forces that are perpendicular to the surface of the retina.1,2,21
Response to extraocular forces exerted on the aging vitreous is heavily influenced by the interaction between intra-vitreous components.1,2 Given the different composition of the 2 phases, each phase uniquely responds to the acceleration forces created with eye movement. In addition to the leftward force exerted on the vitreoretinal interface with abrupt rightward acceleration, the inner liquid phase exerts force against the surrounding gel phase. This further contributes to the stress experienced at the vitreoretinal junction. Bayat et al 2 sought to characterize the effect of these forces in patients with repeated saccade eye movements. They found vitreoretinal shear stress was proportional to angular velocity and saccade amplitude. Additionally, stress in the vitreous and on the retina continued to oscillate after cessation of saccade movement. This further illustrates how the interaction between the vitreous phases accentuates forces exerted on the eye. The maneuverability of flight simulators allows for wide amplitude movements without the limitations of the extraocular range of motion. This allows these machines to produce adequate angular velocity, amplitude, and force required for complete separation of the vitreous from the retina.
Given the temporal association of the flight simulator experience and subsequent PVD development, it is plausible that the significant, sudden, and repeated motions of a flight simulator may have contributed to a complete PVD and resolution of VMT. While it is possible that VMT resolution was coincidental, the patient’s course did not follow the typical timing of spontaneous VMT resolution. Prior publications have analyzed the timing of VMT resolution and found that in the cases that resolve, the timing ranges from 8.75 to 18 months following initial diagnosis.10,14,22,23
Limitations of this therapy method include a lack of quantified force vectors and inefficient use of directional acceleration. There is concern that forceful separation of the vitreous and retina may contribute to force vectors that may lead to retinal pathology, including macular hole formation. Traumatic PVD seen during violent deceleration from parachute accidents has contributed to a condition known as whiplash maculopathy. 24 While it is unknown whether a commercial flight simulator could be capable of velocities necessary to induce whiplash maculopathy, we did not observe this finding in our patient. Other methods of mechanical PVD induction, such as pneumatic vitreolysis, have raised concern for macular hole formation 15 and retinal detachment.15,16 Pneumatic vitreolysis involves injection of gas intraocularly, in contrast with the non-invasive nature of harnessing rotational forces with rapid head movement. Despite different approaches, such adverse effects must be considered in all mechanical therapies for VMT. Of note, the OCT at follow-up showed initial improvement of the foveal contour but was suggestive of an impending macular hole (1e). A full-thickness macular hole remains a potential risk, and caution is thus advisable. Further understanding of this treatment method could involve in vitro modeling to determine more precise, quantifiable metrics of force vectors at the vitreoretinal interface.
Whether other patients undergoing the same flight simulator experience have experienced a PVD or vitreous changes is unknown. However, other related experiences with similar force dynamics at the vitreous-retinal interface could provide insight into whether flight simulation or other phenomena could contribute to PVD induction.
Footnotes
Acknowledgements
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Ethical Approval
This article was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)-compliant manner.
Statement of Informed Consent
Informed consent was not necessary as the case described the care of 1 patient and excluded any personally identifiable information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Eye Institute of the National Institutes of Health under award number R01 EY029594 (Steven Yeh). Funding support is also provided by the National Strategic Research Institute Program of Excellence Award, Macula Society Retina Research Foundation Cox Family Grant, Retina Society, Association for Research in Vision and Ophthalmology Mallinckrodt Foundation Young Investigator Award, and the Stanley M. Truhlsen Family Foundation, Inc.