
Abstract
When encountering diseases of the anterior vitreous and peripheral retina (ie, the “middle segment” of the eye), vitreoretinal (VR) surgeons are specifically trained in surgical techniques for managing the vitreous and visualizing the peripheral retina during anterior vitrectomy, and therefore, they are well equipped to address the complications of surgery involving the anterior vitreous space. This clinical update reviews and compares the current literature discussing techniques and patient outcomes related to complete pars plana vitrectomy versus incomplete, subtotal pars plana vitrectomy, and addresses the proposition of developing an abridged training curriculum for non-VR surgeons to acquire the knowledge and skills required to perform these procedures. Recent studies confirmed that operating in the anterior vitreous carries potential risk of retinal tear, retinal detachment, and other adverse events that may cause vision loss. To mitigate these risks, studies suggest that the use of dedicated visualization equipment and illumination instruments is necessary for surgeons to safely perform anterior vitrectomy and recognize complications, should any occur. Performing VR surgery in the absence of wide-angle viewing systems, endoillumination, careful peripheral examinations, modern vitrectomy platforms, and appropriate training may lead to outcomes that are detrimental to patient safety.
Introduction
Vitreoretinal (VR) surgery is a well-established subspecialty of ophthalmology requiring 2 years of postresidency training, according to the standards developed by the Association of University Professors in Ophthalmology fellowship compliance committee in coordination with the American Society of Retina Specialists, Macula Society, and Retina Society. 1 Procedures performed by VR surgeons to improve or preserve vision often require the surgeons to handle retinal tissue layers ranging just 0.5–3.1 microns in thickness while they skillfully avoid iatrogenic trauma to the neurosensory retina—trauma that can be created indirectly through traction on the vitreous.2–4 During surgery, wide-angle viewing systems, including contact lenses, 5 non–contact lens viewing systems, 6 and 3-dimensional heads-up display systems, 7 are employed to appropriately visualize the choroid and retina all the way to the far periphery (including the ora serrata, pars plana, ciliary body, and zonules). These viewing systems require endoillumination provided by a handheld light pipe or a chandelier light to adequately examine these tissue layers. Many VR surgeries are also performed on an emergent basis to avoid irreversible vision loss for indications such as rhegmatogenous retinal detachment (RRD),8–10 endophthalmitis,11,12 acute elevation in intraocular pressure,13,14 intraocular foreign body,15,16 choroidal hemorrhage,17,18 and vitreous hemorrhage. 19 The goal of surgery in many of these scenarios is to return the eye as close as possible to its normal anatomic state and prevent permanent blindness, an outcome that can occur if these diseases are left untreated.
Recently, there have been discussions—primarily among non-VR surgeons—regarding the “middle segment” of the eye, a term surgeons use to refer to an area 2–4 mm posterior to the limbus. 20 In a report by Hannush and colleagues, 20 non-VR surgeons mention that the anatomic definition of the middle segment is not vital, but the concept of anterior segment surgeons performing a solo surgery from both an anterior and posterior approach is of more importance. The focus of that report was primarily on patients with dislocated intraocular lenses (IOLs), and the authors recommended that the best approach in these patients is a pars plana approach involving an anterior, or subtotal, vitrectomy. They assert that a total vitrectomy is not necessary in all cases, and that a complete subtotal anterior vitrectomy with minimal traction on the anterior retina is sufficient for nearly every dislocated IOL case.
Concerningly, some of these non-VR surgeons claim competency in performing these types of surgeries outside of residency or fellowship training, acquired in a brief skills session with trained mentors. 20 The notion that a short course or observership would provide someone with the abilities necessary to perform VR surgery is erroneous and can lead to poor patient outcomes. For example, non-VR surgeons may decide to perform subtotal vitrectomies for other conditions or purposes, such as vitreous hemorrhage, vitreous biopsies, concomitant placement of pars plana glaucoma shunts, intraocular foreign body, vitreous prolapse into the anterior chamber, or symptomatic vitreous opacities (VOs). In fact, surgeries for symptomatic VOs—sometimes referred to as “floaterectomies”—have been performed in the office setting using a single port vitrectomy machine. 21 Even when a floaterectomy is performed via a 3-port pars plana vitrectomy, the rate of return to the operating room has been reported to be higher than 3%, associated with retinal detachments in up to 11% of eyes, and eyes are still at risk of developing endophthalmitis.22–25
Given these concerns and the skills and training required to safely perform VR surgery, as well as the potential for significant patient harm if not done in an appropriate manner (or simply not done at all), we aimed to bring attention to the so-called “middle segment” concept and evaluate the importance of the surgical techniques and training employed by VR surgeons when treating patients with diseases involving the vitreous, such as management of dislocated lenses or removal of VOs. The concerns regarding non-VR surgeons operating in the middle segment of the eye primarily involve 3 areas: inadequate VR surgical training, lack of visualization techniques and technology, and poor patient outcomes.
Vitreoretinal surgical training
VR surgical training typically centers around procedures related to the anterior segment. Therefore, surgeons operating on the anterior segment may not be as well-versed in posterior segment procedures, such as use of pars plana vitrectomy, endolasers, or endoilluminators. However, it has been suggested by some that handling of these tools can be easily taught or learned in a weekend course. 20 The suggestion that a qualified VR surgical training program—which, in the US, comprises a 2-year fellowship—could be condensed into 2 days calls the validity of this proposal into question. VR fellows routinely perform 500–1200 posterior segment surgeries during their fellowship period while also managing the short- and long-term postoperative care of their patients.26,27 Providing an overview of even a fraction of the VR surgical techniques available, let alone teaching participants the skills to recognize and manage the associated complications, 28 is impossible to be condensed into a single weekend training course. It is also worth emphasizing that the management of potential VR surgical complications, many of which occur postoperatively rather than intraoperatively, 28 is something that would be handled most appropriately by VR surgeons. Non–VR-trained surgeons may lack the experience to identify early postoperative complications and, most importantly, may not be able to identify and rectify intraoperative complications (as detailed below) at the time that they occur.
With regard to its anatomy, when surgeons operate near the VR interface, the vitreous base inserts 2 mm anterior to and 4 mm posterior to the ora serrata (Figure 1) and is located approximately 5 mm posterior to the limbus in all quadrants of the eye; however, it is more anterior nasally than other quadrants (Figure 2). 29 Thus, surgeons operating through the pars plana 2–4 mm from the limbus risk violating the anterior vitreous base, which may lead to inadvertent iatrogenic retinal breaks. The use of limbal-based anterior vitrectomy is commonly employed by cataract surgeons in the management of vitreous prolapse during cataract surgery, which may occur due to zonular insufficiency or posterior capsule rupture. 30 This technique is most often done with cataract phacoemulsification systems, and the cut rate and fluidics are vastly different than those used in current vitrectomy platforms. 31 Older iterations of the Infinity system (Alcon Surgical, Inc.) had a maximum cut rate set to 800 cuts per minute for anterior vitrectomy, but with updates, the cut rate has increased to approximately 2500 cuts per minute. The newer Centurion system (Alcon Surgical, Inc.) has a maximum cut rate of 2500 cuts per minute.32,33 In contrast, the current vitrectomy machines employed by VR surgeons have cut rates of up to 20 000 cuts per minute, and have duty cycles approaching 100% and improved IOP control with a 2- or 3-port approach.34,35 This fluidics technology has decreased intraoperative hypotony during vitrectomy, and offers efficiency and safety advantages over the systems currently in use by non-VR surgeons, who perform anterior vitrectomy through a system designed primarily for cataract surgery. The precise control of fluidics, cut rate, and vacuum currently employed by VR surgeons helps avoid unnecessary iatrogenic retinal breaks during surgery, as well as reducing the risk of suprachoroidal hemorrhage.
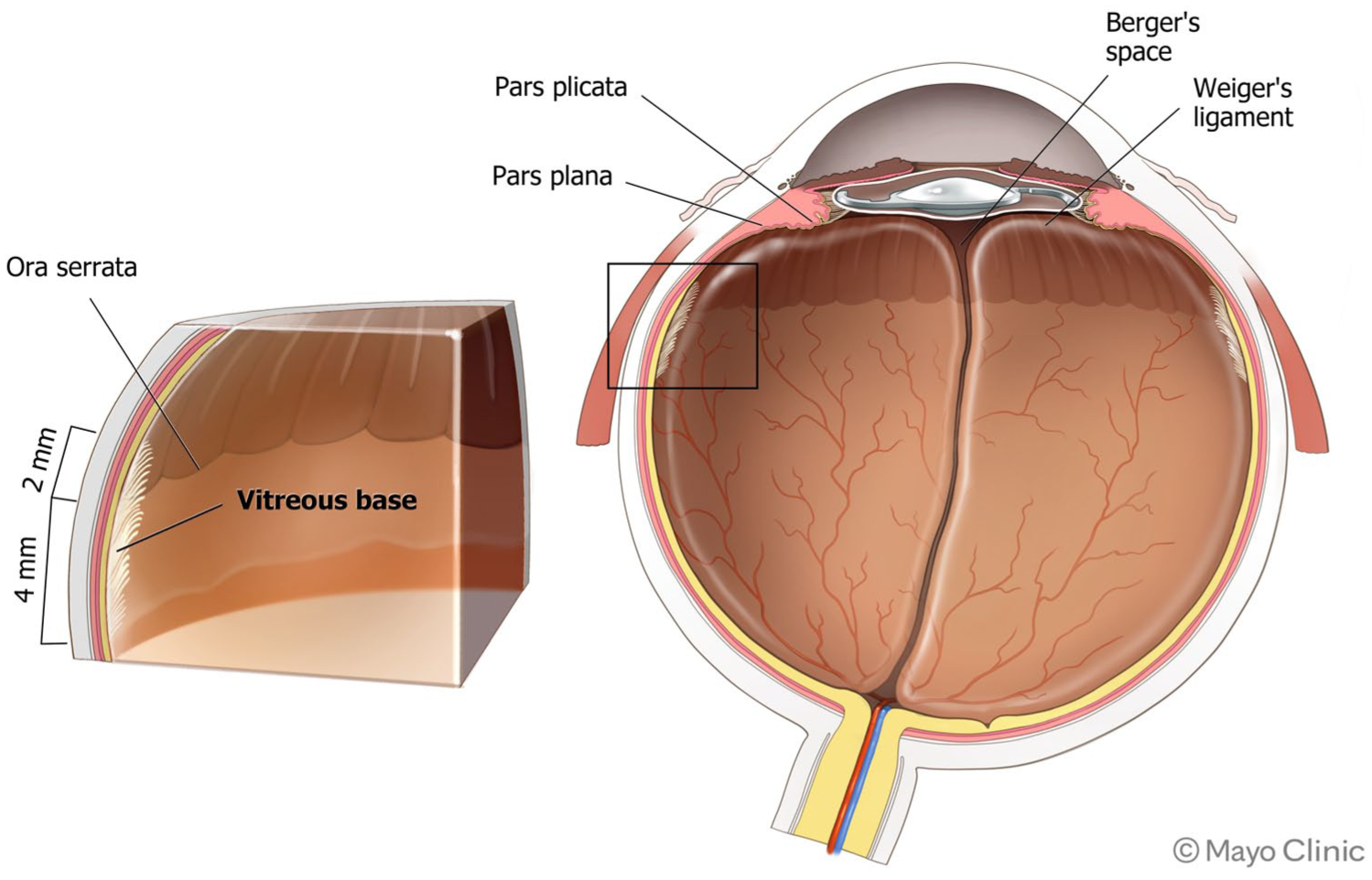
Schematic cross-section of a pseudophakic eye following cataract surgery, highlighting the insertion of the vitreous base in relation to the ora serrata and pars plana (boxed area, with magnified image on left), as well as the anterior rotation of the anterior vitreous base and Weiger’s ligament.
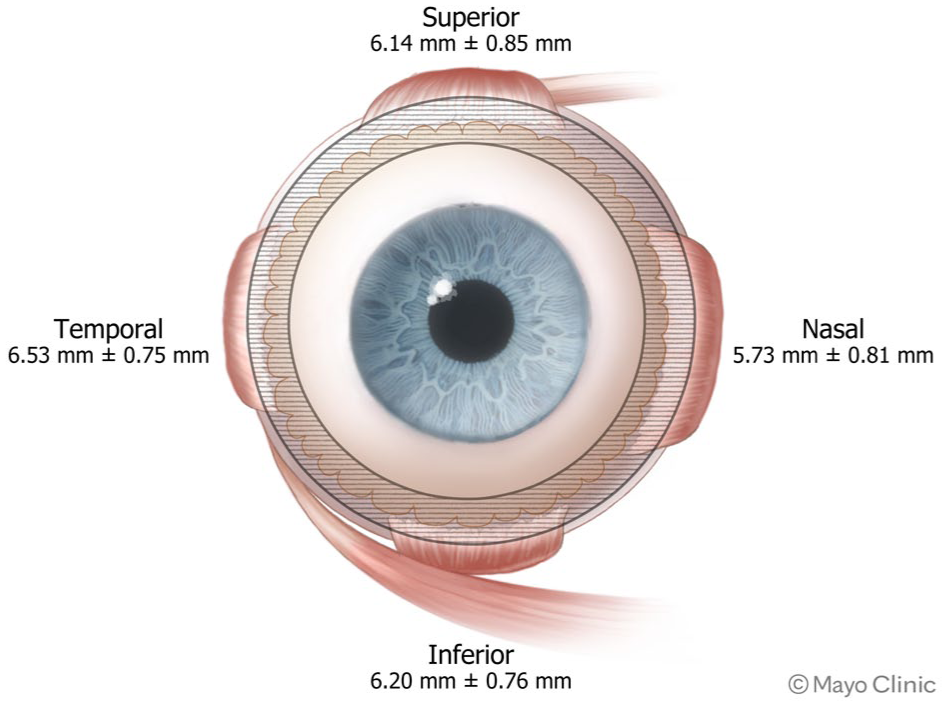
Schematic of a right eye, showing the location of the ora serrata (mean distance ± standard deviation) in relation to Schwalbe’s line near the surgical limbus. Note the more anterior location nasally compared to the inferior, superior, and temporal quadrants, with the approximate insertion of the vitreous base in relation to the ora (shaded region between circles).
Other non-VR surgeons perform anterior vitrectomy through a sclerotomy created through the pars plana. While this is a valid approach, there is limited published evidence regarding the safety and efficacy of this approach.36,37 Some studies have shown a retinal detachment incidence of up to 15% after 8 years following an anterior vitrectomy during a complicated cataract surgery, with up to 4.5% of eyes also developing IOL dislocation.38,39 In contrast, Thornton et al 36 reported a series of nearly 350 eyes in which a modified pars plana vitrectomy technique was used, based on a previously described approach from the 1970s for retained lens material from VR surgeons. 40 Thornton and colleagues observed improved anatomic outcomes with this technique, with only 3 eyes (approximately 1% of patients) developing a subsequent RRD, and 1 eye developing a retinal tear postoperatively. 36 Of note, 40 eyes had < 1 month of follow-up in the study, and 2 eyes that met the original inclusion criteria were ultimately excluded after needing VR surgery following the initial anterior vitrectomy. 36 Those authors postulated that the improvement was attributable to the use of a pars plana approach 36 rather than a limbal approach, which has been shown to have more significant VR traction on the peripheral retina.41,42 In the reports by Thornton et al 36 and Clark et al,38,39 there was no mention of whether an intraoperative peripheral retinal examination was performed.
Patients who have retained lens material after complicated cataract surgery and subsequent pars plana vitrectomy have a postoperative RRD risk profile43,44 similar to that following vitrectomies performed for VOs. 24 In a 2020 study by Chan and colleagues examining more than 290 eyes that had retained lens material after 23-gauge pars plana vitrectomy following a complicated cataract surgery, 9 eyes (3.1%) developed a postoperative RRD. 43 Even with macular surgery, manipulation of the peripheral vitreous base during surgery or simply trocar placement can lead to postoperative complications. In an IRIS database study evaluating routine pars plana vitrectomy for eyes with epiretinal membrane and macular hole, the return to the operating room rate for surgeries other than cataract surgery was 5.5% for eyes with epiretinal membrane and 6.8% for eyes with macular hole. 45 In that same study, the rates of RRD following VR surgery for eyes with epiretinal membrane and eyes with macular hole were 2.5% and 2.0%, respectively. 45 These rates are similar to those in the IRIS database study evaluating outcomes following pars plana vitrectomy for VOs, in which the return to the operating room rate was 3.7%, with 2.6% of eyes developing an RRD following VR surgery for VOs. 24 Recently, in an updated report of the IRIS registry data presented at the 2024 American Society of Retina Specialists Annual Meeting, Chan 46 described even more dramatic complications following pars plana vitrectomy for VOs, with a postoperative vitreous hemorrhage rate of 26.3%, postoperative endophthalmitis rate of 3.7%, and postoperative RRD rate of 4.2%.
Visualization and technology
In addition to the skillset and technology required to operate safely within the anterior vitreous cavity, a key element missing in surgeries performed by non–VR-trained surgeons is visualization techniques. In addition to a standard operating room microscope, VR surgeons utilize sophisticated wide-angle viewing systems to visualize the vitreous and posterior segment, including contact lenses, 5 non–contact lens viewing systems, 6 and 3-dimensional heads-up display systems, 7 all of which offer unparalleled viewing capabilities for the surgeon. While these systems offer excellent views of the peripheral retina, simultaneous scleral depression is often required to adequately view the entire peripheral retina, where tears, holes, and other breaks can be appropriately identified and then treated.
Because of the disease type and complex retinal pathology of patients requiring VR surgery, the rate of identifying preoperative retinal breaks (using a scleral-depressed examination) or intraoperative retinal breaks is approximately 5–8% during routine VR surgery, with the rates being up to 20% for cases of vitreomacular traction or macular holes.47–49 Many, but not all, of these retinal tears and peripheral retinal pathologic characteristics are present preoperatively; in a case series examined by Moore et al, 49 6% of eyes (20/343) with retained lens material had a retinal tear noted before pars plana vitrectomy was performed. Therefore, the ability to comprehensively examine the entire retina intraoperatively is imperative for any surgeon performing a pars plana vitrectomy. The use of standard operating microscopes alone does not allow a complete evaluation of the retina—especially the anterior retina and pars plana—intraoperatively without endoillumination (especially if a single-port vitrectomy is performed), and this can lead to inadvertently overlooked pathology. Indirect ophthalmoscopic examination is rarely performed at the conclusion of an anterior vitrectomy, and even if it is performed, the examination is often limited by corneal clouding or newly created corneal wounds that preclude scleral depression. On the other hand, during conventional VR surgery, peripheral retinal examinations in high-risk patients can be performed thoroughly and safely for both preexisting or iatrogenic peripheral segment and posterior segment pathology. It is standard of care to perform a thorough peripheral retinal examination at the time of any pars plana vitrectomy.
Patient outcomes
Over recent years, with the advent of new secondary fixation techniques such as the Yamane, 50 modified Yamane, 51 and Gore-Tex sutures, 52 most secondary IOL surgeries performed primarily by VR surgeons are either scleral-fixated or scleral-sutured procedures, with successful refractive outcomes.53,54
In a recent series of more than 550 secondary IOL surgeries performed by VR surgeons, 17.5% of cases required use of an endolaser for intraoperative retinal tears, holes, or tufts (with 7.3% of eyes having a retina tear identified intraoperatively); 55 this technique was made much easier with the use of both wide-angle viewing systems and current vitrectomy platforms. Certainly, surgeons could employ laser indirect ophthalmoscopy or cryoretinopexy, but these skills often require a great deal of training as well. There is limited data regarding visual and anatomic comparisons between vitrectomy performed either via the pars plana or anteriorly for subluxed IOLs; however, VR surgeons continue to achieve improved anatomic and refractive outcomes in patients after secondary IOL surgeries are performed.56–58
Furthermore, VR surgeons have employed techniques not only to safely remove a dislocated IOL, but also to address refractive limitations simultaneously.59,60 Cases necessitating secondary corneal transplantation, iris repair, or glaucoma procedures perhaps may be best approached in a staged manner, since refractive shifts in corneal biometry have been noted with these types of surgeries.45–48 Additionally, access to VR surgeons is improving, especially in underserved communities; 61 however, ultimately, limited access may hinder the ability of some patients to undergo a combined surgery or may delay care. This reasoning, though, does not support non-VR surgeons performing these surgeries, as any VR complications would then be further compounded by limited access to a VR surgeon.
As VR surgeons, we are not advocating that only ophthalmic surgeons perform IOL exchanges. However, we are emphasizing that certain capabilities are essential when operating in the vitreous space: the need for enhanced peripheral viewing systems, appropriate vitrectomy platforms and fluids, and the ability to handle intraoperative and postoperative complications. Certainly, many anterior segment surgeons possess expertise on optimizing refractive outcomes following secondary IOL surgery. Thus, when significant pars plana vitrectomy work is necessary, we would advocate that VR and non-VR surgeons work in tandem to achieve optimal patient outcomes.
As new techniques evolve within ophthalmology, surgeons must continue to adapt to provide the highest level of care. Medical malpractice claims within ophthalmology have identified that poor postoperative vision, incorrect lens power selection, inadequate anesthesia, and postoperative complications such as retinal detachment and endophthalmitis are the primary causes for malpractice claims following cataract surgery.62–64 Claims specifically involving retinal detachments usually involve a delay in treatment/examination or a failure to diagnose due to an inadequate examination. 62 In the research by Kim and colleagues examining malpractice claims following retained lens fragments within the Ophthalmic Mutual Insurance Company database, the development of a retinal detachment following complicated cataract surgery was not associated with claims outcomes. 64 In contrast, for every claim (7 total) involving a retained lens fragment in which aggressive intraoperative manipulation, such as levitating posteriorly dislocated fragments up into the anterior chamber, was performed, a postoperative RRD developed. Of these 7 claims, 5 went on to trial or settled, and in all 7 cases, the final visual acuity was 20/200 or worse. In 1 of the 2 cases that went to a plaintiff verdict, the cataract surgeon had “some retinal training” but the jury still deemed this insufficient to handle the complication. 64 If this surgeon with partial retina surgical training was thought not to be sufficiently qualified in the legal case, this again calls in to question the ability to properly train surgeons on VR surgical techniques in a 2-day course and then expect them to be equally as competent as surgeons who completed a 2-year fellowship.
Understandably, the experience of the patient is important. Eliminating multiple surgeries, multiple risks of anesthesia, the costs of multiple days off from work, multiple postoperative visits, and the cost of 2 operations must be considered. However, these surgeries are not the norm, but are unique cases, requiring unique care. Coordinating multiple specialists, although burdensome, may be required, and what is safest for the patient to achieve the best anatomic and visual outcomes should be considered. Attempting to consolidate multiple surgical specialists to reduce these extraneous, nonclinical burdens risks subpar visual and anatomic consequences.
Conclusion
The desire to provide patients whose disease involves both the anterior and posterior segments of the vitreous with the best clinical outcome and fewest number of surgeries is the shared goal between non-VR and VR surgeons. When considering how to manage patients who require a pars plana vitrectomy, perhaps the best approach involves the anterior segment surgeons and VR surgeons working in tandem or in separate surgeries.
VR surgery has known intraoperative and postoperative complications. Management of these situations requires diagnostic and surgical skills that are currently acquired over a 2-year VR surgery fellowship. We believe it is highly unlikely that these skills can be acquired in a wet lab or weekend course. The American Society of Retina Specialists believes that non-VR surgeons without formal VR training in performing pars plana vitrectomy (more than anterior vitrectomy) may subject patients to intraoperative and postoperative risks, which they may not be able to detect nor manage, and thus we hesitate to acknowledge the validity of a “middle segment surgeon.” While we acknowledge that some situations may be appropriately handled in the absence of these elements discussed above—such as a limited anterior vitrectomy in the setting of ruptured capsular bag in cataract surgery—we believe the vast majority of surgery involving the posterior segment and vitreous cavity should be performed by VR fellowship–trained surgeons who can integrate intraoperative wide-field visualization, optimized fluidics, endoillumination, and specialized skills (eg, endolaser). In the absence of these elements, patient outcomes and safety may be compromised.
Footnotes
Ethical Approval
This article does not contain any studies with human or animal participants that would require ethical approval.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Matthew R. Starr is a consultant to AbbVie, Alimera Sciences, and Gyroscope Therapeutics.
Christina Y. Weng is a consultant to Alcon, Alimera Sciences, Regeneron, Allergan/AbbVie, Novartis, REGENXBIO, Opthea, DORC, Genentech, Iveric Bio, EyePoint, and Apellis, receives funding from AGTC, DRCR Retina Network, and Alimera Sciences, and has received research grant support from Springer Publishers.
Lejla Vajzovic is a consultant to AbbVie/Allergan, Alcon Laboratories, Inc. (also serving as a principal investigator), Alimera Sciences, Apellis, Bausch & Lomb, Beaver-Visitec International, Inc., BMC, Clearside Biomedical, Coherus Biosciences, DORC, Guidepoint, Gyroscope, Iveric Bio, Janssen/Johnson & Johnson, Novartis, Ocugen Inc., Ocular Therapeutix, Ocular Surgical, OcuTerra, Outlook Therapeutics, Regenxbio, and Roche/Genentech, and has received research grant support from AbbVie/Allergan, AGTC, Alcon Laboratories, Inc., Aldeyra, Apellis, Gyroscope, Heidelberg Engineering, Janssen/Johnson & Johnson, National Eye Institute, Novartis, Ocular Therapeutix, Regenxbio, and Roche/Genentech.
Kevin J. Blinder is a consultant to Bausch & Lomb, Regeneron, Iveric Bio, and Biogen, and Allergan, and has served as a speaker for Bausch & Lomb, Regeneron, Iveric Bio, and Biogen,
Judy E. Kim is a consultant to and serves on the advisory boards for Allergan/AbbVie, Amgen, Apellis, Bausch & Lomb, Clearside Biomedical, Coherus, Dutch Ophthalmic Research Center, Eyepoint, Genentech/Roche, Notal Vision, Outlook Therapeutics, and Regeneron.
J. Michael Jumper is a consultant to Long Bridge Medical, EyeBio, and EyeMacular Regeneration. He is a principal investigator for Genentech, AbbVie, and 4DMT.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.