
Abstract
Introduction
Vascular endothelial growth factor (VEGF) is a mediator of retinal and choroidal neovascularization, and anti-VEGF agents have been widely adopted to treat a growing number of ocular diseases.1–8 The 3 major anti-VEGF agents used in ophthalmology are aflibercept (Eylea; Regeneron), ranibizumab (Lucentis; Genentech), and bevacizumab (Avastin; Genentech). Bevacizumab was initially approved for treating colon cancer and was subsequently demonstrated to be effective in treating neovascular age-related macular degeneration (AMD).9–13 The use of bevacizumab for treating ocular conditions is off-label. Ranibizumab is an antiangiogenic monoclonal antibody fragment that is approved by the US Food and Drug Administration (FDA) for treating neovascular AMD, macular edema after retinal vein occlusions (RVOs), myopic choroidal neovascularization (CNV), diabetic macular edema (DME), and diabetic retinopathy.14–22 Aflibercept was approved by the FDA in 2011 for treating AMD, macular edema after RVOs, DME, and diabetic retinopathy.23–26
Studies have demonstrated that these 3 anti-VEGF agents exhibit similar effectiveness. In the case of neovascular AMD, the Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) showed that monthly bevacizumab injections resulted in noninferior visual acuity gains when compared with monthly ranibizumab, but it also found that ranibizumab demonstrated a greater decrease in central retina thickness than did bevacizumab. 27 Other studies have further supported the idea that bevacizumab, ranibizumab, and aflibercept are effective for achieving visual acuity gains in patients with neovascular AMD. However, similar to the observations from the CATT trials, studies have found other FDA-approved drugs to be superior to bevacizumab with respect to anatomic outcomes.28,29
Outside of neovascular AMD, some studies have found differences in effectiveness for treating DME. The Diabetic Retinopathy Clinical Research Network (DRCR) Retina Network Protocol T showed that aflibercept is superior to bevacizumab and ranibizumab after 1 or 2 years of treatment for patients who had initial visual acuity of 20/50 or worse. 30 However, there were no differences in mean change in visual acuity at 1 or 2 years among patients with better baseline visual acuity. 31 Visual acuity gains for patients with RVOs have also been found to be similar between the 3 agents in some studies, while other studies have found bevacizumab to fail to demonstrate noninferiority to ranibizumab when treating RVOs.32–34
In addition, DRCR Retina Network Protocol AC examined step therapy by comparing initial bevacizumab treatment with a switch to aflibercept only if certain criteria for improvement were not met, versus immediately starting aflibercept in eyes with visual acuity of 20/50 or worse. Protocol AC found no significant difference in visual outcomes between the different treatment algorithms, despite a large percentage of patients (70%) being switched to aflibercept within the 2-year study period. 35
Bevacizumab, ranibizumab, and aflibercept differ greatly in cost. Using 2015 wholesale acquisition costs, a 2.0 mg dose of aflibercept costs $1,850 and a 0.3 mg dose of ranibizumab costs $1,170, while a 1.25 mg dose of bevacizumab costs approximately $60. 36 Given the significant cost differences between these agents, there has been much debate in the ophthalmology community regarding the balance between cost-containment and medication selection for managing retinal diseases. In 2019, the Centers for Medicare & Medicaid Services (CMS) began allowing Medicare Advantage plans to implement step therapy for Part B drugs. 37 Notably, this policy only applies to Medicare Advantage plans, and Medicare Part B beneficiaries are not subject to fail-first therapy. Step therapy is a fail-first approach that requires demonstration of failure of bevacizumab treatment prior to initiating a switch to the more expensive ranibizumab or aflibercept. The definition of treatment failure is not always well defined and varies by ophthalmologist, but generally it is considered to be an inadequate treatment response or continued vision loss that may be accompanied by clinical biomarkers indicative of disease progression, which can vary based on the disease in question. 38 Step therapy has had uncertain implications on practitioner use patterns and supply chain considerations. 37
The goal of this research study was to analyze nationwide trends in anti-VEGF injection usage, specifically examining the use of different anti-VEGF agents and how step therapy policies may have impacted these trends over time. We hypothesized that step therapy policies would result in increased use of bevacizumab over aflibercept and ranibizumab over the study period. However, we also considered that among patients who are being treated through step therapy, the volume of bevacizumab may ultimately decrease due to eventual switching to branded drugs.
Methods
The study did not involve human subjects, and the data for this study were obtained from a publicly available database and did not contain personally identifiable information. As such, informed consent and institutional review board approval were not required.
Intravitreal anti-VEGF injection data from January 1, 2013 through December 31, 2021 were gathered from the publicly available Medicare Physician & Other Practitioners - by Provider and Service database. 39 This database contains information on services and procedures provided to Original Medicare (fee-for-service) Part B (Medical Insurance) beneficiaries by physicians and other healthcare professionals, and it does not include information for beneficiaries in Medicare Advantage or Medicaid. Medication data was identified using Current Procedural Terminology (CPT) codes specific for aflibercept (CPT code J0178), ranibizumab (CPT code J2778), and bevacizumab (CPT codes J9035/J3490/J3590), and did not include other agents. Using a previously described method of conversion, 40 medication units were converted to number of injections using the following ratios: for bevacizumab, 1 unit:1 injection; for ranibizumab, 4 units:1 injection; for aflibercept, 2 units:1 injection. Ophthalmologists were distinguished by their National Provider Identifier numbers.
For subgroup analysis, ophthalmologists were grouped according to high-volume injection usage in 2021, defined as those within the top 10% by injection volume for each medication and those injecting high volumes of anti-VEGF agents overall (without distinguishing between medications). This produced 4 high-volume injector groups of ophthalmologists, 1 for each anti-VEGF agent and for the overall (all medications) group.
Changes in treatment protocol between 2018 and 2021 were evaluated to assess the possible effects of step therapy. This time period was chosen in order to compare the year right before step therapy implementation with the most downstream year after step therapy implementation that was available in the dataset, in order to maximize our ability to identify the effects of step therapy implementation. For the purposes of time-based comparisons, statistical analysis was limited to ophthalmologists who administered at least one injection of bevacizumab, ranibizumab, and aflibercept. Paired t-tests were utilized to assess changes in injection volumes by ophthalmologists over time. Statistical analyses were conducted using R (version 4.1.1.; R Foundation for Statistical Computing).
Results
Descriptive Statistics
From 2013 through 2021, there were 26 602 816 total injections given to Medicare Part B beneficiaries, which were attributed to 4691 ophthalmologists (Figure 1A and 1B). The average Medicare standardized payment amount was stable throughout this period (Supplemental Figure 1).
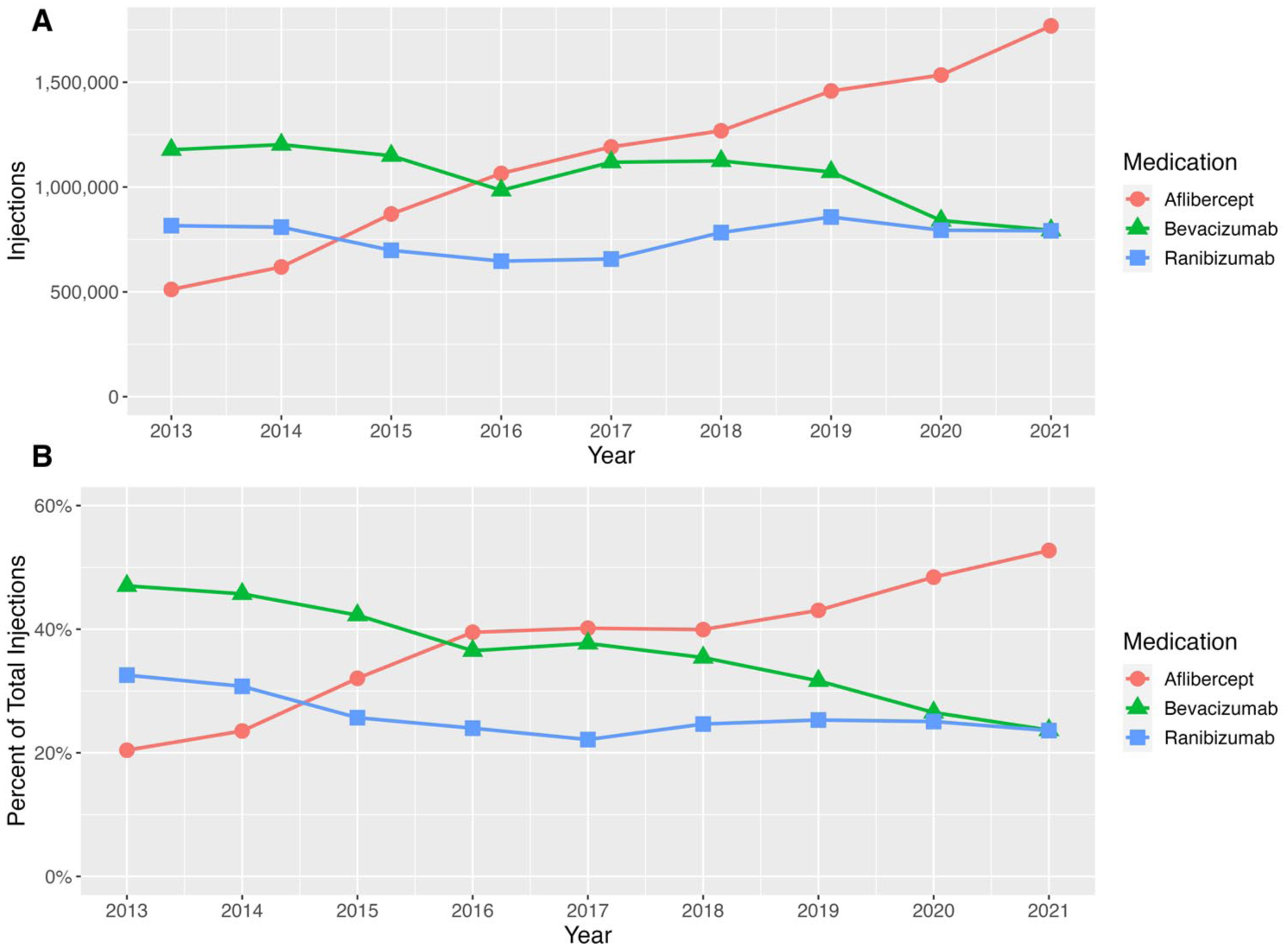
(A) Injection volume (expressed as total number of injections) by antivascular endothelial growth factor (anti-VEGF) medication given to US Medicare Part B beneficiaries from 2013 to 2021. (B) Injection proportion by anti-VEGF medication from 2013 to 2021.
On a year-to-year basis, the number of new injectors (ophthalmologists performing injections in a given year but who were not present in the database for the prior year) and number of injectors who stopped injecting (ophthalmologists absent from the database for a given year after being present in the prior year) were relatively stable throughout the study period (Supplemental Figure 2). For every year of the study period other than 2021, there were a greater number of new injectors than injectors who stopped injecting. In 2021 there were 1 768 598 aflibercept injections (52.7% of total injections), 794 018 bevacizumab injections (23.7% of total injections), and 791 427 ranibizumab injections (23.6% of total injections). Notably, in 2021, fewer ophthalmologists (n = 1440) administered ranibizumab injections compared to those who administered aflibercept injections (n = 3018) and those who administered bevacizumab injections (n = 2369).
High-Volume Injector Analysis
The top 10% of injectors (high-volume injectors) overall in 2021 accounted for a total of 1 157 106 injections (34.5% of total nationwide injections), with the proportions of nationwide injections of each medication varying between each high-volume injection group (Table 1). Notably, in 2021, in the high-volume aflibercept injector group, the percentage of aflibercept injections performed in 2021 (34.5% of total nationwide aflibercept injections) was lower compared to the percentage of ranibizumab injections performed by high-volume ranibizumab injectors (43.2% of total nationwide ranibizumab injections) and compared to the percentage of bevacizumab injections performed by high-volume bevacizumab injectors (41.2% of total nationwide bevacizumab injections). These trends were consistent throughout the study period.
Anti–Vascular Endothelial Growth Factor Injections Given by Ophthalmologists to US Medicare Part B Beneficiaries in 2021, by All Injectors Medications/All Injectors Group and by Each High-Volume Injectors Injector Group. a
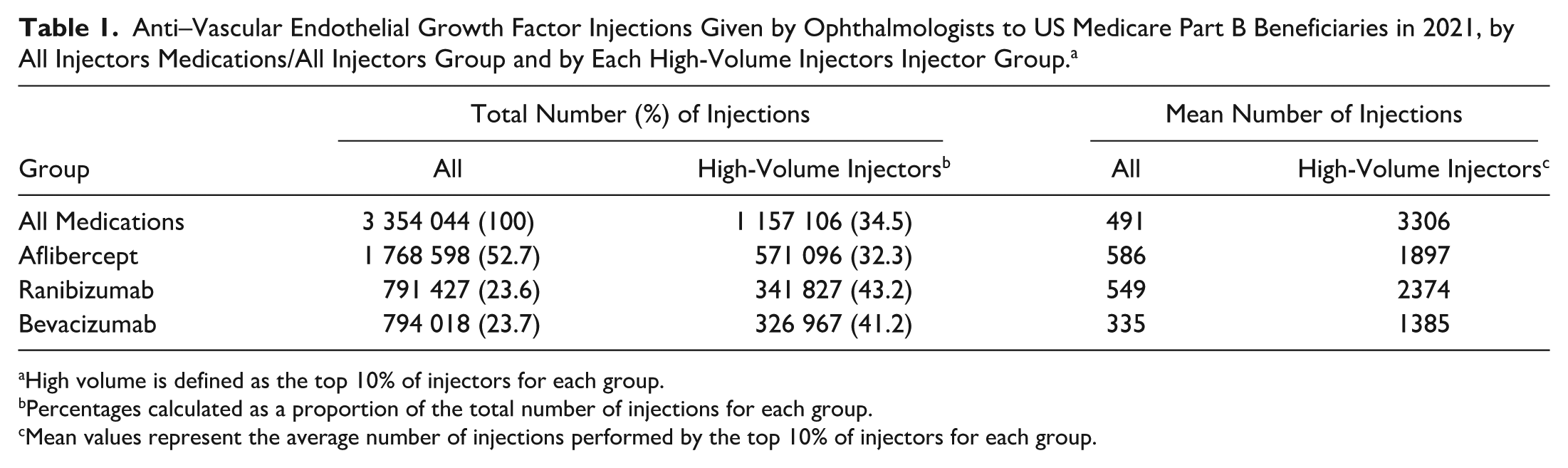
High volume is defined as the top 10% of injectors for each group.
Percentages calculated as a proportion of the total number of injections for each group.
Mean values represent the average number of injections performed by the top 10% of injectors for each group.
When assessing which ophthalmologists were in each high-volume injector group defined by medication, there were variable amounts of ophthalmologist overlap between any of these 3 groups and the medication-nonspecific (all medications) high-volume injector group (ie, overlap defined as the proportion of ophthalmologists in a high-volume injection group categorized by medication who were also in the all medication high-volume injection group). The high-volume ranibizumab group had the highest degree of overlap with the overall high-volume injection group (95.8% overlap, compared with 87.0% overlap between the high-volume aflibercept group and overall group, and 80.9% overlap between the high-volume bevacizumab group and overall group). In contrast, there were much lower levels of ophthalmologist overlap across each of the high-volume injector groups defined by each medication. In particular, 22.9% of high-volume ranibizumab injectors and 18.2% of high-volume bevacizumab injectors were also present in the high-volume aflibercept group, while only 4.2% of high-volume ranibizumab injectors were also present in the high-volume bevacizumab group. Similar associations were observed when the relative frequency of each medication’s use was assessed for differences across the high-volume injector groups (Figure 2).
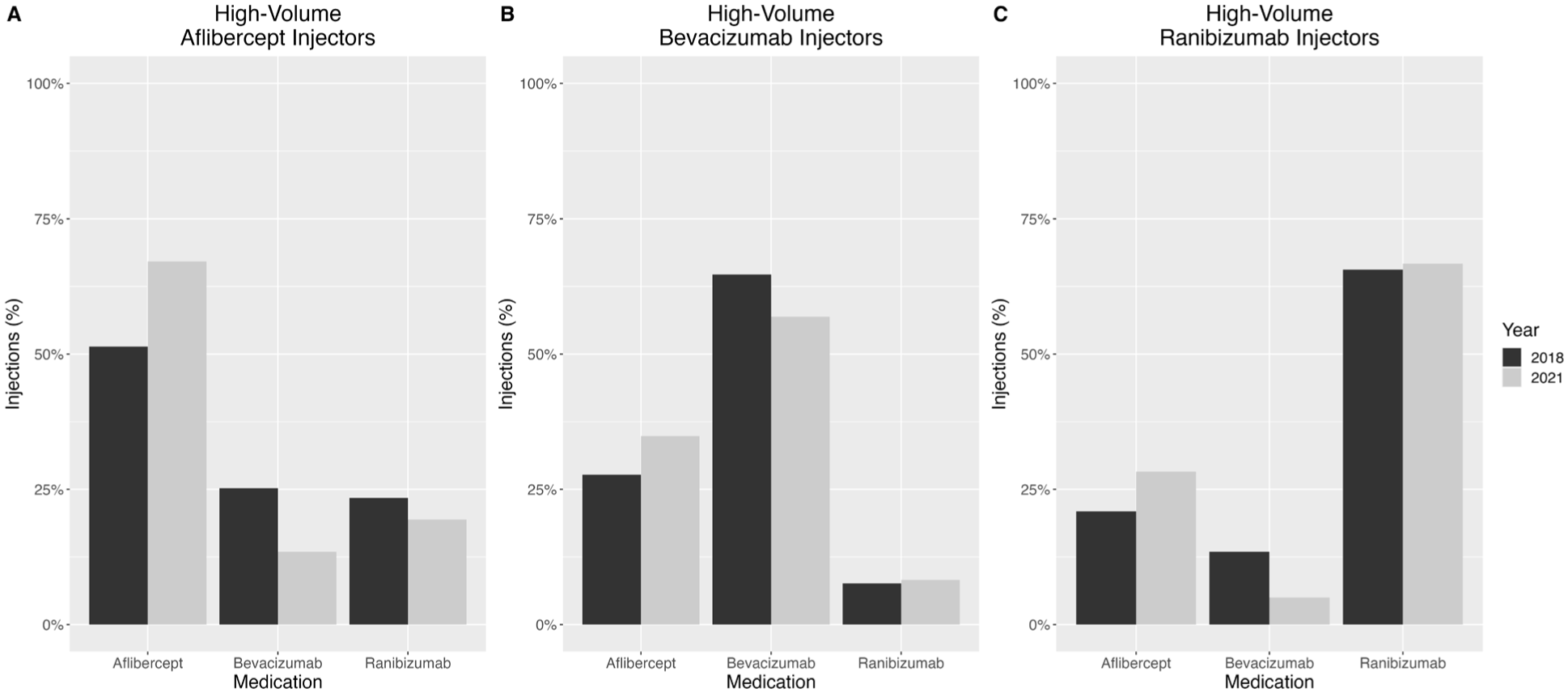
Frequency of medication use in 2018 and 2021 across different high-volume injector groups of ophthalmologists (defined as the top 10% of injectors) administering intravitreal antivascular endothelial growth factor injections to US Medicare Part B beneficiaries: (A) aflibercept, (B) bevacizumab, and (C) ranibizumab.
Step Therapy Analysis
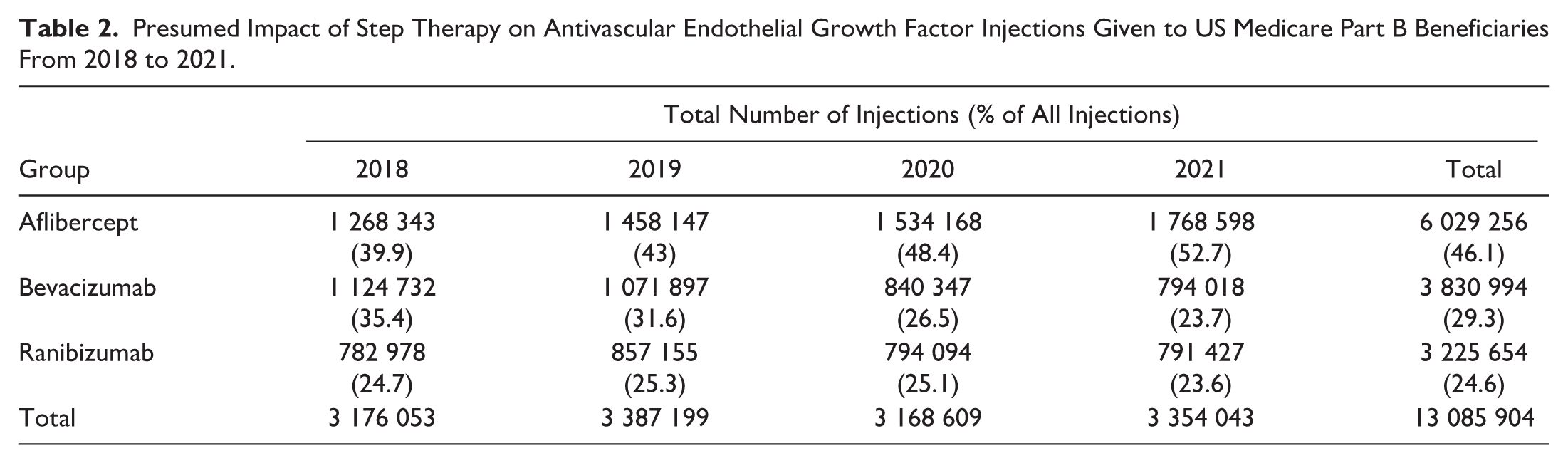
Changes to treatment protocol between 2018 and 2021 were evaluated to assess the possible effects of step therapy. From 2018 through 2021, there were 13 085 904 injections attributed to 4084 ophthalmologists (Table 2). Total injection volume was stable during this time. The relative usage of aflibercept increased by 32.0%, while bevacizumab’s relative usage decreased by 33.2% and ranibizumab’s relative usage decreased slightly by 4.3%. During this study period, all high-volume injector subgroups of ophthalmologists increased their aflibercept injection volume (all P < .0001 from 2018 to 2021), and both the high-volume aflibercept and high-volume ranibizumab injector groups, but not the high-volume bevacizumab injector group, decreased their bevacizumab injection volume (P < .05 for both groups from 2018 to 2021) (Table 3).
Presumed Impact of Step Therapy on AntiVascular Endothelial Growth Factor Injections Given to US Medicare Part B Beneficiaries From 2018 to 2021.
Presumed Impact of Step Therapy on AntiVascular Endothelial Growth Factor Injection Volume Among US Medicare Part B Beneficiaries Across Different High-Volume Subgroups From 2018 to 2021.
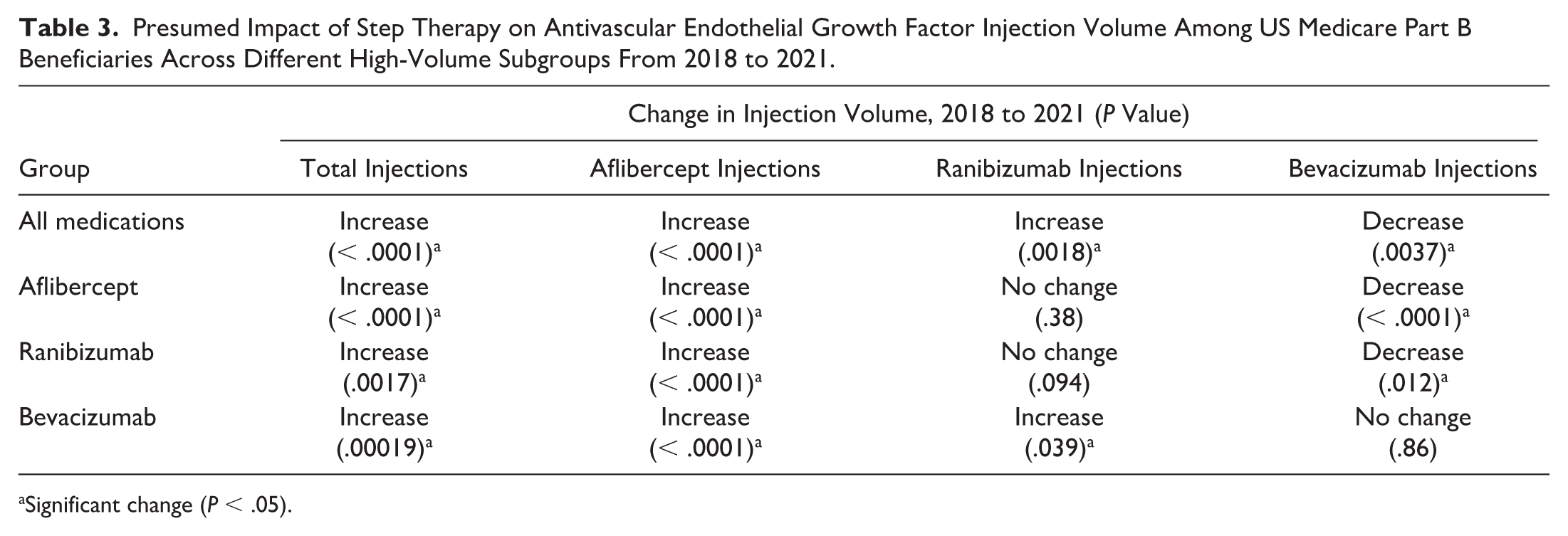
Significant change (P < .05).
Conclusions
During our study period of 2013 through 2021, there were more than 26 million anti-VEGF injections given by 4691 ophthalmologists. We identified a number of important trends in anti-VEGF injection usage, both by assessing usage over the period of 2013–2021 and by comparing data immediately before and after the implementation of step therapy. While other studies have examined anti-VEGF usage with earlier versions of Medicare Part B claims data (through 2015), to our knowledge this is the first study to utilize this data source to examine trends across a wider time range as well as before and after the implementation of step therapy (which first began in 2019) and during the COVID-19 pandemic. 40
The findings showed that a relatively small proportion (10%) of ophthalmologists accounted for a high proportion (34.5%) of the nationwide anti-VEGF injections, with a lower proportion of aflibercept injections being performed by high-volume aflibercept injectors (32.3% of nationwide aflibercept injections) when compared with the proportion of ranibizumab injections performed by high-volume ranibizumab injectors (43.2%) or proportion of bevacizumab injections performed by high-volume bevacizumab injectors (41.2%). These proportions and differences were consistent throughout the entire study period of 2013 through 2021. These findings, combined with the shift in aflibercept usage, which gradually increased from having a modest share of the total nationwide injections (20.4% of all anti-VEGF injections in 2013) to becoming a majority of the nationwide injections (52.7% of all anti-VEGF injections in 2021), support the idea that aflibercept has progressively become the most widely used of the 3 agents in our patient cohort of Medicare Part B beneficiaries. Additionally, the relatively stable proportion of aflibercept injections attributed to high-volume injectors suggests that nationwide increases in aflibercept usage could be attributed to volume changes among a broad set of ophthalmologists, rather than being solely driven by a high-volume injector subset of ophthalmologists.
Another interesting comparison that highlights aflibercept’s widespread use is the degree of enrichment (increase over and above the average injection volume) in injection volume between all ophthalmologists and the high-volume injector subgroups. The largest enrichment was seen with the high-volume ranibizumab injector group, which exhibited a 4.3-fold increase in the average number of annual ranibizumab injections compared to all ophthalmologists in 2021 (mean number of ranibizumab injections, 2374 vs 549). The high-volume bevacizumab injector group showed a similar enrichment in bevacizumab injection volume compared to all ophthalmologists in 2021 (4.1-fold increase; mean number of injections, 1385 vs 324), whereas high-volume aflibercept injectors showed a much more modest enrichment in aflibercept volume compared to all ophthalmologists in 2021 (3.2-fold increase; mean number of injections, 1897 vs 586). This further underscores the observation that, from 2013 to 2021, aflibercept evolved to become the most broadly used anti-VEGF agent across all ophthalmologists, with high-volume injectors playing less of a role in overall injection volume than for ranibizumab and bevacizumab.
Another interesting finding of this study was that fewer ophthalmologists overall chose ranibizumab for treatment in this cohort. In 2021, only 1440 ophthalmologists utilized ranibizumab injections, compared to 3018 ophthalmologists who utilized aflibercept injections and 2369 ophthalmologists who utilized bevacizumab injections. When the change in the number of ophthalmologists injecting each medication from 2013 to 2021 was assessed, aflibercept exhibited a 64% increase while bevacizumab showed a 16.9% decrease and ranibizumab demonstrated an 11.5% decrease. This change in the number of ophthalmologists injecting each medication mirrors the overall trends in medication usage. An additional observation was that each ophthalmologist tended to opt for primarily aflibercept and bevacizumab injections or aflibercept and ranibizumab injections, but it was much less common for an ophthalmologist to choose primarily ranibizumab and bevacizumab injections. These observations are consistent with previous studies examining Medicare Part B claims data from 2012 through 2015. 40
When comparing the period before step therapy versus after step therapy (2018 vs 2021), a few notable trends emerged. Contrary to what would be expected for step therapy’s intended effects, there was a significant increase in aflibercept injections and a decline in bevacizumab injections. The trend of increased aflibercept injections was mirrored by all the high-volume injector subgroups, and the decline in bevacizumab injections was reflected by 2 of the 3 high-volume injector subgroups, other than the high-volume bevacizumab group. While it is possible there may be a more narrowly defined subset of high-volume injectors who defy these trends, these findings reassert the possibility that there may not be fundamental differences in the trends that occur across all ophthalmologists versus only within high-volume subgroups.
There are a few notable limitations to this study. Our dataset comprised solely injection data for Medicare Part B beneficiaries, and as such does not offer insights into trends for patients with private insurance, Medicare Advantage, or Medicaid. Notably, Medicare Part B beneficiaries are not subject to fail-first therapy. It is also possible that some injections may be omitted from the CMS dataset entirely, but we have no reason to believe this is a significant characteristic of this dataset. An additional inherent limitation of the CMS dataset is that it does not differentiate retina specialists from all ophthalmologists. However, the high-volume injector groups are likely nearly entirely composed of retina specialists. Short of closely examining the training credentials of all 4691 ophthalmologists identified in this study, there is no reliable way to perfectly distinguish between retina specialists and non–retina specialists.
An additional limitation is that our study was only able to analyze the effects of step therapy on anti-VEGF usage changes for 2 full years of data following the initial implementation of step therapy. Given that medication choice is most relevant for patients being newly initiated on anti-VEGF injections, and a relatively small proportion of ophthalmologists’ patient panels fall into this category in any singular year (as opposed to the many patients who are continuing a preexisting anti-VEGF regimen), it is possible the full effects of step therapy may not yet be reflected in the available CMS data.
It is also possible that some clinicians use bevacizumab for initial treatment while awaiting insurance coverage for other drugs, and the Medicare database does not provide sufficient granularity to explore this possibility. An additional inherent limitation of the Medicare Part B claims dataset is that it fails to offer insight into the decisions made by individual physicians when deciding which medication to use for a given patient. Another important consideration is that there have been previously documented supply-chain issues with bevacizumab, and our data is unable to account for the possibility that these issues may be partially responsible for the decline in bevacizumab injections in 2020. 41 An additional contextual factor for this study is that the later time range of our dataset coincides with the height of the COVID-19 pandemic. While it is not immediately obvious how the COVID-19 pandemic may have impacted the usage patterns we identified, we cannot exclude the possibility that the pandemic may have had unforeseen effects on our dataset.
Despite these limitations, our dataset is the most optimal source of currently available information for assessing nationwide trends. Another interesting facet of anti-VEGF usage trends impacted by step therapy is the role of biosimilars and other newly approved drugs. The current landscape is certainly very different than that of the time range evaluated in this study, and therefore, this study may not be generalizable to current trends. Although the time range of our dataset does not provide the opportunity to evaluate the use of biosimilars (for example, ranibizumab-nuna [Byooviz; Samsung Bioepis Co., Ltd.] was the first ranibizumab biosimilar given FDA approval for neovascular AMD, in 2021), it would certainly be an interesting future direction to compare usage trends of aflibercept, ranibizumab, and bevacizumab with those of anti-VEGF biosimilars, for which the Medicare Part B dataset would be well-suited. 42 An additional future direction that could prove interesting would be to analyze the impact of fail-first requirements enacted by private insurers, though this would require a different source of data that may not be as readily available as the Medicare Part B database, and such an investigation would likely entail different considerations during data analysis.
Supplemental Material
sj-png-1-vrd-10.1177_24741264251383410 – Supplemental material for Trends in Anti–Vascular Endothelial Growth Factor Injections Among Medicare Part B Beneficiaries in 2013–2021 and the Step Therapy Era
Supplemental material, sj-png-1-vrd-10.1177_24741264251383410 for Trends in Anti–Vascular Endothelial Growth Factor Injections Among Medicare Part B Beneficiaries in 2013–2021 and the Step Therapy Era by John M. Bryan, Neil Sheth and Michael J. Heiferman in Journal of VitreoRetinal Diseases
Supplemental Material
sj-png-2-vrd-10.1177_24741264251383410 – Supplemental material for Trends in Anti–Vascular Endothelial Growth Factor Injections Among Medicare Part B Beneficiaries in 2013–2021 and the Step Therapy Era
Supplemental material, sj-png-2-vrd-10.1177_24741264251383410 for Trends in Anti–Vascular Endothelial Growth Factor Injections Among Medicare Part B Beneficiaries in 2013–2021 and the Step Therapy Era by John M. Bryan, Neil Sheth and Michael J. Heiferman in Journal of VitreoRetinal Diseases
Footnotes
Ethical Approval
Approval was not needed because of the study type (no human participants).
Statement of Informed Consent
This study did not involve human subjects and the data for this study was from a publicly available database without personally identifiable information. Consequently, informed consent is not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an unrestricted departmental grant from Research to Prevent Blindness.
Data Availability
The data used for this study is from a publicly available database on the CMS website. The authors are also able to provide the data used for this study upon request.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.