
Abstract
Introduction
Geographic atrophy (GA) represents an advanced stage of age-related macular degeneration and can result in significant central vision loss. 1 Dysregulation of the complement system, an essential component of the innate immune response, has been implicated in the development and progression of GA. 2 Recently, 2 drugs have received US Food and Drug Administration (FDA) approval for the management of GA: pegcetacoplan (Syfovre; Apellis Pharmaceuticals) and avacincaptad pegol (Izervay; Astellas Pharma Inc.). These treatments are designed to selectively inhibit complement components C3 and C5, respectively.3,4
Both medications are administered via a 0.1 mL intravitreal injection. An acute increase in intraocular pressure (IOP) may occur after any intravitreal injection, although the IOP usually normalizes to preinjection level within 30 minutes.5,6 However, the short-term course of IOP following intravitreal injection of these medications has not been evaluated, and an injection volume of 0.1 mL may cause higher initial IOP compared to an injection volume of 0.05 mL, the typical dose for the more common anti–vascular endothelial growth factor (anti-VEGF) medications. 7
Given that these treatments are relatively new, understanding their safety profile, including the potential for IOP spikes, is crucial. Therefore, the purpose of this study was to investigate the potential IOP increase after intravitreal injection of pegcetacoplan to optimize patient management and further explore the safety of this recently approved medication.
Methods
This single-center, prospective, interventional study evaluated a case series of patients with GA who received pegcetacoplan injections. The study adhered to the tenets of the Declaration of Helsinki and was conducted within the regulations set forth by the Health Insurance Portability and Accountability Act. Institutional review board approval was obtained from Wills Eye Hospital.
All patients with GA scheduled to receive pegcetacoplan injections at Mid Atlantic Retina and the Retina Service of Wills Eye Hospital were offered the opportunity to participate in this study. Patients who agreed to participate and were able to provide fully informed consent were included. Exclusion criteria included corneal pathology, a history of vitreoretinal surgery, cataract surgery within the past 90 days, or prior incisional glaucoma surgery. Eyes were prepared for injection with topical anesthetic drops and topical 5% iodine. In all patients, 0.1 mL of pegcetacoplan was administered in accordance with the manufacturer’s guidelines. IOP was measured using a handheld applanation tonometer just before the injection and immediately after the injection, as well as at 5, 10, 20, and 30 minutes postinjection. Research staff prepared the medications and performed the IOP measurements. Treating physicians were masked to their patients’ IOP readings. If measurement errors occurred with the handheld device, the IOP was measured with a Goldmann applanation tonometer. Baseline demographic data, history of glaucoma or ocular hypertension, use of IOP-lowering medication, and any ocular adverse events were recorded.
All data were analyzed using SPSS (SPSS Statistics version 29; IBM). Continuous variables were assessed using mean (±SD), while categorical variables were analyzed using proportions. A generalized estimating equation was employed to compare postinjection IOP values with preinjection IOP values. Linear regression analysis was performed to assess factors associated with higher IOP values postinjection. A P value of < .05 was considered statistically significant.
Results
A total of 51 patients (73 eyes) were included in the study. The mean (±SD) age of the patients was 80.5 ± 7.4 years (range, 66–95 years). Among the 51 patients, 44 (60.3%) were female. The mean (±SD) number of previous injections at the time of IOP measurements was 3.9 ± 2.2.
Six eyes of 5 patients (8.2% of eyes, 9.8% of patients) had a history of primary open-angle glaucoma (POAG). Among these 6 eyes, a median of 2 IOP-lowering medications (range, 1–3) were being administered at the time of pegcetacoplan injection.
The preinjection IOP in the total cohort was a mean (±SD) 15.3 ± 3.3 mm Hg (range, 7–24 mm Hg). Immediately following injection, the mean IOP increased to 40.2 ± 13.7 mm Hg (range, 15–76 mm Hg) (P < .001). The IOP values at subsequent time points gradually decreased, to a mean 31.3 ± 11.6 mm Hg (range, 14–76 mm Hg) at 5 minutes postinjection (P < .001), 23.2 ± 9.7 mm Hg (range, 9–74 mm Hg) at 10 minutes postinjection (P < .001), 19.6 ± 8.6 mm Hg (range, 8–70 mm Hg) at 20 minutes postinjection (P < .001), and 16.4 ± 4.9 mm Hg (range, 10–33 mm Hg) at 30 minutes postinjection (P = .05) (Figure 1).
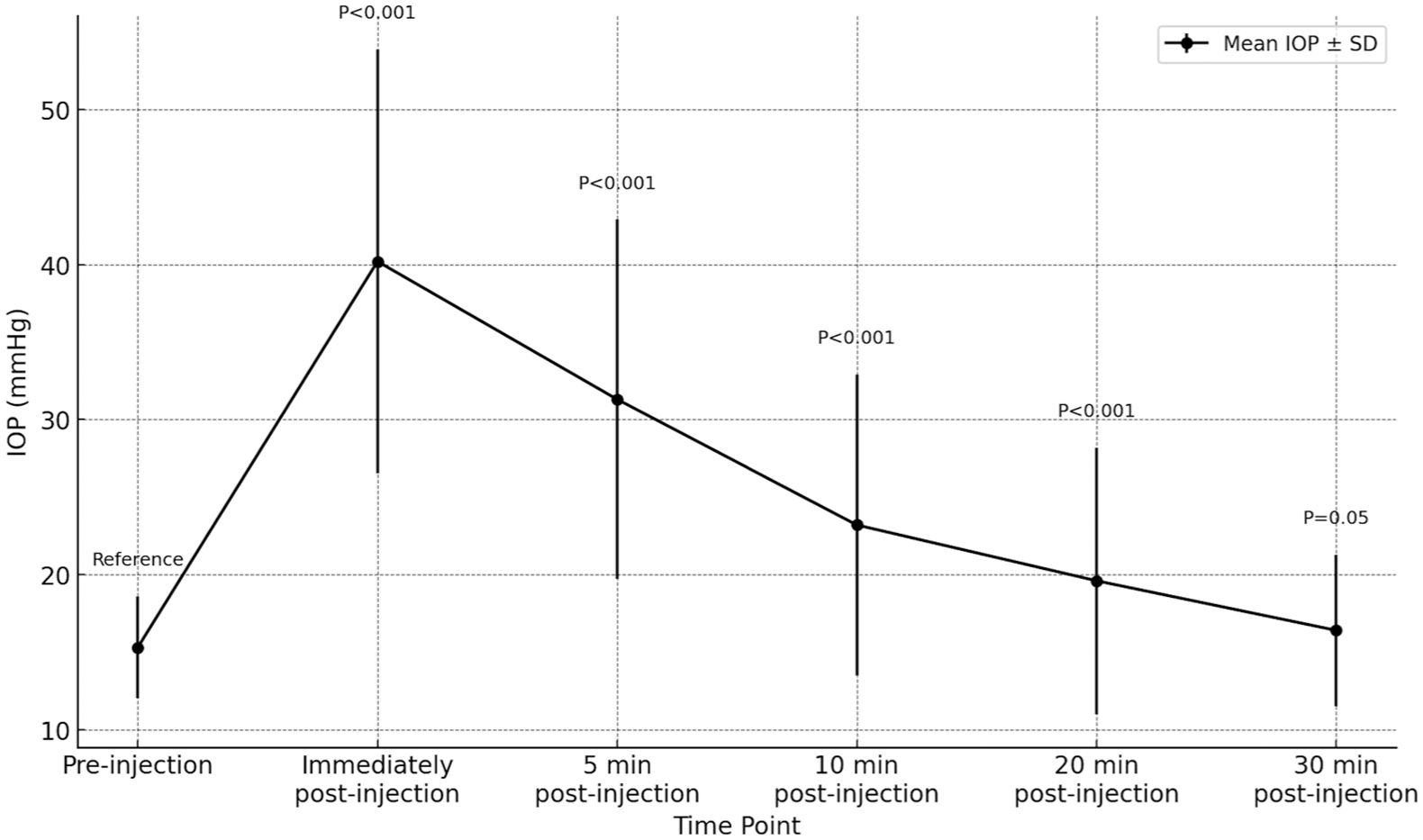
Changes in mean intraocular pressure (IOP) over time following intravitreal injection of pegcetacoplan in patients with geographic atrophy.
Only 1 patient, who had a history of POAG in both eyes and received injection of pegcetacoplan bilaterally, required IOP-lowering intervention within 30 minutes following injection. IOP in this patient’s left eye was 24 mm Hg preinjection and increased to 76 mm Hg, 76 mm Hg, 74 mm Hg, and 70 mm Hg immediately after injection, 5 minutes postinjection, 10 minutes postinjection, and 20 minutes postinjection, respectively. The patient’s left eye received an anterior chamber tap (fluid volume of 0.12 mL), and the IOP decreased to 11 mm Hg immediately following the procedure.
Five patients reported darkening of vision after injection. Of these, 4 patients experienced symptoms in both eyes following bilateral injections. One patient, however, received a unilateral injection. The duration of these episodes varied between a few seconds to 3–5 minutes and resolved without intervention. The median IOP in the eyes of these 5 patients was 64 mm Hg (range, 29–76 mm Hg) immediately after the injection, decreasing to 49 mm Hg (range, 23–76 mm Hg) within 5 minutes postinjection.
Linear regression analysis showed that a higher IOP at 30 minutes following injection was significantly associated with the preinjection IOP (β = 0.588, R2 = 0.160, P < .001) and also significantly associated with a history of glaucoma (β = 6.134, R2 = 0.122, P = .002). Associations of a higher IOP at 30 minutes postinjection with age, gender, and injection frequency were not significant (P = .279, P = .160, and P = .547, respectively). In multivariate linear regression analysis, both the preinjection IOP (P = .004) and a history of glaucoma (P = .019) remained significantly associated with a higher IOP at 30 minutes postinjection.
Similarly, linear regression analysis of associations with a higher IOP at 10 minutes postinjection revealed a significant association with the preinjection IOP (β = 1.423, R² = 0.233, P < .001) and also a significant association with a history of glaucoma (β = 16.542, R² = 0.222, P < .001). In the multivariate model, both preinjection IOP and a history of glaucoma remained significantly associated with a higher IOP at 10 minutes postinjection (both P < .001). These same regression analyses were used to assess associations with a higher IOP immediately following injection. The results did not reveal any significant factors.
Conclusions
With the advent of any novel therapy, ongoing safety studies are important to better understand the effects of these medications. Although other studies have assessed the effect of administering 0.05 mL of an anti-VEGF medication on IOP, the larger volume of 0.1 mL used for the complement inhibitors has the potential to cause greater IOP increases. This study provides insights into the IOP response following intravitreal injections of pegcetacoplan. Our findings demonstrated a significant increase in IOP immediately after injection of pegcetacoplan, followed by a gradual decrease in IOP over 30 minutes. Higher preinjection IOP and a history of glaucoma were significantly associated with higher IOP levels at 10 minutes and 30 minutes postinjection, but neither of these factors were associated with the immediate postinjection IOP. However, while significant associations were seen with some postinjection IOP values, not all of them were clinically significant.
Our results highlight an immediate increase in IOP following intravitreal injections of pegcetacoplan, with a mean IOP of 15.3 mm Hg at baseline, which increased to a mean IOP of 40.2 mm Hg immediately postinjection. Although the IOP gradually decreased over the subsequent 30 minutes, it remained elevated above baseline at all measured time points, with the final mean IOP being 16.4 mm Hg at 30 minutes postinjection. This pattern of transient IOP elevation following intravitreal anti-VEGF injections of 0.05 mL has been observed in numerous studies. Felfeli et al reported an IOP elevation from a mean IOP of 15.3 mm Hg at baseline to a mean of 41.6 mm Hg within 1 minute after an anti-VEGF injection, while El-Chehab et al reported a mean IOP of 46.4 mm Hg at 1 minute postinjection.8,9 Additionally, in a meta-analysis of 46 studies conducted by de Vries et al, the mean IOP increase immediately after an anti-VEGF injection was 23.41 mm Hg, which further increased by a mean of 2.51 mm Hg above baseline at 30 minutes postinjection. 10 Other observational studies have reported rates of sustained IOP, variably defined as an increase in IOP of 21 or 22 mm Hg or an elevation of ≥6 mm Hg from baseline on at least 2 consecutive visits, in 3–11% of patients receiving anti-VEGF injections.11–14 The average duration of IOP elevation is 30–60 minutes, although this can be prolonged in patients with POAG. 15 Although previous studies were conducted using anti-VEGF agents with a volume of 0.05 mL, pegcetacoplan requires a volume of 0.1 mL. Despite pegcetacoplan’s higher viscosity compared to anti-VEGF agents, viscosity does not appear to influence IOP outcomes. Instead, the main factor affecting IOP seems to be the volume of the injection. Allmendinger et al developed an instrumental setup to study IOP changes following intravitreal injections in enucleated porcine eyes and found no differences in IOP based on the viscosity of the injected solution. 16 They established that injection volumes of up to 100 µL could be safely administered in healthy porcine eyes before a significant exponential increase in IOP occurred. 16
In the majority of cases, IOP returned to near-baseline levels without the need for intervention. However, 1 eye (1.3%) of a patient with a history of POAG required an anterior chamber paracentesis to manage an extreme elevation in IOP 20 minutes after intravitreal injection. Moreover, 5 patients reported experiencing transient darkening of vision following injections (4 patients received bilateral injections and had darkening of vision in both eyes, and 1 patient received injection in 1 eye and had darkening of vision in the single treated eye); these symptoms resolved without intervention within a few seconds to 3–5 minutes. Our study identified a history of glaucoma and higher baseline IOP as risk factors for elevated IOP 30 minutes after injection. It is important to note that higher IOP refers to an elevated IOP as a continuous variable in the analysis, without a specific cutoff value, as the association was determined through linear regression. Consistent with our findings, studies by Kim et al and Good et al also found that eyes with preexisting glaucoma are at a higher risk for postinjection IOP spikes following anti-VEGF injections and may take longer to recover from these acute IOP elevations.5,17
In the phase 3 multicenter, randomized, double-masked, sham-controlled clinical trials that led to FDA approval of pegcetacoplan (OAKS and DERBY trials), ocular treatment-related adverse events related to IOP were not specifically described. 18 However, a few cases of ischemic optic neuropathy were observed. While the effect of an unanticipated drug-related predisposing factor cannot be ruled out, it is possible that reduced ocular blood flow secondary to the increased IOP observed following the injections may impact ocular perfusion. 7 In the phase 2 study, 1 patient (1.2%) in the pegcetacoplan monthly subgroup experienced a serious adverse event involving 2 episodes of IOP increase, and 1 patient (1.3%) in the every-other-month subgroup experienced an episode of IOP elevation. 19 Ocular treatment-emergent adverse events were reported in 7 eyes (8.1%) in the pegcetacoplan monthly subgroup and 8 eyes (10.1%) in the every-other-month subgroup in the phase 2 study. 19 The authors noted that overall pegcetacoplan administration had no long-term effects on IOP, as assessed by preinjection measurements, with postinjection IOP elevations of more than 30 mm Hg resolving spontaneously or with standard IOP-lowering procedures that included ocular massage, IOP-reducing medications, anterior chamber paracentesis, or a combination of treatment approaches. 19
In the phase 2/3 clinical trial for avacincaptad pegol, a transient elevation of the mean IOP was observed postinjection, which returned to near-baseline levels at the next follow-up visit and at the end of the study. 20 The mean preinjection IOP remained consistent from baseline to month 12 across all study arms. 20 There were no reported adverse events of glaucoma or ocular hypertension in the subjects receiving avacincaptad pegol. Specifically, ocular adverse events related to IOP increase occurred in 4 eyes (6.0%) in the avacincaptad pegol 2 mg group and in 16 eyes (19.3%) in the avacincaptad pegol 4 mg group, though there were no serious ocular adverse events. 20 In the studies with both drugs, glaucoma alone was not an exclusion factor. The only exclusions were eyes with uncontrolled glaucoma or eyes that had undergone surgical procedures, including the use of glaucoma drainage devices.
In contrast to the acute IOP elevation occurring immediately following an intravitreal injection, there is a lack of consensus on the long-term sequelae related to eye pressure changes over time with numerous injections. Using claims data, Cui et al identified 17 113 eyes without glaucoma that received intravitreal anti-VEGF injections, and those that received 14 or more injections at a 2-year follow-up or 20 or more injections at a 3-year follow-up had a higher likelihood of requiring IOP-lowering therapy or receiving a new diagnosis of glaucoma. 21 The mechanism of sustained IOP elevation with anti-VEGF agents is not well understood, although proposed mechanisms include obstruction of the conventional outflow pathway due to aggregates of protein, inflammation of the trabecular meshwork, mechanical trauma, and chronic angle closure.22–25 Additionally, endogenous VEGF expression in the trabecular meshwork has been identified as a paracrine regulator of conventional outflow facility. 26 Currently, it is unknown how the differences between complement inhibitors and anti-VEGF agents, along with the increased injection volume required for the administration of pegcetacoplan, could affect sustained IOP elevation.
While this study provides valuable data on the short-term IOP response following intravitreal injection of this novel therapy for GA, several limitations should be noted. The relatively small sample size limits the generalizability of the findings. Moreover, as a single-center study, there may be biases related to patient selection and management practices. The long-term sequelae of this drug with sustained IOP elevation remain unknown. Further studies are needed to elucidate the potential impact of repeated injections on IOP and glaucoma risk, and to identify which patients may be most susceptible to these outcomes. Future studies should aim to include larger, more diverse patient populations and more eyes with a history of ocular hypertension and glaucoma, and should explore the underlying mechanism driving the observed IOP changes and investigate potential strategies to mitigate these effects.
In conclusion, this study highlights that following the administration of intravitreal pegcetacoplan, there is a potential for significant acute IOP elevation, particularly in patients with higher baseline IOP and those with a history of glaucoma. IOP monitoring and personalized management strategies to ensure the safety of this therapy is important. Additional research is essential to fully understand the long-term impacts of this drug on IOP.
Footnotes
Ethical Approval
This study was approved by the Wills Eye Hospital Institutional Review Board.
Statement of Informed Consent
The Wills Eye Hospital Institutional Review Board approved this prospective study, including study documents and informed consent (IRB approval no. 2023-106).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Regillo is a consultant to 4D Molecular Therapeutics, Adverum, Alcon, Allergan, Annexon, Apellis, Aviceda, Clearside, Coherus, Cognition Therapeutics, EyePoint, Genentech, Inc., Iveric Bio, jCyte, Janssen, Kodiak Sciences, Lineage Cell Therapeutics, Merck, NGM Bio, Novartis, Ocugen, Ocuphire, OcuTerra, Opthea, Ray, Regeneron, Regenxbio, Stealth, Théa, and Zeiss, and has received research support from 4D Molecular Therapeutics, Adverum, Allergan, Annexon, Apellis, Astellas, EyePoint, Genentech, Inc., Gyroscope, Iveric Bio, Kodiak Sciences, Lineage Cell Therapeutics, NGM Bio, Novartis, Ocugen, Opthea, Regeneron, and Regenxbio.
Dr. Ho is a consultant to Apellis, Astellas, and Iveric, and has received research support from Apelis and Iveric.
Dr. Hsu is a consultant to Bausch & Lomb, Gyroscope Therapeutics, and Iveric Bio, and has received grant support from Aldeyra Therapeutics, Genentech/Roche, and Iveric Bio.
Dr. Yonekawa is a consultant to Alcon, Apellis, Bausch Health, Genentech, Pykus, and Versant Health, and has received grant support from Genentech/Roche, Kyowa Kirin, Ocugen, and Regeneron.
Dr. Orlin is on the advisory board for Genentech and Allergan.
Dr. Garg is a consultant to American Academy of Ophthalmology, Apellis, Bausch & Lomb, Boehringer Ingelheim, Merck Manual, and West Pharmaceuticals; has performed contracted research for Adverum, Alexion, American Academy of Ophthalmology, Annexon, Apellis, Astellas, Avonelle-X, Boehringer Ingelheim, Genentech, Gyroscope, Iveric Bio, Jefferson, KCRN, Kodiak, Lineage Cell Therapeutics, MUST Network, NGM Bio, Ocugen, Ocuterra, Opthea, Regeneron, RegenxBio, and Roche/Genentech; is on the advisory board for Coherus; and has received lecture fees from the Canadian Ophthalmological Society, Cole Eye Summit, Physicians’ Education Resource, and Retina Fellows Forum.
All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by the J. Arch McNamara, MD Fund for Retina Research and Education.