
Abstract
Introduction
Familial exudative vitreoretinopathy (FEVR) is a rare inherited retinal disease characterized by abnormal development of peripheral retinal vasculature, resulting in progressive ischemia. 1 Because the amount of peripheral retinal ischemia varies, patients with FEVR are at high risk of developing vision-threatening complications, such as secondary neovascularization, retinal detachment (RD), retinal folds, or retinal dysplasia. 2 Although major advancements have been made in identifying the pathologic mutations in certain genes linked to the development of FEVR, approximately half of FEVR cases harbor no identifiable causative gene mutation, making the diagnosis of FEVR still largely a clinical process. 3
Retinoschisis refers to the separation of retinal layers. 4 The location of separation can occur in either the macula or the periphery of the retina, or both, depending on the condition and any patient demographic characteristic.5,6 Retinoschisis is often associated with juvenile X-linked retinoschisis (JXLRS), a hereditary retinopathy caused by mutations in the RS1 gene, 6 which encodes an extracellular cell-to-cell adhesion protein called retinoschisin. 4 A defect in this protein has been attributed to formation of lamellar and cystic spaces within the separated layers of the retina. 4
We report a unique case series of patients with genetically confirmed FEVR caused by mutations in FZD4 who presented with schisis-like characteristics seen on optical coherence tomography (OCT) imaging in the setting of a retinal examination with anesthesia.
Methods
The clinical course and OCT images of the retina of 4 patients with schisis-like presentations of FEVR due to mutations in FZD4 were evaluated. The University of Miami Institutional Review Board approved this retrospective case review. The study adhered to the tenets of the Declaration of Helsinki.
Results
Case 1
A 5-year-old boy with a history of retinopathy of prematurity that did not require treatment was referred to a retina specialist by a pediatric ophthalmologist for suspected subretinal fluid in both eyes. The patient was born preterm at 31 weeks via an urgent cesarean section, initiated because the mother had either possible cholestasis of pregnancy or fatty liver disease in the setting of severe pregnancy-induced hypertension. The patient weighed 1632 grams at birth and has a twin sister who weighed 1630 grams at birth. At the time of birth, the patient required oxygen treatment in the neonatal intensive care unit for 2 months, due to prematurity, respiratory distress, apnea of prematurity, bradycardia, and hypoglycemia. Details regarding the clinical course of the patient’s twin sister were not available at the time of this retrospective review, and other family members were not screened due to the family’s preference.
Initial ophthalmic examination of the patient at age 5 years showed a visual acuity (VA) of 20/20 in both eyes. A retinal examination with the patient under anesthesia was then performed. Fundus examination showed an attached macula with temporal exudation, peripheral avascularity, atypical vasculature most prominent temporally in the right eye, and incomplete peripheral vascularization in the left eye. Echography revealed an axial length of 21.3 mm in the right eye and 23.5 mm in the left eye, and B-scan showed normal posterior contour with an attached retina in both eyes. Anterior segment examination findings and the intraocular pressure were unremarkable in both eyes. Fluorescein angiography (FA) showed incomplete peripheral vascularization in both eyes and temporal leakage and anomalous vessels in the right eye. OCT showed a normal foveal contour in both eyes, with temporal exudation and an extensive amount of inner retinal schisis in the inferior and superior temporal periphery of the right eye (Figure 1A). At this point, the patient’s right eye was treated with laser photocoagulation, intravitreal bevacizumab, and sub-Tenon triamcinolone acetonide.
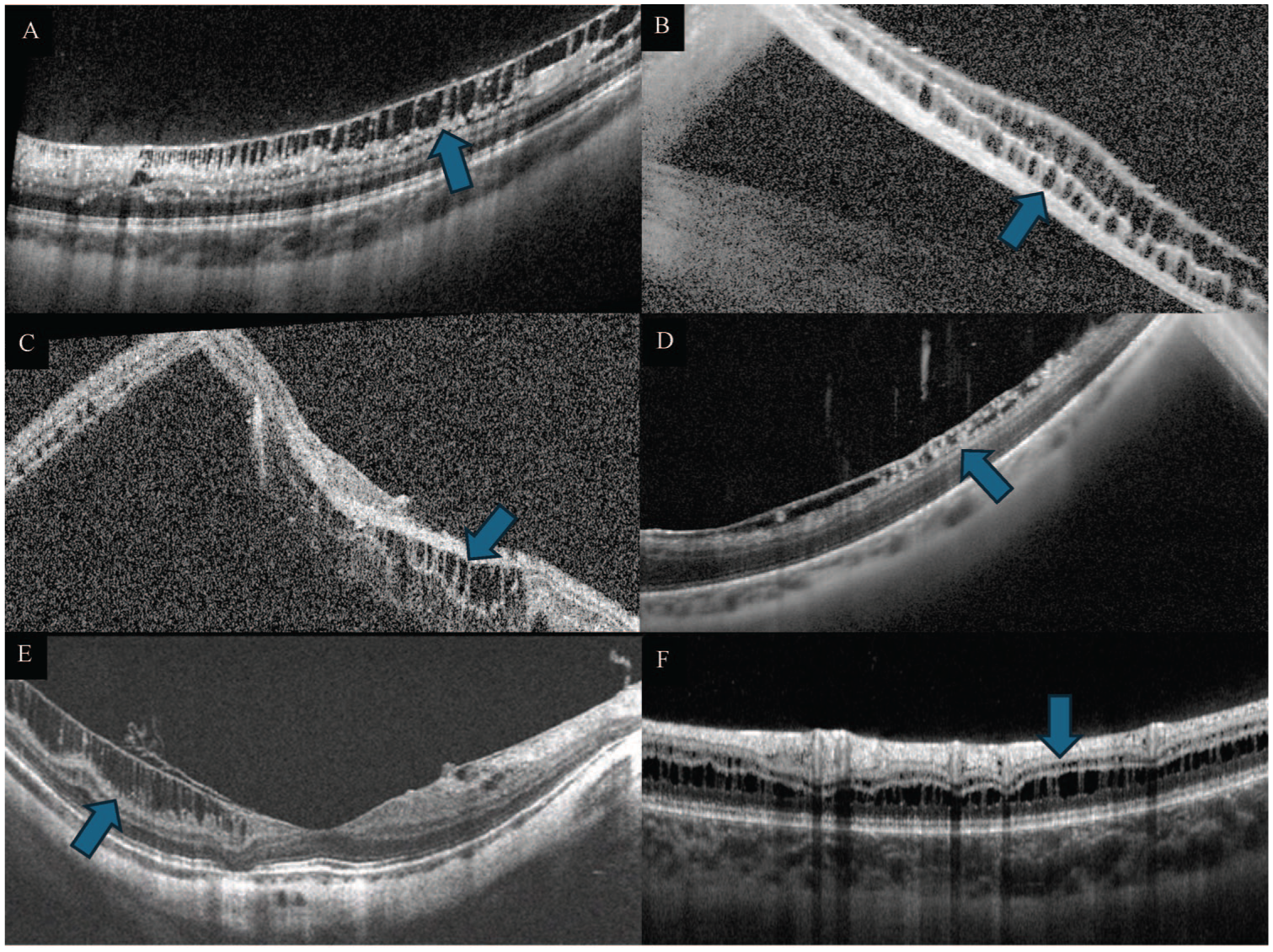
Optical coherence tomography (OCT) shows schisis (blue arrows) in the retinal periphery of the right eye in (A) case 1, the left eye in (B) case 2, the right eye in (C) case 3, and the left eye in (D) case 4. For comparison, OCT shows (E) inner maculoschisis in myopic traction maculopathy in a different patient, and (F) retinoschisis affecting the inner nuclear layer in a patient with juvenile X-linked retinoschisis.
A suspected diagnosis of inherited retinal disease prompted further investigation with genetic testing using the Invitae Inherited Retinal Disorders Panel (CLIA-certified laboratory testing; Invitae Corporation). Results revealed a heterozygous variant of unknown significance: c.1441A>C (p.Ile481Leu) in FZD4, a gene associated with autosomal-dominant FEVR. The patient’s twin sister was also genetically tested for inherited retinal disease, despite the fact that she lacked ophthalmic findings suggestive of clinical disease or symptoms at the time. Results revealed no variants in FZD4 in the twin sister.
Retinal examination of the patient under anesthesia and multimodal retinal imaging were repeated after 3 months and 6 months. At the follow-up fundus examinations, results still showed exudation, with evidence of leakage on FA, in the right eye. At both follow-up evaluations, the right eye was again treated with laser photocoagulation and an injection of intravitreal bevacizumab.
At the patient’s last follow-up appointment in the clinic, mild, pinpoint exudation on the superior arcades and peripherally in the right eye were noted on examination, and VA was 20/20 in both eyes. Therefore, the decision was made to observe. The patient continues to follow up with a pediatric ophthalmologist and a retina specialist.
Case 2
A 5-month-old girl, who was born full-term, was referred to a pediatric retina specialist for failure to fixate starting at age 3 months.
A retinal examination with the patient under anesthesia was performed. Fundus examination showed incomplete peripheral vascularization in both eyes. There was a rhegmatogenous RD with a retinal break temporally at 3:00 clock hours in the mid periphery and epiretinal proliferative vitreoretinopathy present circumferentially for 180 degrees pre-equatorially in the left eye. Echography revealed an axial length of 19.3 mm in the right eye and 19.7 mm in the left eye. B-scan showed normal posterior contour in the right eye and vitreous membranes in the left eye. Anterior segment examination revealed posterior nuclear opacity in the left eye, and the intraocular pressure was unremarkable in both eyes. FA showed 360 degrees of peripheral nonperfusion in both eyes. OCT showed peripheral schisis in the left eye (Figure 1B). At this point, laser photocoagulation was administered to the right eye, and pars plana vitrectomy (PPV) with membrane peel and placement of 1000 cc of silicone oil was performed in the left eye.
Genetic testing of this patient using the Invitae Inherited Retinal Disorders Panel revealed a heterozygous variant of unknown significance: c.359T>A (p.Met120Lys) in FZD4.
Four weeks later, the patient underwent a follow-up retinal examination under anesthesia. Due to the fact that FA showed focal areas of peripheral retinal nonperfusion posterior to the laser scars in the right eye and focal areas of retinal nonperfusion and leakage in the periphery along with disc staining in the left eye, laser photocoagulation was administered to the right eye. Intravitreal bevacizumab and sub-Tenon triamcinolone acetonide were administered to the left eye.
At the last follow-up appointment in the clinic, 4 years after the initial retinal examination under anesthesia, the patient’s VA was 20/30 in the right eye and light perception in the left eye. The patient continues to follow up with a pediatric ophthalmologist and a retina specialist.
Case 3
An 11-year-old boy, who was born full-term, presented to a pediatric retina specialist by referral from a community optometrist, with the chief presenting symptom being blurred vision in the right eye for 1 year. At the time of presentation, the patient’s VA was 20/400 in the right eye and 20/30 in the left eye.
A retinal examination with the patient under anesthesia was performed. Fundus examination showed a detached macula and temporal retinal periphery (consistent with a chronic, macula-off exudative RD with no identifiable breaks), vascular straightening, and incomplete retinal vascularization posteriorly in the right eye. Fundus examination of the left eye showed vascular straightening and incomplete retinal vascularization. Echography revealed an axial length of 23.3 mm in the right eye and 24.5 mm in the left eye. B-scan showed vitreous membranes in both eyes. Anterior segment examination findings and the intraocular pressure were unremarkable in both eyes. FA showed posterior nonperfusion in both eyes. OCT showed peripheral schisis in the right eye (Figure 1C). At this point, surgery was indicated, and the patient underwent a scleral buckle procedure and PPV with drainage of exudative fluid and a silicone oil tamponade in the right eye.
Inherited retinal disease testing with the Invitae Inherited Retinal Disorders Panel revealed a heterozygous variant of unknown significance: c.359T>A (p.Met120Lys) in FZD4, which is identical to the FZD4 mutation found in case 2.
The patient underwent cataract extraction with an intraocular lens implant and silicone oil exchange in the right eye. At the patient’s last follow-up appointment in the clinic, the VA was 20/100 in the right eye and 20/20 in the left eye. The intraocular pressure was unremarkable in both eyes. The patient continues to follow up with a pediatric retina specialist and a pediatric glaucoma specialist.
Case 4
A 41-year-old woman presented to a retina specialist by referral for retinal evaluation due to a suspected diagnosis of FEVR with possible vitreomacular traction and epiretinal membrane in the left eye. At the time of presentation, the patient’s VA was 20/20 in the right eye and 20/25 in the left eye.
A retinal examination with the patient under anesthesia was performed in order to treat both eyes simultaneously, which was the patient’s preference after not being able to tolerate laser photocoagulation in a clinical setting. Fundus examination showed peripheral exudates in both eyes and inferior neovascularization in the left eye. Anterior segment examination findings and the intraocular pressure were unremarkable in both eyes. FA showed peripheral ischemia with supernumerary vessels in both eyes and mild central macular edema (CME) in the left eye. OCT showed peripheral schisis in the left eye (Figure 1D). At this point, laser photocoagulation and sub-Tenon triamcinolone acetonide were administered in both eyes, and intravitreal bevacizumab was administered in the left eye.
Inherited retinal disease testing with the Invitae Inherited Retinal Disorders Panel revealed a heterozygous variant of unknown significance: c.1499C>G (p.Thr500Ser) in FZD4.
One month later, the patient was treated with intravitreal bevacizumab for persistent exudative fluid leakage, as demonstrated on FA, and worsening CME due to worsening traction in the left eye. Due to the patient’s preference for treatment with injections rather than surgical intervention, the patient has continued to undergo treatment with intravitreal bevacizumab, and CME has remained stable with good vision.
At the patient’s last follow-up appointment in the clinic, the VA was 20/20 in the right eye and 20/30 in the left eye. The patient continues to follow up with a retina specialist.
Conclusions
We report a unique case series of patients with FEVR caused by mutations in FZD4 and schisis-like presentations as revealed on OCT scans. Although FEVR is known to manifest with peripheral avascularity, the additional schisis-like presentation in our case series is rare. The nature of the schisis observed in our cases has similarities to and differences from schisis observed in other retinal conditions and could be a product of abnormalities in FZD4.
It is interesting to note that our patients had a unilateral schisis-like presentation, given that they occurred in the setting of FEVR, an inherited retinal disease that is thought to be bilateral. 7 Disease asymmetry in patients with FEVR has been reported 7 and might apply to the concept of schisis-like presentation of FEVR as well.
The exact relationship between FEVR and traditional retinoschisis is unclear, but indirect links between the products of NDP and FZD4 8 may explain the schisis-like presentation seen in our cases. Ke et al report that NDP products bind with the extracellular cysteine-rich domain of the FZD4 receptor and with the beta-propeller of low-density lipoprotein receptor (LDLR) 5/6, which activates canonical β-catenin signaling. 9 This signaling contributes not only to eye development but also to proper retinal angiogenesis. 9 LDLR promotes endocytosis of cholesterol-rich LDL and maintains lipid levels in the plasma membrane. 10 Mutations in the LDLR5 receptor and FZD4 can cause FEVR. 8 Therefore, mutations in either or both FZD4 and NDP could influence downstream actions, possibly resulting in decreased cell–cell adhesion in layers of the retina that manifests uniquely as FEVR with a schisis-like presentation. Also, there is a possibility that more severely abnormal vessels or neovascularization in 1 eye compared to the other eye (as in our cases) could have caused unusual or more severe traction from the posterior hyaloid, resulting in the schisis-like presentation of the right eye. Due to its propensity for causing exudation, mutations in FZD4 could result in cytokine release and subsequent hyaloid contraction that produces the schisis-like characteristics seen in our cases. Furthermore, it is possible that fibrovascular membranes in FEVR could cause schisis in a manner similar to that seen in retinopathy of prematurity, although those cases have been associated with JXLRS 11 and vitreous hemorrhage, 12 which were not present in our patients.
Parolini et al described a classification system for a similar concept addressing schisis in the macula from traction in the setting of myopia.13,14 Although our cases did not have an abnormal macula or foveal contour due to myopia, the schisis-like presentation of the inner retinal layers in the retinal periphery on OCT imaging was similar to that of inner maculoschisis, being described by Parolini et al 13 as a thickening of the inner retinal layers in a column-like structure, at different levels, from the inner nuclear layer (INL) to the internal limiting membrane (ILM) (Figure 1E). Moreover, Parolini et al 13 reported that the ILM can be detached from the nerve fiber layer (NFL) and connected to it with a column-like structure in some cases (Figure 1E). Overall, our cases demonstrate some similarity in the form of thickening of the inner retinal layers in a column-like structure affecting the ILM, NFL, and ganglion cell layer (GCL), but are also different because they mostly spare the INL, are located in the peripheral retina rather than the macula, and occur in the setting of FEVR rather than myopia.
Retinoschisis associated with JXLRS and the schisis-like presentation in our cases are also distinct entities. Genetically, JXLRS is associated with mutations in RS1; none of our patients had an RS1 mutation. Phenotypically, although there is a broad spectrum of presentations of JXLRS, Rao et al categorized them into 4 presentation types that all include foveal schisis, 15 which is not consistent with our patients’ schisis-like presentations in solely the peripheral retina. Also, retinoschisis associated with JXLRS has been described to affect the NFL, GCL, INL, outer plexiform layer, and outer nuclear layer. 16 In contrast, Gregori et al reported that retinoschisis in JXLRS tends to occur most often in the INL, 17 and Georgiou et al reported that intraretinal cysts in JXLRS are usually found in numerous quantities in the INL specifically. 16 In a study by Nakajima et al, OCT imaging showed that peripheral retinoschisis and cystoid changes in patients with JXLRS occurred in the INL in 44% of eyes (Figure 1F). 18 It is possible that the schisis-like presentation analyzed by OCT in one of our cases (case 3) could be classified as similar to JXLRS, in that the retinal layers affected include the INL. However, overall, the schisis-like presentation in our cases is different because, although the presenting characteristics were cyst-like, peripheral, and located in the inner retina, the NFL and GCL were specifically affected, sparing the INL. Therefore, the schisis-like presentation in our cases seems to affect more superficial inner retinal layers, such as the NFL and GCL, and can be best visualized with OCT imaging.
It is also important to note that in the setting of an RD in a pediatric patient, inner retinal schisis could result from traction due to proliferative vitreoretinopathy (PVR). However, no clear break or PVR membrane was identified intraoperatively.
Regarding treatment, the standard of care for FEVR is laser photocoagulation to ablate peripheral avascular retina and inhibit neovascularization and exudative fluid leakage evident on FA. 19 Because the pathogenesis of FEVR has been linked to abnormalities in the Wnt receptor:β-catenin pathway, which upregulates vascular endothelial growth factor (VEGF), anti-VEGF agents, such as intravitreal bevacizumab, have been shown to help treat this disease. 20 When discussing treatment options with FEVR patients and families, it is important to emphasize that it is a gradual process, requiring compliance with multiple retinal examinations under anesthesia for consideration of possible serial treatments with intravitreal injections and laser photocoagulation over a period of months and requiring surveillance for life. Imaging with fundus photography, OCT, and FA is essential to assess disease activity and decide whether additional treatment should be performed. RD can occur if both inner and outer retinal holes develop in the schisis cavity, allowing communication from the vitreous cavity into the subretinal space, and can necessitate treatment. 21 Fortunately, our patients’ schisis-like presentations on follow-up examination were found to be asymptomatic, nonprogressive, not bullous, and lacking retinal holes. It is unclear how the pathologic progression in our cases will behave in the long-term. Therefore, continued care with a pediatric retina specialist has been recommended to the patients and their family members.
Patients with genetically confirmed FEVR due to mutations in FZD4 can also possess a distinctly unilateral schisis-like presentation that may not be apparent clinically. This schisis-like presentation appears to be similar to that seen in other retinal disorders with schisis, and yet there are differences, such as myopic traction maculopathy and JXLRS, making it a distinct entity. In addition to genetic testing and FA, which usually guide diagnosis and treatment, providers should consider peripheral OCT imaging in these patients.
Footnotes
Acknowledgements
The authors thank Giselle de Oliveira, BFA and senior ophthalmic photographer, for providing the images.
Ethical Approval
The University of Miami Institutional Review Board approved this study, and it adheres to the tenets of the Declaration of Helsinki. Pertinent information about patients’ medical and ocular history are included, but identifying information was excluded.
Statement of Informed Consent
Written consent to publish this case series has been obtained; however, this case series does not contain any personal identifying information.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Berrocal is a consultant for Alcon, Allergan, Zeiss, Dutch Ophthalmic Research Center, Novartis, ProQR, and Oculus. All other authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was supported in part by an unrestricted grant from Research to Prevent Blindness (grant P30EY014801) in New York, New York, from the NIH Center Core in Bethesda, Maryland, and from the Department of Defense (grant W81XWH-09-1-0675) in Washington, DC. The sponsors or funding organizations had no role in the design or conduct of this study.
Data Availability
Data sharing is not applicable to this case report, as no datasets were created or analyzed.