
Abstract
Keywords
Introduction
Typical optic nerve colobomas are part of a spectrum of congenital cavitary optic disc anomalies in which the optic fissure does not achieve complete closure at the optic disc.1,2 The incidence of optic disc malformations is estimated to be around 8.9 per 100 000 live births. 3 The most common presenting signs include decreased visual acuity, amblyopia, strabismus, and nystagmus.1,3 Visual deficiency may occur owing to decreased central visual acuity or various visual field defects. 2 Patients with optic nerve colobomas may exhibit differing levels of visual function depending on the severity of the anatomic defect and the presence of other factors such as refractive amblyopia.4,5
Cavitary disc maculopathy is a clinical entity characterized by the accumulation of fluid in the intraretinal and subretinal spaces, associated with anomalies of the blood–retinal barrier at the level of the optic disc. It may arise secondary to congenital or acquired conditions. 6 In some cases, it may occur owing to an abnormal connection between the subretinal and subarachnoid spaces. 6 Macular retinoschisis may be present in some patients. 7 The etiology of the subretinal fluid in patients with cavitary disc maculopathy remains unclear. Proteomic analysis of the submacular fluid in affected patients has suggested a vitreous origin. 8 Conversely, another possible source may be cerebrospinal fluid (CSF) leakage through a defect in the optic nerve head, allowing CSF to dissect into the subretinal space. 7
Previously reported treatments for cavitary disc maculopathy include oral corticosteroids, oral acetazolamide, laser photocoagulation, pars plana vitrectomy (PPV), and macular buckling procedures.7,9–14 Despite these treatment options, cavitary disc maculopathy carries a guarded prognosis, often limited by recurrence.9,10,12,15 We present a case of cavitary disc maculopathy managed with primary optic nerve sheath fenestration followed by juxtapapillary laser photocoagulation.
Case Report
A 20-year-old Hispanic woman without systemic illness was referred for ophthalmologic evaluation owing to a retinal detachment in her right eye. She reported a long-standing history of poor vision in the same eye since childhood. She denied experiencing flashes, floaters, or pain in either eye. Her ocular history was remarkable only for deep refractive amblyopia. She denied any previous ocular surgeries, prescribed medications, or recent eye trauma.
On physical examination, the patient’s best-corrected visual acuity was 20/400 in the right eye and 20/20 in the left eye. Intraocular pressures were within normal limits in both eyes, and full ocular ductions were present. Pupillary evaluation showed an afferent pupillary defect in the right eye. Anterior segment examination did not reveal any abnormalities such as cataracts, colobomas, or iris rubeosis. On dilated fundus examination, the right eye revealed a colobomatous optic disc with peripapillary atrophy and an abnormal blood vessel course (Figure 1A). A complete serous retinal detachment was observed, accompanied by secondary peripheral retinal neovascularization and peripheral vitreous hemorrhage. The serous detachment extended to the colobomatous optic nerve, where the retina appeared slightly atrophic. Fundus examination of the left eye was unremarkable. Macular spectral-domain optical coherence tomography (SD-OCT) of the right eye revealed subretinal fluid and a macular detachment (Figure 1B), while the SD-OCT of the left eye was unremarkable.
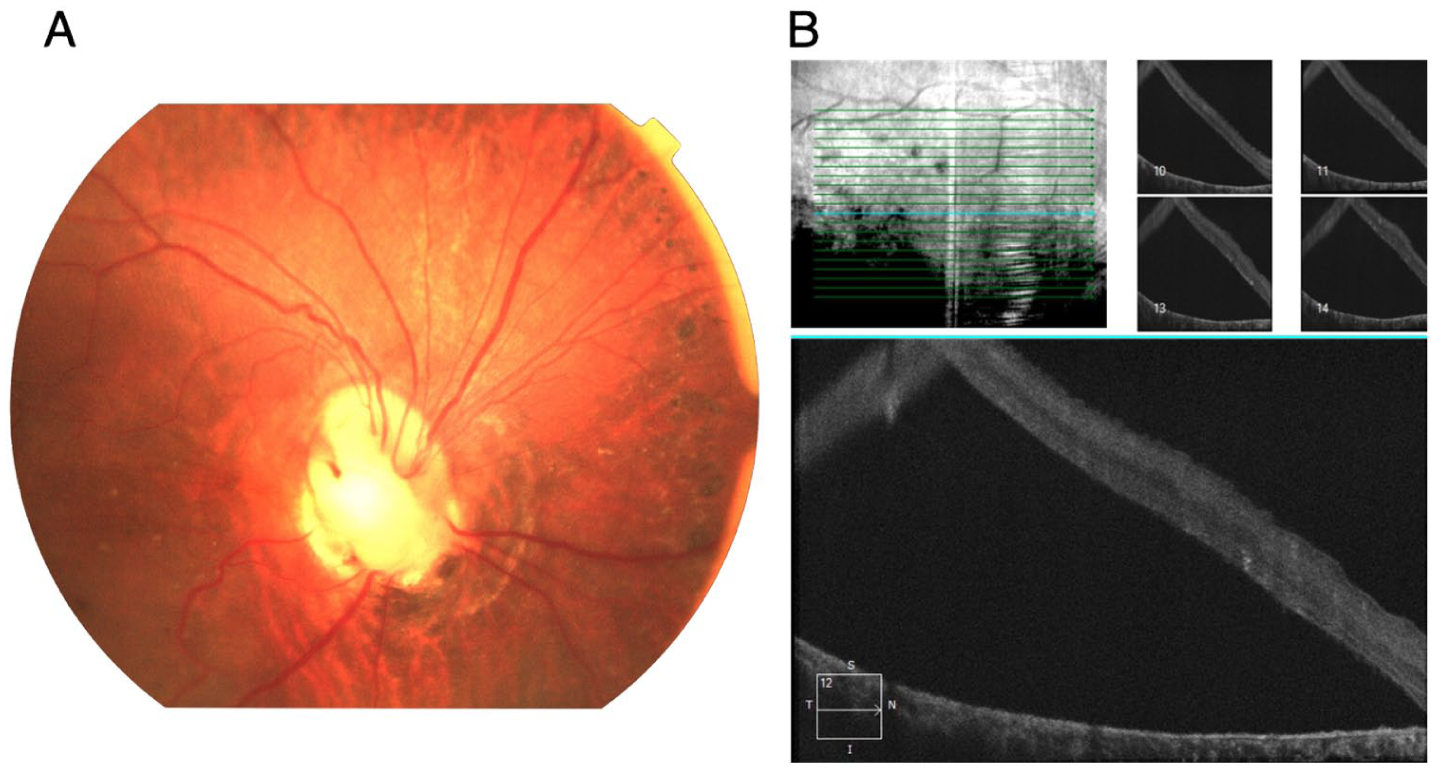
Clinical evaluation of a patient with cavitary disc maculopathy. (A) Fundus photograph of the posterior pole of the right eye demonstrates a colobomatous optic disc with irregular borders and cup, and a blunted foveal reflex. (B) Macular spectral-domain optical coherence tomography of the right eye shows serous retinal detachment.
After initial evaluation, the patient was observed for 3 months to assess for spontaneous resolution of the serous retinal detachment. As no improvement was observed, she subsequently underwent primary optic nerve sheath fenestration of the right eye using the medial transconjunctival approach described by Galbraith and Sullivan. No postoperative complications occurred. Eight weeks after optic nerve sheath fenestration, a significant decrease in subretinal fluid was observed (Figure 2). Twelve weeks following optic nerve sheath fenestration, diode laser photocoagulation was applied to the juxtapapillary retina to prevent further fluid migration and reaccumulation into the subretinal space. Four weeks after the laser barricade, complete resolution of the serous retinal detachment was achieved (Figure 3). The patient’s visual acuity remained stable throughout. At 1-year follow-up, the retina remained attached with no recurrence of fluid accumulation, and visual acuity was unchanged. The left eye demonstrated a normal macular contour and optic disc appearance (Figure 4).
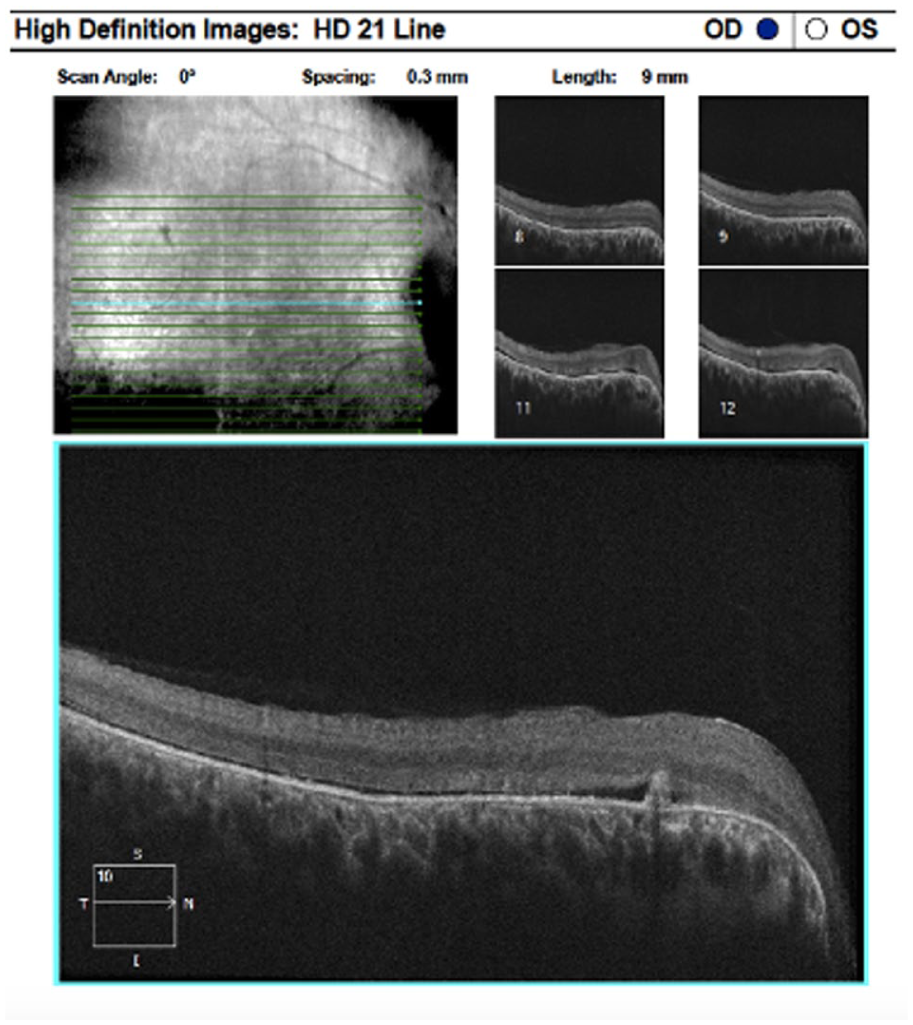
Macular spectral-domain optic coherence tomography of the right eye 8 weeks after optic nerve sheath fenestration demonstrates a significant reduction in subretinal fluid, with only a trace amount remaining.
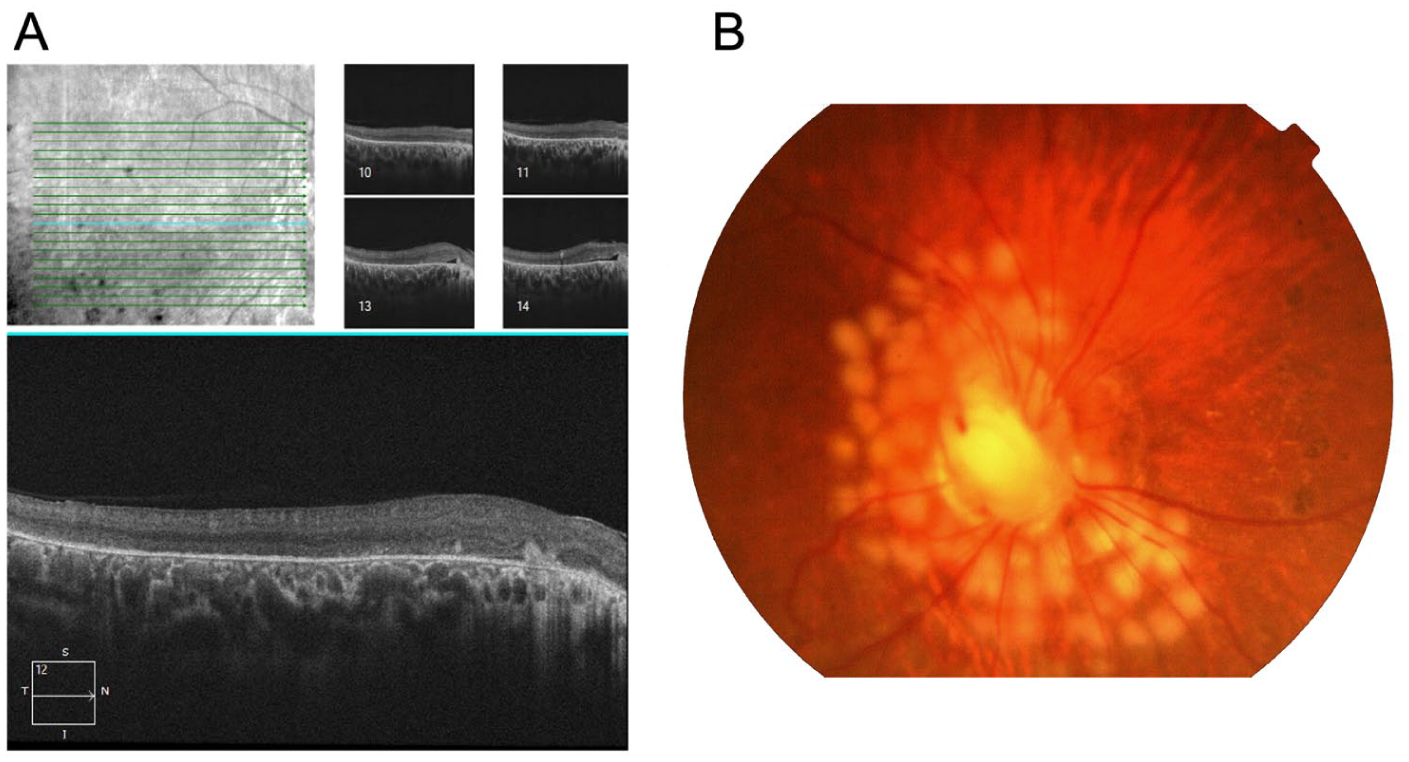
(A) Macular spectral-domain optic coherence tomography performed 16 weeks after optic nerve sheath fenestration (4 weeks after diode laser photocoagulation) shows near-complete resolution of subretinal fluid. (B) Fundus photograph of the right eye taken 16 weeks after optic nerve sheath fenestration shows juxtapapillary laser photocoagulation.
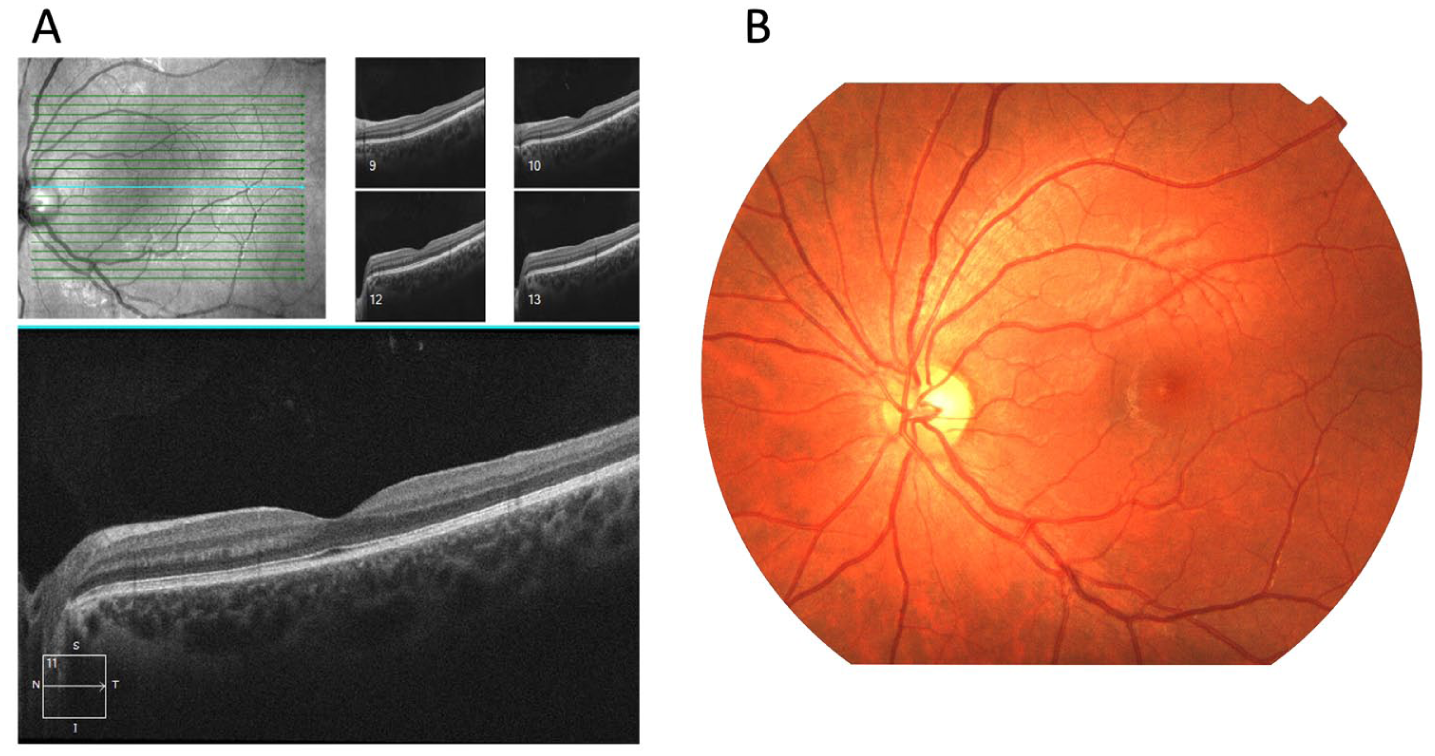
(A) Macular spectral-domain optic nerve sheath fenestration and (B) fundus photograph of the left eye, included for comparison, show normal macular contour and optic disc appearance.
Conclusions
Historically, the management of cavitary disc maculopathy has included both nonsurgical options, such as diuretics, and invasive intraocular or periocular surgeries. Some of the current surgical techniques include PPV with tamponade, ILM peeling and flap techniques, and PPV with tamponade in conjunction with juxtapapillary laser photocoagulation.16–18 To our knowledge, this is 1 of the few reported cases of cavitary disc maculopathy treated with optic nerve sheath fenestration as a primary treatment modality. 19 Previous studies have shown the utility of optic nerve sheath fenestration as a secondary intervention in cases refractory to intraocular surgery. 14 In our patient, 12 weeks after fenestration, there was a significant decrease in subretinal fluid and complete resolution of the peripheral retinal neovascularization.
Although the pathophysiology of cavitary disc maculopathy remains incompletely understood, our case demonstrates that optic nerve sheath fenestration may serve as a primary treatment to drain the subretinal fluid in select patients with this rare condition. In addition to previous reports of optic nerve sheath fenestration success, our decision to perform the procedure was based on the hypothesis that, in some cases, cavitary disc maculopathy may occur owing to an abnormal connection between intraocular and extraocular spaces.6,7,14,19 While optic nerve sheath fenestration carries potential risks, including CSF leak, optic nerve trauma, temporary ocular motility disorders, and vascular occlusion, no complications occurred in our patient. 20 The procedure resulted in successful drainage of subretinal and submacular fluid. This reduction supports the presence of a possible anatomic connection between the subretinal space and the subarachnoid compartment, thus allowing a better understanding of the underlying pathophysiology of cavitary disc maculopathy. Consistent with previous reports,14,19 our findings further support the hypothesis of fluid extravasation from the subarachnoid space into the subretinal space. Accordingly, optic nerve sheath fenestration represents a physiologically targeted therapeutic approach that directly addresses this communication and may provide an effective treatment option for selected cases of cavitary disc maculopathy.
The use of laser photocoagulation in patients with cavitary disc maculopathy has been previously described as an adjunctive therapy, before or after PPV.16,18 In our case, juxtapapillary laser photocoagulation was applied to create a laser barricade and minimize the recurrence of subretinal fluid after drainage through the fenestration. Despite the application of extensive papillomacular bundle laser photocoagulation, the patient’s visual acuity remained stable (20/400 in the right eye and 20/20 in the left eye), and she reported no new visual symptoms after treatment. Our case suggests that optic nerve sheath fenestration may offer therapeutic benefit in some patients with cavitary disc maculopathy and may help avoid the risks associated with intraocular surgeries, particularly in patients with limited visual potential.11,19,21
Optic nerve sheath fenestration may be considered a viable therapeutic option in select cases of optic nerve colobomas and cavitary disc maculopathy. Long-term follow-up is needed to evaluate the risk of recurrence. Further research is warranted to determine the best treatment strategies and to better define the role of optic nerve sheath fenestration within the management spectrum of optic nerve coloboma– and cavitary disc maculopathy–associated subretinal fluid.
Footnotes
Ethical Approval
This case report was prepared in accordance with the Declaration of Helsinki. All protected patient health information was handled in compliance with the Health Insurance Portability and Accountability Act (HIPAA).
Statement of Informed Consent
Informed consent was obtained from the patient before the procedure, including permission for the publication of all photographs and images included in this report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.