
Abstract
Introduction
Diabetes is becoming increasingly prevalent, and diabetic retinopathy (DR) is among the leading causes of blindness in the working-age population. 1 Preventing the onset and progression of DR can significantly improve patients’ quality of life and overall health. Lack of physical activity is a well-known modifiable risk factor in the management of diabetes.2,3 It has been well established that physical inactivity and sedentary behavior are associated with the development and progression of diabetes and its microvascular complications. 4 Previous studies have also shown that higher levels of physical activity, as measured by counseling intervention or self-reported standardized questionnaires, are associated with decreased prevalence and progression of DR.5–8 However, more quantitative measures are needed to further elucidate the nuances of the relationship between physical activity and DR. Wearable technology, an increasingly available resource for both promoting and measuring physical activity, presents a simple, low-cost avenue for this investigation.
The All of Us Research Program is an effort to advance individualized, precision healthcare by accelerating health research discoveries. Established by the National Institutes of Health in 2018, the program now includes over 340 sites across the US, with 783 640 enrolled participants as of March 31, 2024 and with a goal of enrolling more than 1 000 000 participants. The All of Us program is free to join, and its participants are asked to complete surveys as well as give permission to share their electronic health record (EHR). In addition, participants may share samples of blood, urine, or saliva for laboratory or DNA tests. In 2019, the All of Us program announced the option for patients to link their personal fitness activity (Fitbit) tracker data 9 under the Bring Your Own Device program.
This study leverages accelerometry data from wearable activity trackers to examine the longitudinal impact of objective measures of physical activity on the development of DR.
Methods
Patient Selection
Accelerometer data from personal fitness trackers was gathered from 668 individuals with diabetes using the All of Us Research Program Registered Tier dataset version 7.
Participants were included in the study if they had linked activity tracking data, EHR data, and a diagnosis of diabetes as defined by the International Classification of Diseases, Tenth Revision diagnosis code and SNOMED Clinical Terms. In addition, participants must have been taking insulin or other diabetes medications, and have a hemoglobin A1c (Hb1c) level >6.5% or fasting glucose level >126 mg/dL. Participants were excluded from the study if they were age <18 years or if there was <1 month of activity tracking data available.
Statistical Analysis
Binary logistic regression models were used to assess the adjusted association between the presence of DR and the physical activity measures of mean number of daily steps (in unit increase increments of 1000 daily steps) and mean number of daily minutes spent on moderate-to-vigorous activities (in unit increase increments of 1 minute). Data analyses were performed in R Project for Statistical Computing (version 4.2.2).
Results
Of the 668 individuals with diabetes participating in the study, 421 (63%) were female and 247 (37%) were male; 534 (80%) were non-Hispanic White; and 284 (42.5%) had a history of smoking (defined in the patient questionnaire as having smoked ≥100 cigarettes over one’s lifetime). Mean age was 64.3 years (range, 25–91 years), and the mean body mass index was 33.9 kg/m2. The mean (±SD) HbA1c level was 6.62 ± 1.3% (range, 4.8%–10.5%), and 194 participants (29.0%) were taking insulin. The mean (±SD) duration of diabetes was 8.1 ± 3.5 years, and DR was present in 34 participants (5.1%). The mean systolic blood pressure was 127.0 mm Hg. Participants spent a mean 322.5 daily minutes asleep. In total, participants walked a mean (±SD) 6100 ± 2150 steps per day (range, 1020–14 410 steps) and engaged in a mean 30.1 minutes of moderate-to-vigorous physical activity per day (defined as the total number of minutes per day in which step cadence reached ≥100 steps per minute for at least 2 consecutive minutes). 10
A unit increase in the mean number of daily steps walked by participants (per 1000 daily steps) was significantly associated with a 45% reduction in the odds of having DR (odds ratio [OR] 0.55, 95% CI 0.33–0.91). When analyses were adjusted for the mean number of daily steps, women had significantly lower odds of having DR compared to men, while older patients and those with higher HbA1c levels had an increased risk of DR (Table 1).
Associations of Participant Characteristics With Presence of Diabetic Retinopathy Among 668 Participants in the All of Us Research Program, Adjusted for Mean Daily Steps. a
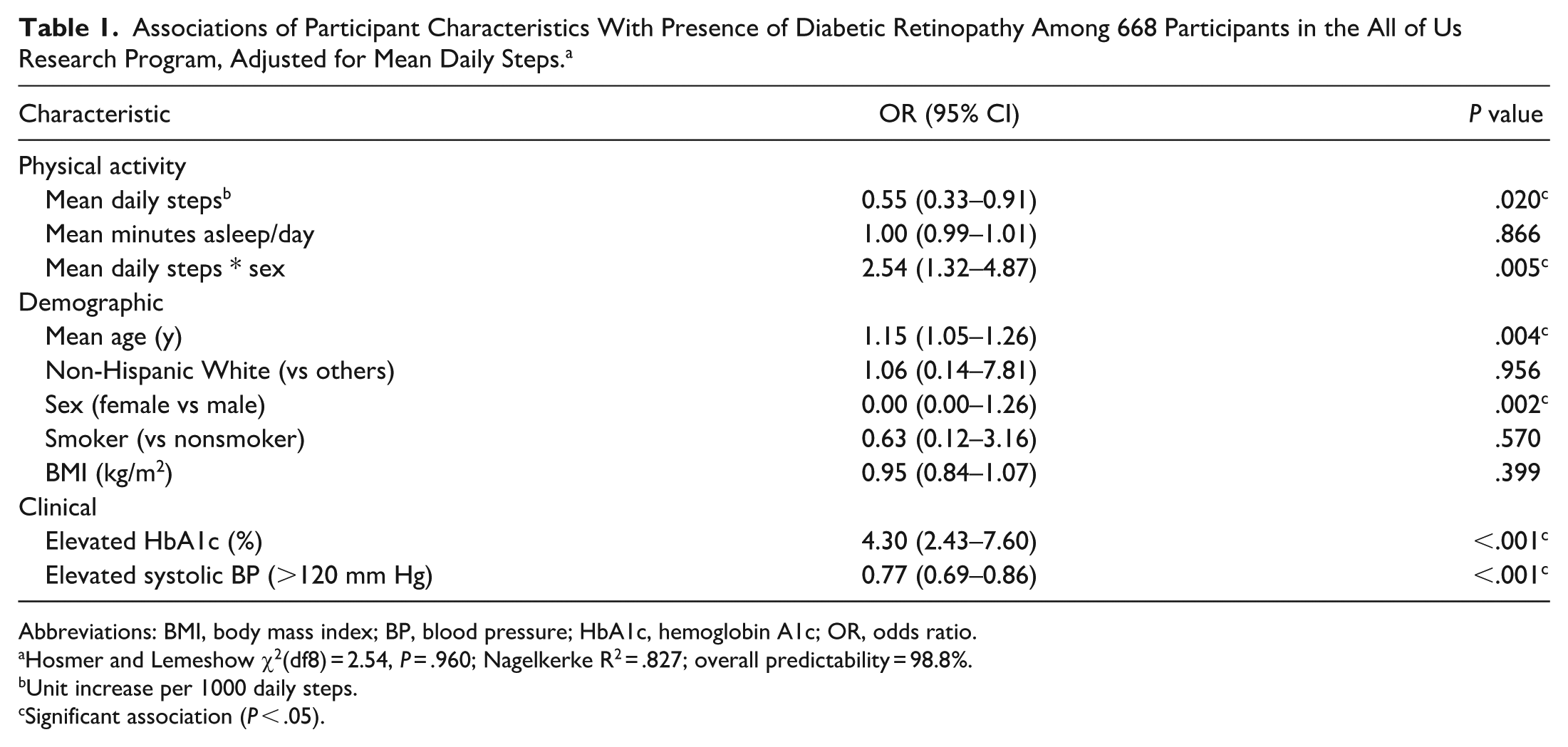
Abbreviations: BMI, body mass index; BP, blood pressure; HbA1c, hemoglobin A1c; OR, odds ratio.
Hosmer and Lemeshow χ2(df8) = 2.54, P = .960; Nagelkerke R2 = .827; overall predictability = 98.8%.
Unit increase per 1000 daily steps.
Significant association (P < .05).
A unit increase in the mean number of daily minutes spent on moderate-to-vigorous activity (per unit increase of 1 minute) was significantly associated with a 24% reduction in the odds of having DR (OR 0.76, 95% CI 0.63–0.92). When analyses were adjusted for the mean number of daily active minutes, women had significantly lower odds of having DR compared to men, while older patients and those with higher HbA1c levels had an increased risk of DR (Table 2).
Associations of Participant Characteristics With Presence of Diabetic Retinopathy Among 668 Participants in the All of Us Research Program, Adjusted for Mean Daily Active Minutes. a
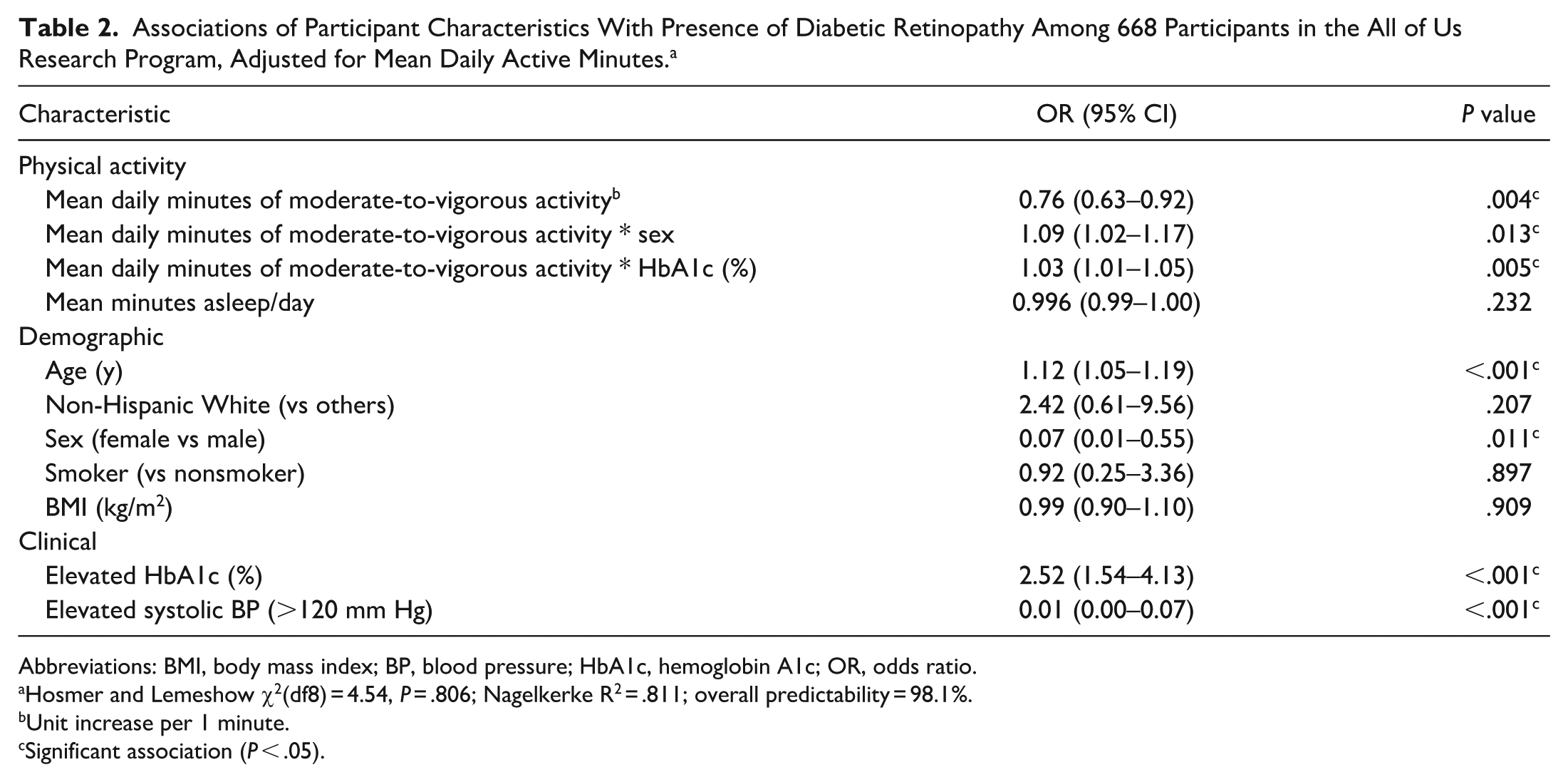
Abbreviations: BMI, body mass index; BP, blood pressure; HbA1c, hemoglobin A1c; OR, odds ratio.
Hosmer and Lemeshow χ2(df8) = 4.54, P = .806; Nagelkerke R2 = .811; overall predictability = 98.1%.
Unit increase per 1 minute.
Significant association (P < .05).
Conclusions
This study demonstrates that increased physical activity, as measured through objective quantification of both daily steps and minutes of activity, is inversely correlated with the presence of DR. This is in keeping with previous questionnaire-based studies showing that increased physical activity is associated with decreased prevalence, 6 less severe disease levels, 5 and lower risk of progression 7 of DR. This study also supplements a prior study assessing accelerometer-based data, 11 which highlighted the association between lower risk of both microvascular and macrovascular complications of diabetes and moderate-to-vigorous physical activity in particular. These data reinforce that wearable technology provides a novel and more precise avenue for measuring and quantifying physical activity levels. Considering the increasing population prevalence of diabetes, 12 it is important to identify simple approaches to ameliorating disease complications such as DR. These findings not only reinforce current diabetes management guidelines that recommend regular physical activity, 13 but also suggest that even modest increases in step count or activity intensity may yield measurable retinal health benefits. As wearable technology becomes increasingly accessible, integrating these data streams into both clinical care and research will be critical to advancing personalized medicine in diabetes management.
Study analysis was limited by the patient population in the All of Us Research database, which is subject to several levels of selection bias. The site-based recruitment methods tend to attract participants with more time available to complete surveys, and is further restricted to those with personal activity trackers. Individuals who wear fitness trackers are more likely to engage in healthy lifestyle behaviors that, in turn, can impact their disease status. Accordingly, the cohort of patients with both diabetes and available activity tracker data in the All of US registry was disproportionately White, female, and older than the national population with diabetes. Subsequent analyses should aim to stratify data on this basis, and will include a dedicated comparison between participants with and those without linked accelerometer data to quantify any selection bias that may be present.
There was also insufficient data to evaluate the severity or progression of disease, as only 5.1% of the study population had any degree of DR, and the mean HbA1c was just 6.62%, which is only slightly above the diagnostic threshold for diabetes. Moreover, this is not representative of the broader US population with diabetes, among whom it is estimated that 26.4% have any degree of DR, and whose mean HbA1c is notably higher, with 47.4% having an HbA1c level >7.0%.11,14 However, these data are relatively similar to the findings from previous accelerometer-based studies, 8 which have drawn meaningful inferences with moderately larger DR event counts. Additionally, the All of Us Research database does not currently include ocular imaging, which makes it difficult to validate retinopathy staging. Future investigations will incorporate ocular imaging when available in these national databases, and should include a more representative distribution of patients, especially focusing on patients with more severe disease, to further evaluate the role of physical activity in various demographics and stages of diabetes.
Overall, given the significant social and economic impact of diabetes and its microvascular complications, targeted prevention strategies are crucial. Our study contributes to evidence that wearable technology may play an important role in personalizing the management of this chronic disease, and highlights the potential for digital health tools to support risk stratification and early intervention, particularly in populations at high risk for vision loss. Additional studies are needed to further elucidate the role of physical activity in the development and progression of DR, with the goal of incorporating specific, personalized physical activity targets into treatment guidelines.
Footnotes
Acknowledgements
We thank all individuals who have delivered data to the All of Us Research Program. Beyond usual salary, no one received financial compensation for their contribution.
Authors’ Note
Levenson, Dias, Shah, Kovacs :Concept and design
Levenson, Dias, Shah, Kovacs: Acquisition, analysis, or interpretation of data
Levenson, Dias, Shah, Kovacs: Drafting of the manuscript.
Levenson, Dias, Shah, Kovacs: Critical review of the manuscript for important intellectual content.
Shah: Statistical analysis.
n/a: Obtained funding.
Shah: Administrative, technical, or material support.
Kovacs: Supervision.
Dr. Kovacs had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Ethical Approval
The Weill Cornell Medicine Institutional Review Board waived the need for ethics approval for the retrospectively obtained and anonymized data used in this noninterventional study.
Statement of Informed Consent
The Weill Cornell Medicine Institutional Review Board waived the need for patient consent for the collection, analysis, and publication of the study’s retrospectively obtained and anonymized data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Access to the All of Us Researcher Workbench is available to approved researchers who complete the registration, training, and data use agreement.