
Abstract
Introduction
Multiple myeloma is a plasma cell neoplasm belonging to a group of disorders known as immune gammopathies. These disorders are characterized by an overproduction of light- or heavy-chain immunoglobulin segments, which may deposit in various organs and increase serum viscosity, leading to systemic symptoms. Several ocular findings have been associated with multiple myeloma and related immune gammopathies, including ciliary, retinal, orbital, and neurologic abnormalities, although their underlying mechanisms remain incompletely understood. 1 Several retinal vascular manifestations of multiple myeloma occur secondary to hyperviscosity, including microaneurysms, hemorrhages, and retinal vein occlusions.1–4 Only a few cases have demonstrated other retinal sequelae, including deposits consisting of light- or heavy-chain immunoglobulin fragments, retinal detachments, subretinal fluid accumulation, and macular edema.5–8 Owing to their rarity, the underlying pathophysiology of these findings is neither well characterized nor well understood. This report aims to highlight the first described case of primarily intraretinal fluid and cystoid macular edema (CME) as a manifestation of smoldering multiple myeloma.
Case Report
A 67-year-old man with immunoglobulin A (IgA) κ smoldering multiple myeloma presented with more than 6 weeks of episodic blurry vision in his left eye. He had been diagnosed with multiple myeloma 1 year earlier, characterized by a faint IgA κ M-spike of 378 g/L and 10% plasma cells on bone marrow biopsy, with persistent neutropenia noted during his most recent evaluation. He had no significant prior ocular history, including no history of cataract surgery. He was referred to our retina service for a second opinion after a different ophthalmologist diagnosed him with a presumed retinal vein occlusion in the left eye, despite the absence of characteristic retinal findings.
Initial evaluation revealed a best-corrected visual acuity of 20/20 in the right eye and 20/60 in the left eye. Fundus examination demonstrated no significant abnormalities in the right eye and loss of the foveal reflex in the left eye (Figure 1, A and B). No vitreous or anterior chamber cells were noted. Optical coherence tomography (OCT) confirmed CME in the left eye, characterized by small intraretinal cystic spaces, and minimal ellipsoid zone (EZ) abnormalities in the right eye (Figure 1, C and D). The intraretinal fluid was accumulated primarily within the outer plexiform layer.
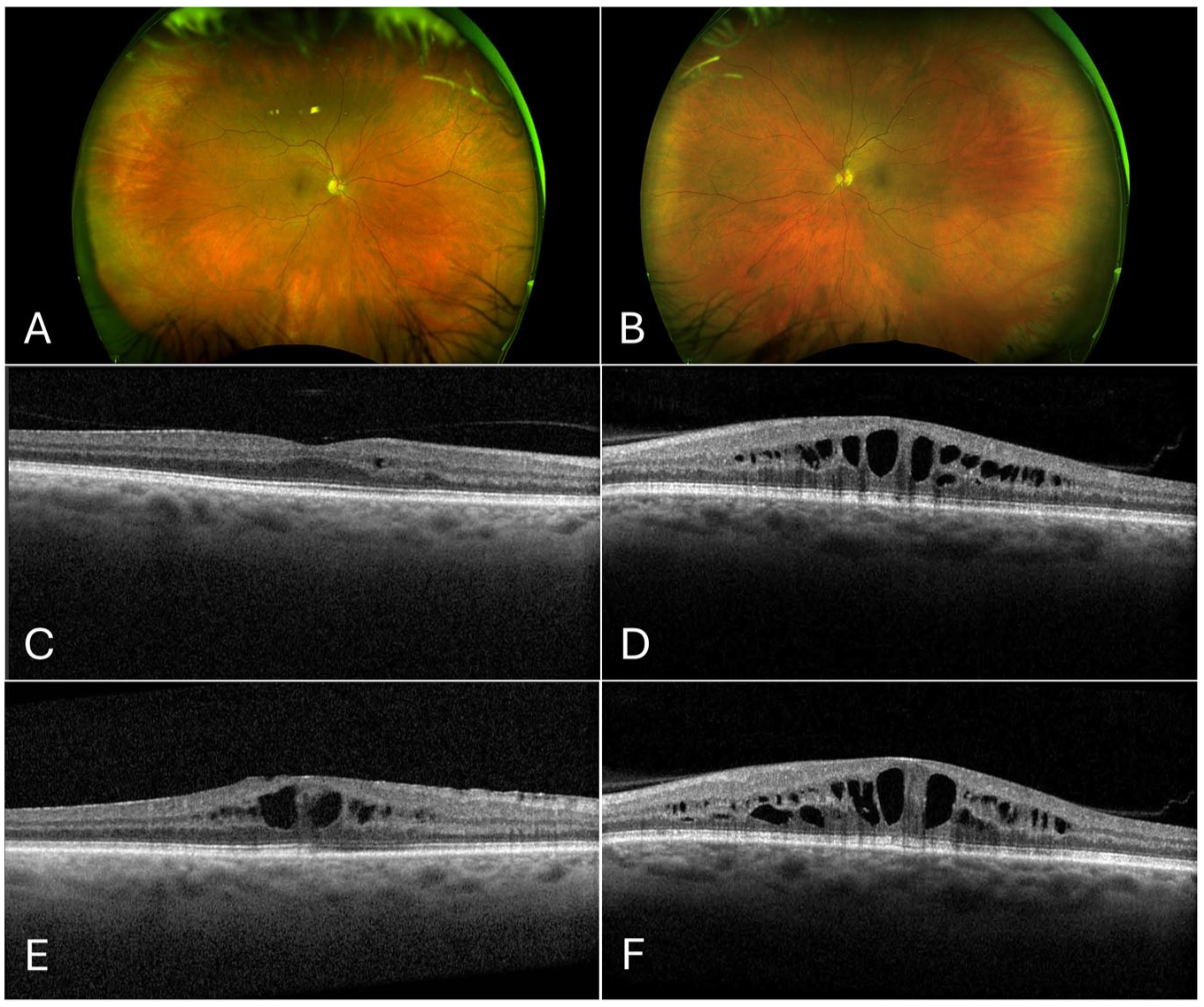
(A) Widefield fundus photograph of the right eye at initial presentation demonstrating no significant abnormalities. (B) Widefield fundus photograph of the left eye at initial presentation showing loss of the foveal reflex. (C) Optical coherence tomography (OCT) of the macula of the right eye at initial presentation, revealing small intraretinal fluid cysts, and (D) OCT of the left eye demonstrating more prominent cystoid macular edema (CME). (E) OCT of the right eye at the 2-year follow-up showing progression of CME after dorzolamide use. (F) OCT of the left eye during topical carbonic anhydrase inhibitor therapy, demonstrating persistent prominent CME.
Multiple myeloma was suspected to be the underlying etiology of the CME. Therefore, prednisolone acetate 1% and ketorolac tromethamine 0.5% eye drops were started 4 times per day in the left eye. The patient declined further intervention with intravitreal (IV) antivascular endothelial growth factor (anti-VEGF) injections and photodynamic therapy (PDT) for preventing further fluid accumulation or progression into adjacent layers of the retina. After 2 months without any improvement, topical treatments were discontinued owing to lack of efficacy. Subsequent fluorescein angiography (FA) revealed marked petaloid macular leakage in the left eye, without evidence of vasculitis (Figure 2, A and B). The patient was then started on topical dorzolamide 2% given 3 times per day in the left eye.
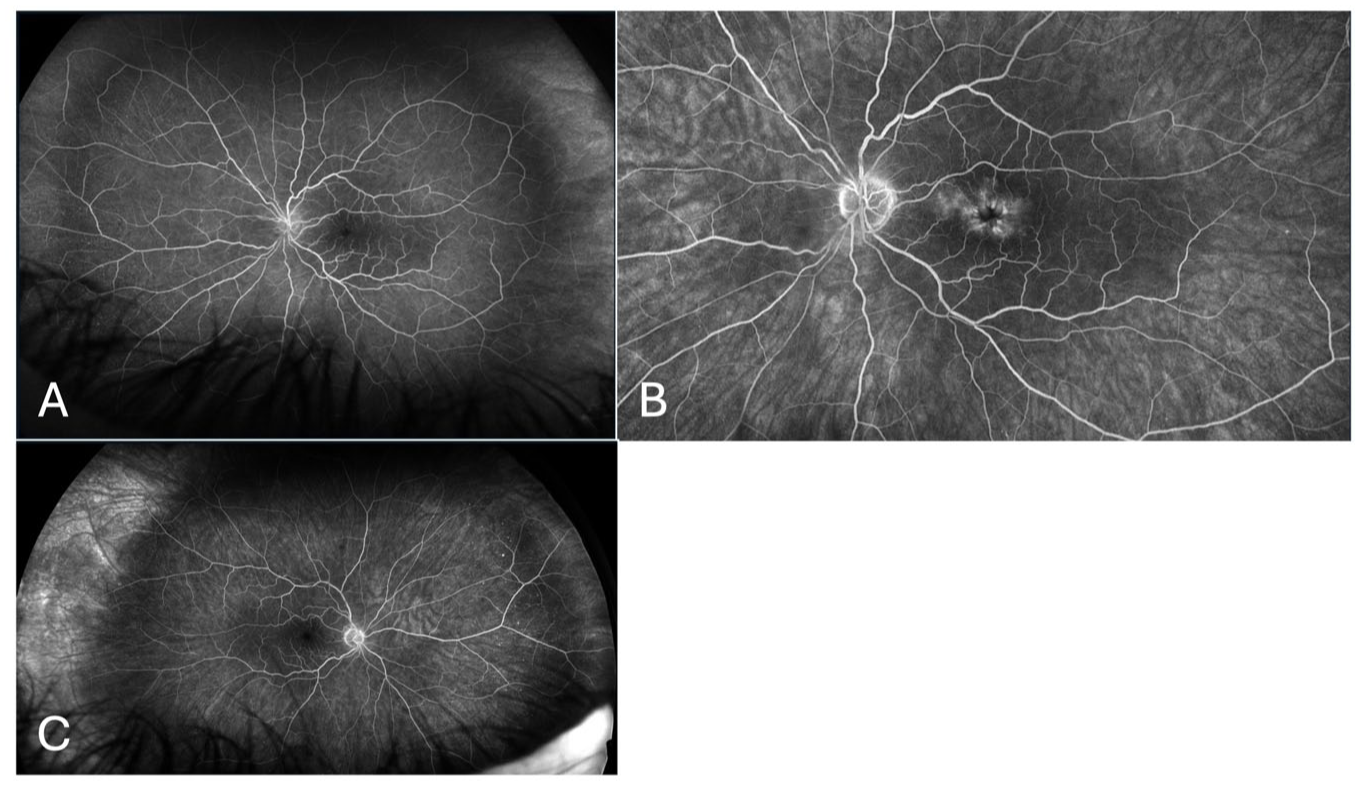
(A) Widefield fluorescein angiography (FA) of the left eye 2 months after treatment with a topical steroid and nonsteroidal anti-inflammatory drug, showing early-phase imaging at 33 seconds. (B) Higher magnification showing late petaloid macular leakage at 3 minutes and 36 seconds. (C) Corresponding FA of the right eye at 3 minutes and 46 seconds, showing mild late leakage.
At the 1.5-year follow-up, he remained on dorzolamide, and FA revealed new mild petaloid leakage in the right eye (Figure 2C). OCT showed persistent CME in both eyes with continued intraretinal fluid in the left eye. At the 2-year follow-up, OCT revealed worsening CME with mild EZ changes in both eyes. The VA was 20/20 OD and 20/50 OS (Figure 1, E and F). Given the patient’s stable vision and limited therapeutic response, dorzolamide was discontinued. Until the time of writing this report, the patient had not received any pharmacotherapy for smoldering multiple myeloma but remained on a clinical trial waitlist for linvoseltamab, a bispecific antibody targeting B-cell maturation antigen and CD3.
Conclusions
This case contributes to the literature on ophthalmic manifestations of myeloma spectrum disorders by documenting a unique retinal manifestation. To date, only 1 previously reported case has described CME associated with smoldering multiple myeloma. 4 This case represents the first reported instance of smoldering multiple myeloma presenting with sequential bilateral involvement characterized solely by intraretinal fluid accumulation. In addition, this case demonstrates resistance to standard topical treatment.
Initially, the patient’s symptoms were thought to be caused by a retinal vein occlusion; however, further evaluation revealed no significant hemorrhages, venous tortuosity, or areas of nonperfusion on FA. Initial OCT revealed CME in the left eye, with subsequent involvement of the right eye. This case highlights the importance of thorough multimodal imaging, which, along with bilateral disease progression, pointed toward an underlying systemic rather than vascular etiology. Notably, none of the characteristic clinical features of a retinal vein occlusion were observed.
Other differential diagnoses considered included vitreomacular traction and pachychoroid spectrum disease. Autoimmune retinopathy was considered as a potential differential, as it can present with CME and rapid-onset visual symptoms. Additionally, attenuation of the EZ can be observed in autoimmune retinopathy; however, our OCT images noted only minimal EZ abnormalities (Figure 1, C–F).9–11 Furthermore, our patient did not report characteristic symptoms such as photopsias, shimmering lights, or scotomas, nor were clinical signs such as optic atrophy or bone spiculation observed on fundus examination.10,12 Therefore, autoimmune retinopathy was considered unlikely to be the underlying cause of the patient’s condition.
In comparison, multimodal imaging in other hyperviscosity disorders, such as Waldenström macroglobulinemia, has shown variable findings, including tortuous retinal vessels, extensive retinal hemorrhages, and intraretinal as well as subretinal fluid accumulation, depending on the severity of the condition. Macular edema has also been reported as a notable finding in patients with immune gammopathies, potentially reflecting a pathophysiology similar to that in the present case.13–15 The pathophysiology behind this patient’s findings, and other related retinal manifestations of multiple myeloma, remain poorly understood. Unlike the first reported case of CME secondary to smoldering multiple myeloma, which demonstrated both intraretinal and subretinal fluid, our case showed intraretinal fluid only. 4 This potentially occurred via infiltration of immunoglobulins into the neurosensory retina and subretinal space, creating an osmotic pressure gradient that promotes fluid transudation into the intraretinal space.16,17 Impaired retinal pigment epithelium (RPE) pump function may further limit fluid resorption, contributing to persistent CME.7,16,17
Prior large-scale population-level analyses have shown that elevated plasma total protein levels are associated with thickening of the inner nuclear layer (β = 0.03, P = 7.9 × 10−10). 18 These mechanisms are independent of hyperviscosity and are more prevalent in IgA multiple myeloma, likely owing to the larger molecular weight of IgA.3,16 In addition, blood dyscrasias manifesting via any anemias or neutropenias, as seen in this patient, may promote CME by increasing transmural pressure and leakage of fluid across the vessel wall.19,20 Markers of pancytopenia, which are often associated with multiple myeloma, have also been associated with thickening of the outer plexiform layer, inner plexiform layer, and inner nuclear layer layers—all involved in the development of CME. 11
Although no clear intraocular inflammation was observed, CME often has an underlying inflammatory component. As a result, anti-inflammatory topical therapy, including nonsteroidal anti-inflammatory drugs and steroids, was initiated in case the inflammation was mild or subclinical. These treatments did not result in improvement, and escalation to a stronger corticosteroid such as difluprednate was avoided to prevent cataract formation. As a next step, dorzolamide was started. Carbonic anhydrase inhibitors reduce CME by promoting fluid resorption across the RPE. 21 After the patient experienced mild improvement, dorzolamide was discontinued, and the patient opted for close observation. This improvement may also be attributed to natural fluctuations observed in the course of this retinal manifestation, as CME has been reported to fluctuate or resolve spontaneously.22,23 Owing to his stable VA, the patient declined IV anti-VEGF injections and PDT.
Systemic chemotherapy is one of the main approaches for managing multiple myeloma-related retinal manifestations, aiming to reduce serum immunoglobulin levels. Although numerous cases have highlighted the necessity of this therapy, standardized treatment guidelines have not been established owing to the rarity of such cases.2,5,16,17 In a previously reported case, dexamethasone and bortezomib improved CME associated with smoldering multiple myeloma, likely owing to their antiangiogenic effects and reduction of immunoglobulin levels.3,4 In another case, macular edema and subretinal fluid resolved with chemotherapy, plasmapheresis, and an IV dexamethasone implant. 16 In addition, Salcedo Mafla et al described a patient with IgA multiple myeloma who developed intraretinal fluid similar to that observed in our case, with improvement following IV bevacizumab administration in the absence of systemic chemotherapy. 3 In the present case, treatment focused on addressing the CME rather than the underlying hematologic disorder. At the time of writing, the patient was awaiting enrolment in an experimental clinical trial, which may reduce systemic disease burden and improve ocular outcomes.
Although current clinical evidence does not strongly indicate that ocular involvement is a marker of disease severity in monoclonal gammopathy of undetermined significance or multiple myeloma, macular edema has been reported in association with both these conditions.5,24 In light of the unique findings of our case, CME could be the initial manifestation of myeloma spectrum disorders and should be considered in patients with treatment-resistant macular edema. Oncologists should also remain vigilant and counsel patients appropriately to monitor vision changes. Early intervention, including systemic chemotherapy when clinically indicated, may help avoid potential long-term sequelae of any retinal manifestations in affected patients.
This case highlights a rare occurrence of cystoid macular edema in a patient with smoldering multiple myeloma. It underscores the importance of considering myeloma spectrum disorders in cases of unexplained CME. Patients with smoldering multiple myeloma who experience visual symptoms should undergo prompt ophthalmologic evaluation and intervention to facilitate early diagnosis and management and prevent further visual impairment.
Footnotes
Authors’ Note
Dr. Nimesh Patel is the senior author.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)-compliant manner.
Statement of Informed Consent
Verbal informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Patel is a consultant for Apellis, Alcon, Allergan, Atheneum, biogen, Dorc, Alimera, Eye Point, Genentech, Regenx Bio, Regeneron, Lifesciences, Guidepoint, and Gerson Lehrman Group, Inc.
None of the other authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Hoyek and Dr. Zekavat are supported by the VitreoRetinal Surgery Foundation. Dr. Patel is supported by the Simourian Family Foundation and the Saint Vincent de Paul Foundation funding to the Retina Innovation Fund, Massachusetts Eye and Ear, Boston, MA. The funding organizations had no role in the design or conduct of this research.