
Abstract
Introduction
Macular telangiectasia type 2 is an idiopathic, bilateral ocular disorder characterized by slowly progressive foveal atrophy that eventually leads to central vision impairment. 1 It is commonly diagnosed in middle-aged women and has a reported prevalence of 0.1%. 2 The prevailing theory regarding macular telangiectasia type 2 posits that degeneration of Müller cells is the primary pathogenic event driving disease progression. This degeneration disrupts retinal structural integrity, leading to the formation of intraretinal cystic spaces. Over time, these spaces may enlarge and coalesce, potentially progressing to a full-thickness macular hole (FTMH).1,3 Furthermore, the depletion of Müller cells is believed to trigger a secondary response in the form of retinal telangiectasia, contributing to the distinct clinical features observed in macular telangiectasia type 2. 4 An FTMH is an uncommon but clinically significant complication of the condition, often resulting in central scotoma and substantial visual impairment. Various management strategies have been described, including medical treatments, surgical interventions, and watchful observation.1,5,6
Conventional surgical interventions for repairing FTMHs associated with macular telangiectasia type 2 have generally yielded suboptimal outcomes.7,8 However, Sborgia et al reported the use of the inverted internal limiting membrane (ILM) flap technique for treating FTMHs secondary to macular telangiectasia type 2. They reported improvement in visual acuity (VA) at the 3-month follow-up, despite incomplete closure of the macular hole. 9
Few studies have reported spontaneous closure of FTMHs in cases of macular telangiectasia type 2, attributed to the release of vitreoretinal adhesions, occurring in up to 6% of cases, or potentially to Müller cell proliferation.10,11 These findings suggest a complex interplay of factors influencing the course and management of FTMH in macular telangiectasia type 2.
Case Report
A 40-year-old woman presented with a persistent right-sided central scotoma for 1 year. Her medical history was significant for diabetes mellitus and hypertension, while her ophthalmic history was insignificant. Comprehensive ophthalmic examination showed a best-corrected visual acuity (VA) of 20/300 in the right eye and 20/30 in the left eye. Anterior segment findings were within normal limits for both eyes. Dilated fundus examination showed subtle right-angle venules and loss of macular transparency temporal to the fovea in both eyes. An FTMH was detected in the right eye. No pigment changes or signs of choroidal neovascularization were observed. Optical coherence tomography (OCT) confirmed an FTMH with inner retinal cavitation in the right eye and an ILM drape in the left eye (Figure 1). Based on these findings, a diagnosis of macular telangiectasia type 2 in both eyes with secondary FTMH in the right eye was established. The treatment plan consisted of pars plana vitrectomy (PPV) with a 360-degree ILM flap technique and gas tamponade in the right eye.
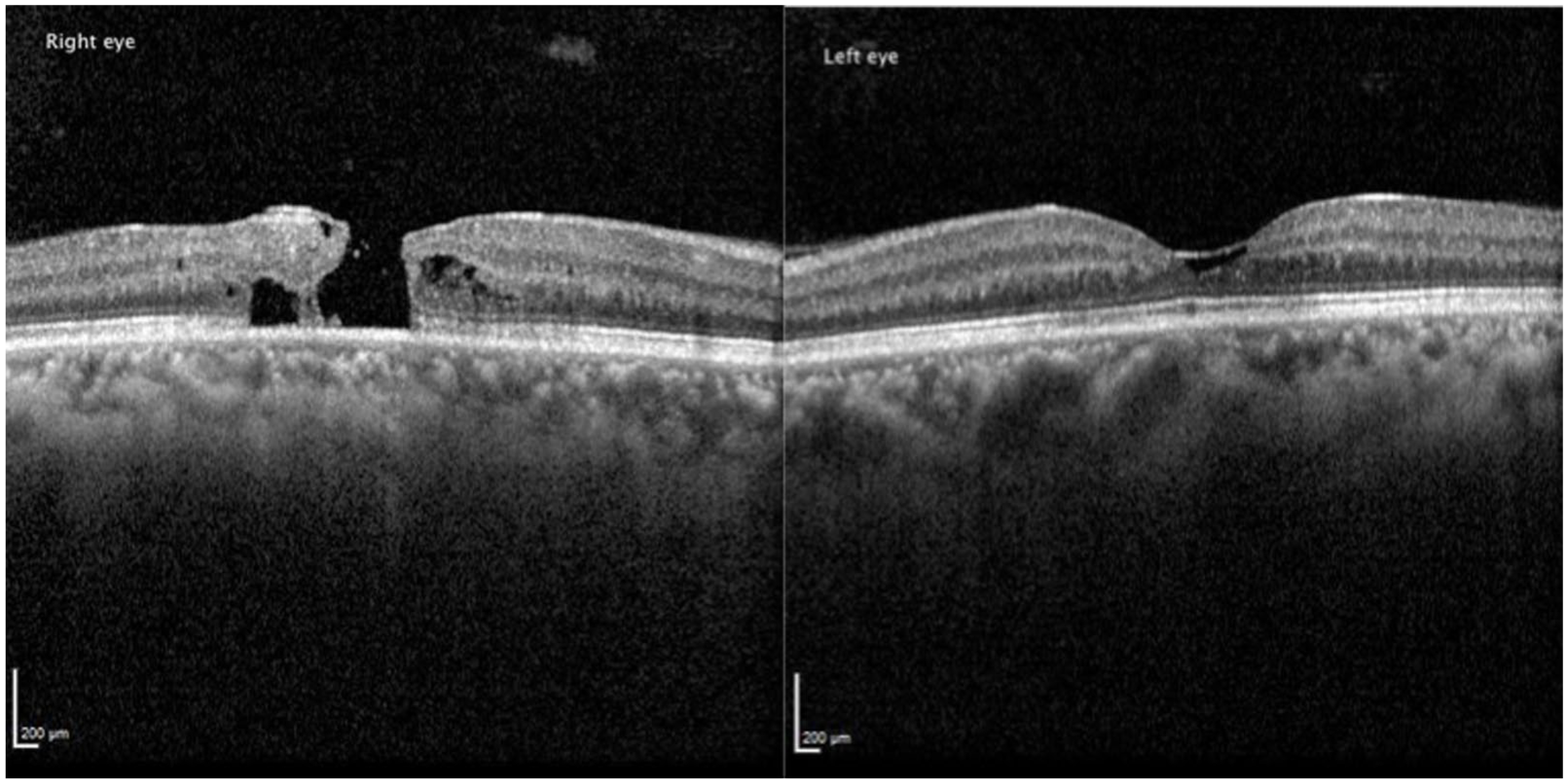
Optical coherence tomography (OCT) of the right eye demonstrates a full-thickness macular hole with inner retinal cavitation. OCT of the left eye shows an internal limiting membrane drape, consistent with features of macular telangiectasia type 2.
PPV was started with a core vitrectomy, followed by the induction of posterior vitreous detachment. Brilliant blue G dye was applied to stain the ILM. Using an inverted 360-degree flap technique, the ILM was peeled starting from the temporal to the fovea in a circular manner, extending approximately 2 disc diameters around the macular hole. During the circumferential peeling, the ILM was not completely removed from the retina but was left attached at the edges of the macular hole. This ILM remnant was then inverted to cover the macular hole circumferentially. Figure 2 demonstrates the 360-degree ILM flap technique. 12 A fluid–air exchange was then performed, followed by tamponade with 20% sulfur hexafluoride (SF6). The patient was instructed to maintain a facedown position for 7 days after the procedure.
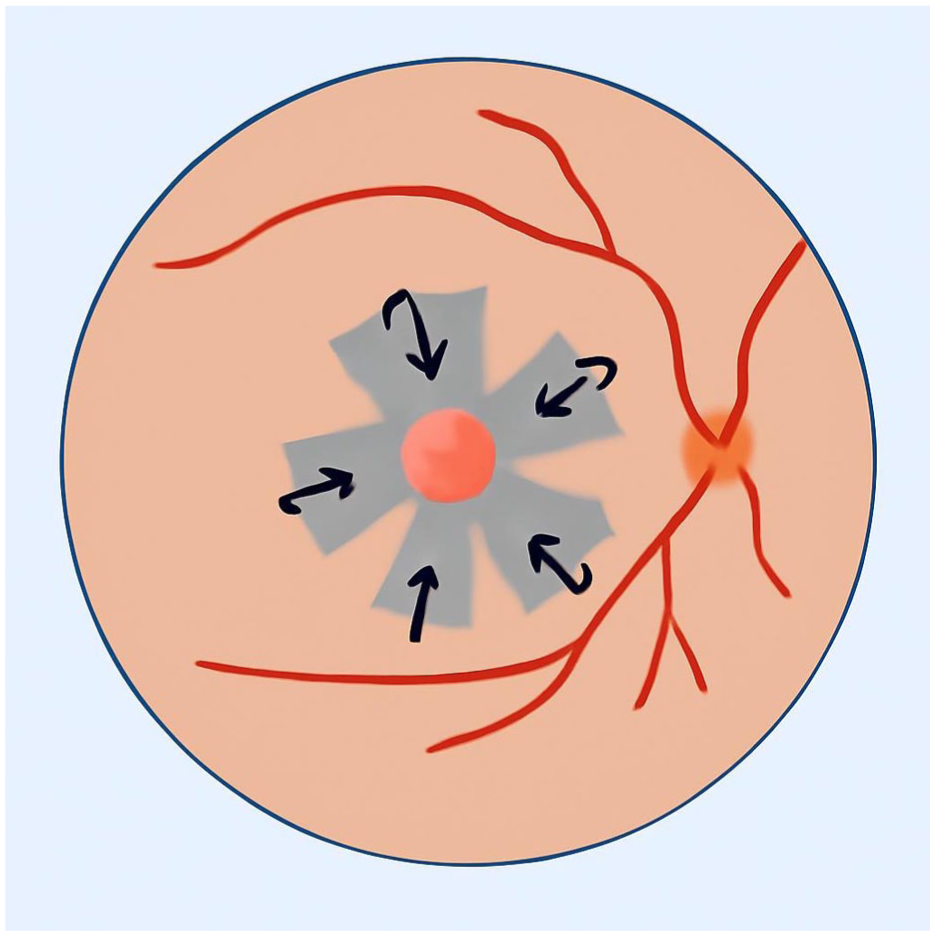
Image demonstrating the 360-degree inverted internal limiting membrane flap technique.
The patient was observed for 24 months postoperatively. At the 6-month postoperative visit, her VA had improved to 20/200 on the Snellen chart, and OCT demonstrated partial closure of the macular hole (Figure 3A). At 12 months, both VA and OCT findings remained largely unchanged, with persistent partial closure of the macular hole and a VA of 20/200 (Figure 3B). At the 24-month follow-up, the patient still had the same VA of 20/200; however, OCT imaging showed almost complete closure of the macular hole, with loss of inner segment/outer segment photoreceptors and disruption of the ellipsoid zone (Figure 3C). Figure 3 illustrates the postoperative OCT images across the follow-up period.
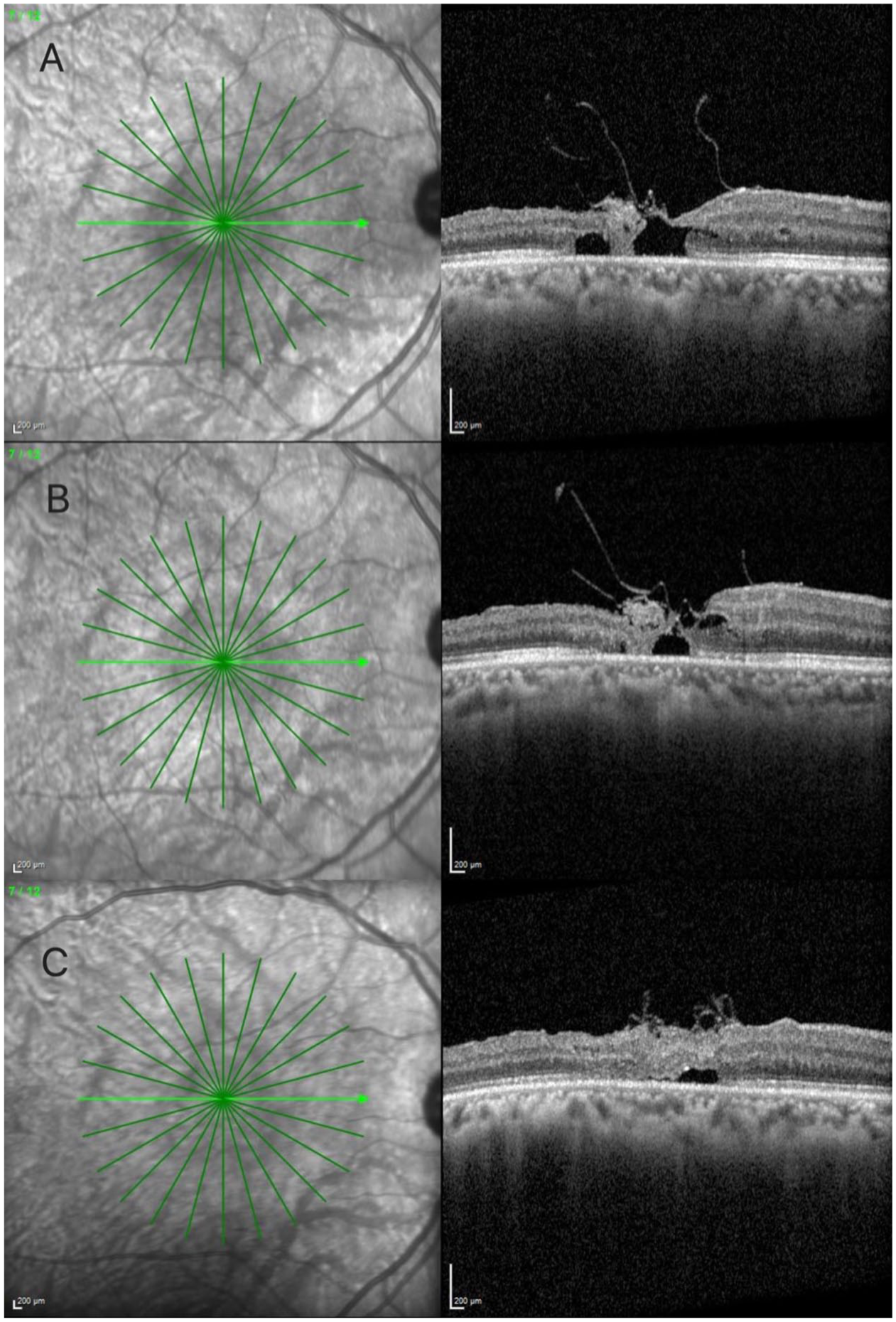
Postoperative optical coherence tomography image at (A) 6 months showing partial closure of the macular hole. (B) At 12 months, further reduction in macular hole size is seen with persistent partial closure. (C) At 24 months, near-complete closure of the macular hole is seen, with ongoing disruption of the outer retinal layers, including the ellipsoid zone and inner segment/outer segment junction.
Conclusions
An FTMH is a rare complication of macular telangiectasia type 2. It was first reported by Olsen et al, who documented its occurrence in a patient with the disease who had not undergone any surgical intervention. 13 The pathophysiology of FTMH occurrence in macular telangiectasia type 2 differs from the typical pathophysiology associated with vitreomacular traction seen in idiopathic macular holes, which generally show high closure rates after surgery. In macular telangiectasia type 2, FTMH formation is attributed to progressive neurosensory retinal degeneration accompanied by the development and coalescence of cystic spaces. 7 The degree of tissue atrophy and the appearance of FTMH on posterior OCT may play an important prognostic role. 13 The 360-degree ILM flap technique has shown favorable outcomes in cases of idiopathic macular holes; however, its visual benefits appear to be less consistent in cases of macular holes associated with macular telangiectasia type 2. One study demonstrated significant visual improvement following the ILM flap procedure in patients with idiopathic macular holes, regardless of their size. 14
Owing to the rarity of this condition, only a few reports have described the surgical outcomes and long-term follow-up, and a standardized treatment approach has not yet been established. Surgical outcomes for FTMH associated with macular telangiectasia type 2 remain suboptimal, as OCT findings sometimes show structural restoration without corresponding improvements in VA. Reported closure rates are 30% when the ILM is peeled.15 –17
In this report, we present a case of FTMH associated with macular telangiectasia type 2 that was treated using the 360-degree inverted ILM flap technique combined with gas tamponade. This approach led to a mild improvement in VA and nearly complete closure of the macular hole at 24 months postoperatively; however, disruption of the outer retinal layers persisted. The ILM flap technique was first introduced by Michalewska et al, who demonstrated significant improvements in both functional outcomes and anatomic closure rates in patients with large idiopathic macular holes. 16 Various theories have been proposed regarding the pathophysiology of macular hole closure. One theory suggests that the inverted ILM flap may accelerate the closure process by promoting the proliferation and migration of glial cells, which ultimately contributes to macular hole filling. 5
Michalewska et al conducted a prospective clinical trial and concluded that the inverted ILM flap technique effectively reduces the postoperative flat-open configuration of macular holes. This approach significantly enhances both functional and anatomic outcomes of vitrectomy for macular holes greater than 400 µm in diameter. 16 Nishiyama et al reported the 2-year surgical outcomes of 3 patients with FTMH associated with idiopathic macular telangiectasia type 2 who underwent the inverted ILM flap procedure. 5 Of the 3 patients, 2 achieved successful closure of the macular holes, with VA improving to 20/20. The third patient demonstrated temporary closure for 6 months, after which the hole reopened, resulting in a final VA of 20/100 at the last follow-up examination. The findings suggest that the inverted ILM flap technique is an effective, safe, and viable alternative approach for managing this condition.
In summary, this case demonstrates that the inverted 360-degree ILM flap technique may offer an effective surgical option for closing FTMHs associated with macular telangiectasia type 2. However, owing to the rarity of this condition, current evidence remains limited, and long-term visual and anatomic outcomes are not yet established. Multiple factors, including the delayed presentation of patients, advanced retinal atrophy, and the underlying neurodegenerative pathophysiology of macular telangiectasia type 2, may negatively affect surgical outcomes.
Although the inverted ILM flap technique has shown promise in achieving anatomic closure, improvements in VA remain unpredictable and often limited. Studies reveal varied outcomes, ranging from complete closure and improved vision to temporary or incomplete closure with limited functional benefit. Given these uncertainties, larger prospective studies with longer follow-ups are needed to better define optimal surgical strategies and assess long-term outcomes for FTMH associated with macular telangiectasia type 2.
Footnotes
Ethical Approval
This case report received approval from the Institutional Review Board of King Khaled Eye Specialist Hospital.
Statement of Informed Consent
Written informed consent was obtained from the patient for the clinical procedure and for the publication of this case report and accompanying images.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.