
Abstract
Keywords
Introduction
Fungal endophthalmitis is a rare but serious, vision-threatening infection that poses significant diagnostic and therapeutic challenges owing to its insidious onset, nonspecific symptoms, and limited treatment options. Common causative organisms include Aspergillus and Fusarium (molds) and Candida species (yeast). An Indian study identified Aspergillus as the most frequent pathogen (37.06%), followed by Fusarium (16.87%) and Candida (10.65%). 1 Mold infections are typically exogenous and occur in immunocompetent individuals, while yeast infections, particularly those caused by Candida albicans, are endogenous and often affect immunocompromised patients. Risk factors include recent hospitalization, diabetes mellitus, renal or liver failure, indwelling catheters, organ transplantation, and immunosuppressive therapy. Treatment involves a combination of intravitreal (IVT) and systemic antifungals, with or without vitrectomy. IVT amphotericin B and voriconazole are the most commonly used agents, while clinical experience with IVT caspofungin remains limited. 2
This case highlights the successful treatment of bilateral endogenous fungal endophthalmitis with a good visual outcome. To our knowledge, this is the first report in human eyes demonstrating the effect of caspofungin on retinal function using electroretinography (ERG), with the other eye serving as a control.
Case Report
A 40-year-old woman presented with a 1-month history of diminished vision and pain in her right eye. A week before symptom onset, she was diagnosed with left renal hydronephrosis secondary to a ureteral calculus and underwent double-J stent placement. During treatment, she developed a pleural effusion, which was managed with intravenous antibiotics, following which the double-J stent was removed. She was subsequently treated elsewhere with topical and oral antifungal therapy.
On presentation, best-corrected visual acuity (BCVA) was hand motion OD and 0.8 logMAR (20/125) OS. Slitlamp examination revealed keratic precipitates with anterior chamber cells and flare, more pronounced in the right eye, with no hypopyon (Figure 1, A and B). Dense vitreous haze was noted in the right eye, while the left eye showed vitreous and preretinal infiltrates at the posterior pole (Figure 1, C and D).
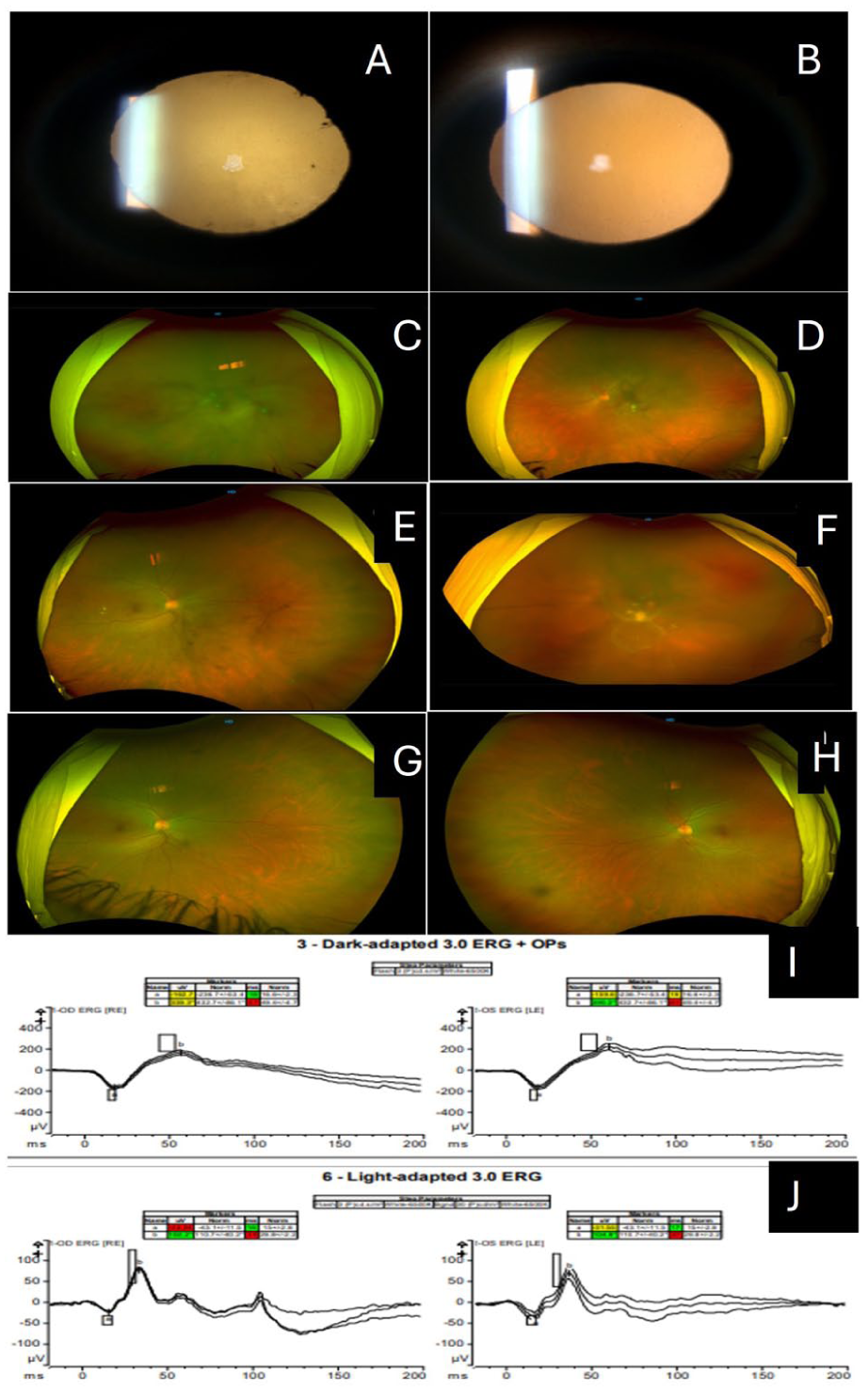
(A) Slitlamp photograph (10×; retroillumination) at presentation shows posterior synechiae with a dull fundus glow in the right eye. (B) The left eye shows a clear media. Widefield fundus photographs show preretinal exudates, more prominent in the (C) right eye than in the (D) left eye. (E, F) Day 9 postvitrectomy images. (E) The right eye shows organizing exudates, and (F) the left eye shows clinical worsening with the characteristic “string of pearls” appearance of exudates. (G, H) At the 1-month follow-up, both eyes exhibited clear media with a healthy optic disc and macula. (I, J) Electroretinogram demonstrates comparable dark-adapted (3.0) and light-adapted responses between the control (right) eye and the caspofungin-injected (left) eye.
Ultrasonography of the right eye revealed numerous low-reflective dots and clump echoes with an attached retina. Pars plana vitrectomy (PPV) with IVT voriconazole (100 μg/0.1 mL) was performed in the right eye, and vitreous aspirates were sent for bacterial and fungal cultures and polymerase chain reaction (PCR) analysis. On postoperative day 3, PCR was positive for panfungal genomes, and culture showed budding yeast. Urine cultures grew Klebsiella pneumoniae. On day 4, infectious disease specialists recommended intravenous meropenem (1 g, 3 times daily for 10 days) and oral fluconazole (400 mg daily). Owing to clinical worsening in the left eye, IVT voriconazole was administered bilaterally. Topical steroids, antibiotics, cycloplegics, and antifungals were continued. On day 5, vitreous aspirate from the right eye grew Candida albicans, which was highly sensitive to amphotericin B and flucytosine, moderately sensitive to caspofungin and micafungin, and resistant to voriconazole and fluconazole.
On day 6, the BCVA of the patient was 0.8 logMAR (20/125) OD and 1.47 logMAR OS. Organizing exudates in the right eye were closely observed, while IVT amphotericin B (5 μg/0.1 mL) was injected in the left eye for persistent exudates. Topical voriconazole and oral fluconazole were discontinued. Based on the favorable response observed in the right eye, IVT voriconazole was repeated in the left eye on day 8. Despite IVT therapy, the left eye showed clinical worsening, and PPV was therefore performed on day 9 (Figure 1, E and F). Although the infectious disease specialist recommended intravenous amphotericin B, the patient declined owing to concerns regarding systemic toxicity. Liver function was closely monitored throughout the course of treatment.
On day 11, the vitreous aspirate from the left eye showed heavy growth of Candida albicans. Postoperatively, IVT amphotericin B was administered but elicited a suboptimal response. Hence, IVT caspofungin (50 μg/0.1 mL) and IVT amphotericin B were administered alternately (5 doses each) in the left eye. Oral fluconazole was restarted at a dose of 200 mg 2 times a day. Gradual resolution of organizing exudates and improved media clarity were noted. The patient was closely observed for recurrence, even after cessation of IVT therapy (Figure 1, G and H).
Four weeks later, the BCVA of the patient improved to 0.2 logMAR (20/32) OD and 0.3 logMAR (20/40) OS. At the 2-month follow-up, visual acuity was maintained, and fundus examination revealed a structurally normal retina. However, functional assessment using ERG showed slightly reduced and delayed scotopic responses, with normal but delayed light-adapted responses that were comparable in both eyes (Figure 1, I and J). Regular follow-up was advised.
Conclusions
Endogenous endophthalmitis frequently presents bilaterally (67%) and is often associated with multifocal lesions (80%). The infection progresses from the choriocapillaris to the vitreous, causing chorioretinitis, vitritis, anterior segment inflammation, and, in severe cases, exudative retinal detachment. 3 In this case, the presence of a double-J stent and anemia (hemoglobin: 10.2 g/dL) likely predisposed the patient to infection.
The indolent course of fungal endophthalmitis often delays diagnosis. Pulimood et al 4 reported a mean latent period of 30 days, with only 3% of patients presenting within 1 week of symptom onset. A characteristic feature of Candida endophthalmitis is a fluffy, creamy-white, well-circumscribed retinal lesion with strand-like extensions, creating a classic “string of pearls” appearance, often accompanied by vitreous haze, as observed in our patient. 5 Comprehensive systemic investigations are essential in cases of endogenous endophthalmitis to identify the primary septic focus and to monitor for drug-related toxicity. Microbiologic analysis of ocular fluids remains the cornerstone of diagnosis, while consultation with infectious disease specialists is crucial for effective systemic infection control.
Early vitrectomy is both diagnostic and therapeutic, as it reduces the fungal load and enhances intraocular drug penetration. Sallam et al 6 demonstrated that early vitrectomy significantly reduces the risk of retinal detachment. IVT amphotericin B (5–10 μg/0.1 mL) and voriconazole (100 μg/0.1 mL) are standard treatment options, with voriconazole preferred for its broad antifungal spectrum and superior ocular penetration. Owing to poor systemic bioavailability and significant systemic toxicity, amphotericin B is primarily used intravitreally. 7 In the present case, vitrectomy was performed in the right eye at presentation and in the left eye a week later. However, a suboptimal response to amphotericin B in the left eye necessitated switching to caspofungin.
Oral fluconazole was restarted, based on the rationale that Candida infections usually respond favorably to fluconazole. 8 Alternating IVT injections of amphotericin B and caspofungin effectively controlled the infection in the left eye. This highlights 2 important considerations: 1) in vitro antifungal sensitivity may not always translate to in vivo outcomes, especially in fungal infections, 9 and 2) combination therapy may leverage the synergistic effects of amphotericin B and caspofungin, thereby reducing toxicity, enhancing pharmacokinetics, and overcoming resistance. 10
Caspofungin, a cell wall synthesis inhibitor, is effective against Candida and Aspergillus species, including azole- and amphotericin B-resistant strains. Although primarily approved for intravenous use, off-label IVT administration has shown encouraging results. Several case reports have highlighted the successful use of intravenous and/or IVT caspofungin using varying doses and regimens.7,11,12 Yadav et al 13 demonstrated the efficacy of alternating IVT amphotericin B (50 μg/0.01 mL) and caspofungin (50 μg/0.1 mL) administered 4 times each in a similar case; however, recurrence occurred after cessation of therapy, and amphotericin B-induced nephrotoxicity was noted. 13 In contrast, in the present case, we combined the lowest effective dose of amphotericin B (5 μg/0.1 mL) with caspofungin (50 μg/0.1 mL), achieving sustained infection control without retinal toxicity or recurrence.
IVT caspofungin was administered at a concentration of 50 μg/0.1 mL, and ERG findings were comparable between the 2 eyes, with the right eye serving as the control. These findings are consistent with those reported by Shen et al in rabbit retinas, where IVT caspofungin at concentrations up to 200 μg/mL did not impair retinal function. 14 They reported no significant differences in ERG amplitudes or implicit times, suggesting preserved inner and outer retinal function. Additionally, the ratio of b-wave-to-a-wave amplitude was similar between the caspofungin-treated and control eyes.
Similarly, an in vitro study by Kernt and Kampik found no toxicity at vitreous concentrations ranging from 5 to 75 μg/mL after 24 hours of exposure. In contrast, concentrations exceeding 150 μg/mL led to a significant reduction in retinal pigment epithelial cell viability. ERG waveforms were comparable between control and treated eyes at nontoxic concentrations. 15
This case supports the use of IVT caspofungin as an effective adjunctive therapy for drug-resistant fungal endophthalmitis. Its uniqueness lies in the assessment of the effect of caspofungin on retinal function in the human eye using ERG. Further studies involving larger cohorts and longer follow-ups are required to confirm its safety and efficacy.
Footnotes
Ethical Approval
Ethical approval for case was obtained from the institutional review board.
Statement of Informed Consent
Verbal informed consent was obtained from the patient for publication of this case report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.