
Abstract
Introduction
Endophthalmitis, although rare, is a vision-threatening intraocular infection that, if untreated, can result in severe visual impairment or even blindness. 1 It is broadly classified as exogenous, following ocular surgery, trauma, or intravitreal injections, or endogenous, arising from hematogenous spread of infection.2,3 Postoperative endophthalmitis accounts for more than 70% of cases and most commonly occurs after cataract surgery. 4 Visual outcomes vary widely and depend on the causative organism, the degree of presenting intraocular inflammation, and the timeliness of treatment. 2
Bacterial replication within the vitreous cavity is exponential, typically with a 10-fold increase in bacterial load occurring within the first 3 hours after infection.3–8 The current standard of care involves the immediate administration of intravitreal broad-spectrum antimicrobials such as vancomycin, ceftazidime, and amikacin for suspected bacterial infections and amphotericin B or voriconazole for suspected fungal infections. In some cases, pars plana vitrectomy (PPV) may be required. 5 However, drug shortages, limited availability of medications in outpatient ophthalmology clinics, antimicrobial resistance, and patient-specific contraindications such as severe antibiotic allergies can lead to detrimental delays in treatment. These barriers highlight the need for safe, effective, and rapidly deployable nonantibiotic alternatives.
Povidone–iodine may help address these concerns owing to its wide availability, broad-spectrum antimicrobial activity, rapid onset of action, low cost, and lack of documented resistance.9,10 It acts by releasing free iodine, which penetrates microbial cell membranes and oxidizes intracellular proteins, nucleotides, and fatty acids.9–11 Its bactericidal effect can be achieved in as little as 15 seconds, significantly faster than that of antibiotics such as vancomycin, which may require 8 to 24 hours to achieve bactericidal activity.4,5,12 This rapid antimicrobial action may help prevent structural ocular damage and accelerate recovery.
Recent reports have described the use of povidone–iodine during PPV as an infusion additive and, in isolated cases, as an intravitreal injection administered before PPV. However, to our knowledge, no published study has evaluated in-office intravitreal povidone–iodine injection as a standalone treatment for exogenous endophthalmitis.13–16 Herein, we describe the clinical outcomes of patients with acute exogenous endophthalmitis and documented antibiotic allergies who were treated with intravitreal 1.25% povidone–iodine (0.1 mL).
Methods
This single-center, retrospective case series included patients with multiple antibiotic allergies who presented with acute exogenous endophthalmitis between 2018 and 2025. The study protocol was approved by the institutional review board of the University of Puerto Rico Medical Sciences Campus and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from each patient. After a discussion of the risks and benefits, each patient declined intravitreal antibiotic administration but agreed to and underwent vitreous tap and injection with 1.25% povidone–iodine (0.1 mL).
Inclusion criteria were patients who 1) presented with clinical signs of acute endophthalmitis after documented intraocular surgery or intravitreal injection, 2) had a history of severe allergy to antibiotics, 3) declined standard intravitreal antibiotic injections, and 4) had a minimum of 6 months of follow-up. Exclusion criteria were patients younger than 21 years of age, those with endogenous endophthalmitis, or those without a clear exogenous inciting event.
All patients underwent a standard in-office vitreous tap-and-inject procedure. After topical anesthesia with tetracaine and placement of an eyelid speculum, 5% povidone–iodine was applied to the ocular surface for at least 30 seconds. A vitreous tap was attempted 3.5 to 4 mm posterior to the limbus; if unsuccessful, an anterior chamber tap was performed. Immediately thereafter, 1.25% povidone–iodine (0.1 mL) was injected intravitreally at 3.5 to 4 mm posterior to the limbus. Samples were submitted for microbiological culture. After the procedure, all patients received prednisolone acetate 1% ophthalmic drops, which were tapered according to clinical response. Follow-up evaluations were conducted on days 1 and 3 and at weeks 1, 2, 4, 8, 12, and 24, with additional visits as needed. If no clinical improvement or worsening inflammation was evident after the povidone–iodine injection, PPV was planned as the next step in management.
Data collected included patient demographics, surgical history, povidone–iodine-related complications, and best-corrected visual acuity (VA). The primary outcomes were VA and treatment-related complications at 3 and 6 months. Statistical analyses were performed using Microsoft Excel. VA measurements were converted into logMAR equivalents for statistical analysis. Count fingers vision at 3 feet was assigned a logMAR value of 1.6, hand motions were assigned a value of 2.3, and light perception was assigned a value of 2.7. Descriptive statistics were calculated, and comparisons were made using paired t tests and regression analysis. A 2-sided P < .05 was considered statistically significant.
Results
A total of 7 eyes from 7 patients met the inclusion criteria. The mean patient age was 72 years (range, 31–85 years, SD, 18.9 years), and most patients (71%, 5 of 7) were female. The mean follow-up duration was 10.5 months (range, 3–24 months, SD, 7.5 months). Six eyes (86%) were left eyes (Table 1).
Demographic and Presenting Characteristics.
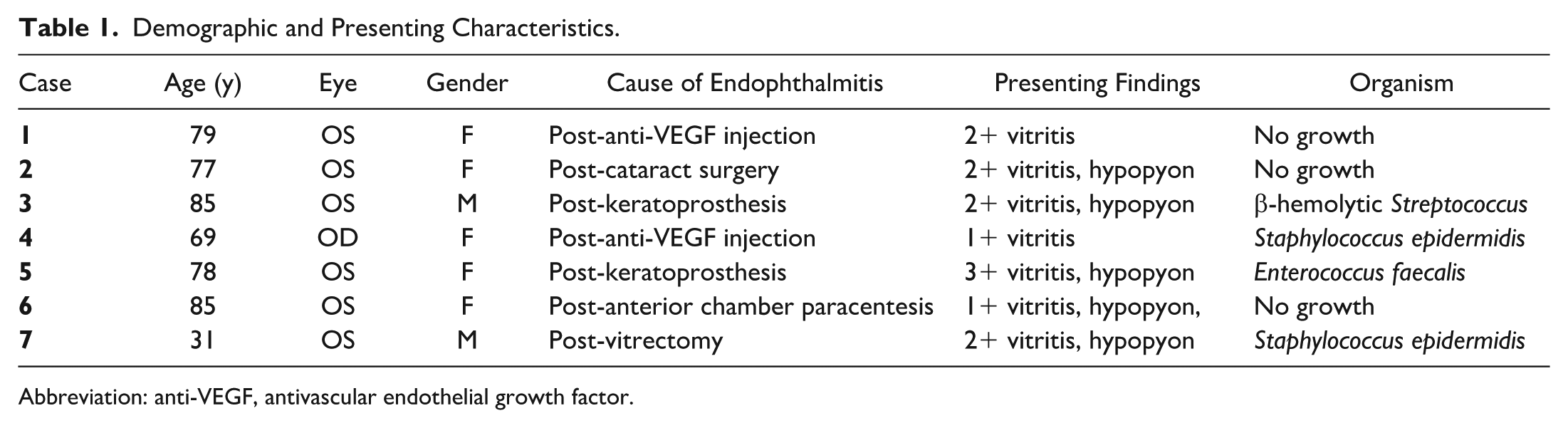
Abbreviation: anti-VEGF, antivascular endothelial growth factor.
Endophthalmitis Characteristics
Two (28.5%) patients developed endophthalmitis following keratoprosthesis implantation and 2 eyes (28.5%) following intravitreal injection. One case each occurred following vitrectomy, anterior chamber paracentesis, and cataract surgery. At presentation, most patients had a hypopyon (71.4%, 5 of 7) and 2+ vitritis (57.1%, 4 of 7) (Figure 1). Among the remaining patients, 2 (28.5%, 2 of 7) had 1+ vitritis, and 1 (14.3%, 1 of 7) had 3+ vitritis. Four patients (57.1%) had positive cultures, including 1 with Enterococcus faecalis infection. Staphylococcus epidermis and β-hemolytic Streptococcus species were the other isolated microorganisms.
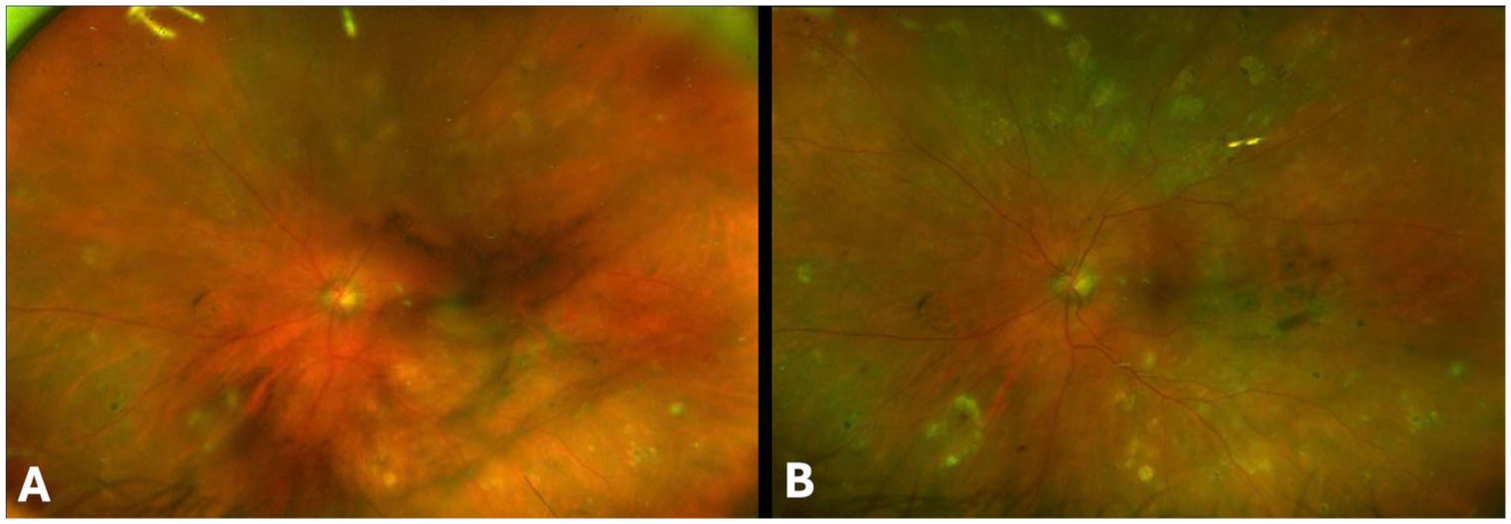
Patient 6. Ultra-widefield fundus images of an 85-year-old patient who presented with subjective vision loss and ocular pain 4 days after anterior chamber paracentesis. (A) Initial examination demonstrates hypopyon, vitritis, and vitreous debris. (B) Image taken 3 weeks after intravitreal povidone–iodine injection demonstrates improvement in vitritis and vitreous debris. The hypopyon and ocular pain had completely resolved.
Visual Outcomes
The mean BCVA at presentation was 1.83 ± 0.97 logMAR. Following treatment, VA improved to 0.91 ± 0.99 logMAR at 3 months (P = .03) and remained stable at 6 months (0.89 ± 1.00 logMAR, P = .03) (Table 2). At the final follow-up visit, the mean VA was 0.93 ± 0.98 logMAR (P = .03). VA improved after the procedure in all but 1 case. Overall, 5 patients (71%) recovered to baseline VA or better at 3 months after the procedure.
Visual Acuity Outcomes.
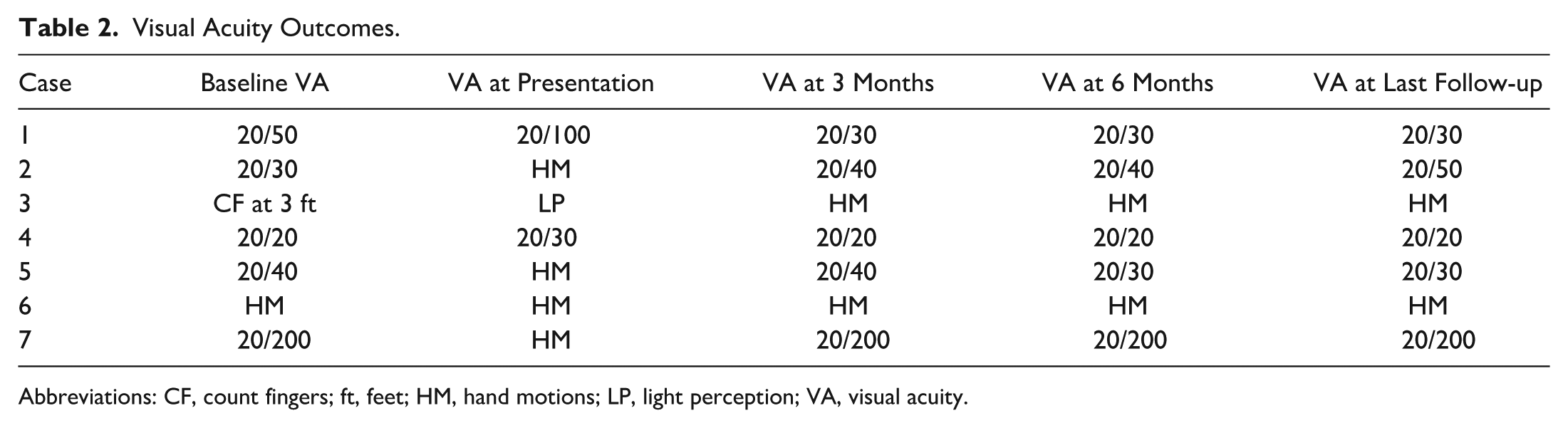
Abbreviations: CF, count fingers; ft, feet; HM, hand motions; LP, light perception; VA, visual acuity.
Safety
No adverse events or complications were observed following treatment with intravitreal 1.25% povidone–iodine (0.1 mL). There were no cases of delayed inflammation or retinal vasculitis, and no patients required subsequent PPV or intravitreal antibiotic therapy. In addition, no patients required treatment with oral or intravitreal corticosteroids.
Conclusions
In this retrospective series of patients with exogenous endophthalmitis treated with intravitreal povidone–iodine, in-office povidone–iodine monotherapy was noted to be safe and effective, with improvement in VA, pain resolution, and infection control. No povidone–iodine-related complications or adverse effects were observed at an average follow-up of 10 months after the procedure, and no patients needed further interventions.
Most patients in this series recovered to their baseline VA by 3 months after the procedure. Statistically significant improvement in VA was observed from baseline to both 3 and 6 months after the procedure. Moreover, 4 patients reported pain resolution by postoperative day 1, and pain had resolved in all patients by 1 week. Notably, no patients required PPV or further interventions.
Overall, these results suggest that intravitreal 1.25% povidone–iodine (0.1 mL) may be associated with favorable clinical outcomes in selected patients with exogenous endophthalmitis. This was especially notable in case 5, in which E. faecalis, a pathogen typically associated with significant retinal toxicity and poor visual outcomes, was isolated. The patient experienced rapid visual recovery to baseline by 1 week after the procedure, underscoring the potential efficacy of povidone–iodine even in infections caused by virulent organisms. These results complement prior rabbit model studies demonstrating that a single intravitreal injection of povidone–iodine was effective against vancomycin-resistant E. faecalis endophthalmitis. 17
These results align with prior studies demonstrating the intraocular safety of povidone–iodine in both animal and human studies. Intravitreal concentrations up to 0.025% have shown bactericidal activity without evidence of retinal toxicity.18–20 Povidone–iodine has also been shown to be an effective adjunct in vitrectomy irrigation and in combination with intravitreal injection. In a series of 12 patients with endophthalmitis undergoing PPV with 0.025% povidone–iodine added to the infusion fluid, significant visual improvement was observed without adverse effects. 13 Similarly, Nakashizuka et al14,15,20 treated 8 patients with intravitreal 1.25% povidone–iodine followed by PPV using 0.025% povidone–iodine in the irrigation solution, reporting visual improvement in 7 of 8 cases without evidence of ocular toxicity on electroretinography, endothelial cell density measurement, or visual field testing. As in our series, their cohort included a patient with E. faecalis endophthalmitis who experienced dramatic improvement in vision. Notably, vitrectomy was performed in all patients in that study, limiting conclusions about the efficacy of intravitreal povidone–iodine as monotherapy. Similar to our findings, Tanaka et al 16 reported a case of endogenous endophthalmitis in a patient who was unable to undergo vitrectomy and was treated with intravitreal povidone–iodine and systemic antibiotic therapy. The patient responded well and showed resolution of symptoms.
Our findings extend these observations by suggesting that intravitreal povidone–iodine monotherapy delivered in the office setting may be associated with favorable outcomes in selected cases, without the need for immediate surgical intervention or use of systemic antibiotics.
Our findings also highlight the benefits of povidone–iodine monotherapy in patients with antibiotic allergies. In many cases, these allergies are not adequately documented or lack objective confirmation. 21 For this patient population, therapeutic options may be limited, and delays in identifying and obtaining a safe alternative antimicrobial agent may adversely affect visual outcomes. This delay is especially concerning given that some causative bacteria can double in number in under 30 minutes, with each hour of inadequate antimicrobial coverage potentially worsening outcomes. 22
As an accessible, broad-spectrum antimicrobial agent that is not structurally related to conventional antibiotics, povidone–iodine may provide a potential immediate solution for managing acute endophthalmitis without the risk of hypersensitivity reactions or the development of antimicrobial resistance. In our study, all patients responded well to a single povidone–iodine injection. In the absence of clinical improvement, we would have proceeded with PPV as the next step in management.
In addition to being useful in specific clinical scenarios, such as in patients with unverified or complex antibiotic allergies, povidone–iodine may help address broader challenges in the management of ophthalmic infections. Although intraocular cultures remain the diagnostic gold standard, their sensitivity is limited, and results may be delayed. 8 The use of intravitreal povidone–iodine in our series allowed us to provide immediate, broad-spectrum coverage independent of culture confirmation or antimicrobial resistance profiles. Furthermore, povidone–iodine requires only a single injection, in contrast to the multiple intravitreal injections often required when empirically treating both bacterial and fungal etiologies. This approach may reduce patient discomfort in an already inflamed eye.
Finally, povidone–iodine may help address the increasingly common challenge of limited access to essential antibiotics worldwide. 23 Unlike many conventional antibiotics, povidone–iodine is inexpensive, stable at room temperature, widely available, and not associated with the development of antimicrobial resistance. 9 These characteristics make it particularly valuable in both high- and low-resource settings. 16 Rising resistance rates among ocular isolates of Staphylococcus aureus and coagulase-negative Staphylococcus species, exceeding 50% in some regions, and emerging vancomycin resistance, further emphasize the importance of exploring nonantibiotic treatment alternatives.24–27
This study has several limitations, including its retrospective design, small sample size, and lack of a control group. Variability in prior surgical history and baseline VA among patients may also have influenced outcomes. In addition, the average follow-up duration of 10 months limits conclusions regarding the long-term safety and efficacy of intravitreal povidone–iodine therapy. Larger, prospective, randomized studies are warranted to define optimal dosing, refine patient selection criteria, establish long-term safety, and directly compare intravitreal povidone–iodine with standard intravitreal antibiotics.
This case series represents, to our knowledge, the largest reported cohort of exogenous endophthalmitis managed with in-office intravitreal povidone–iodine monotherapy. Our findings suggest that intravitreal injection of 1.25% povidone–iodine (0.1 mL) is a potentially effective and accessible therapeutic option for acute exogenous endophthalmitis. Treatment was associated with rapid symptom relief, resolution of inflammation, and significant visual improvement, without observed complications. Although limited by the small sample size and retrospective design, these findings support the consideration of intravitreal povidone–iodine as an alternative or bridging therapy when conventional antibiotics are contraindicated, delayed, or unavailable.
Footnotes
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the institutional review board (IRB) of the University of Puerto Rico Medical Sciences Campus in San Juan, Puerto Rico, USA (IRB approval number: 2506420922).
Statement of Informed Consent
Written informed consent for enrollment and publication was obtained from each study participant.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. L.A. Berrocal serves as a consultant for Apellis, and Dr. M.H. Berrocal serves as a consultant for Alcon and Genentech. None of the other authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.