
Abstract
Introduction
Vitreous cysts are a rare ocular finding, with only a limited number of cases reported in the literature. The first description of a vitreous cyst was published in 1899. 1 Vitreous cysts are typically classified as congenital or acquired and further characterized as pigmented or non-pigmented, and fixed or free-floating entities. Diagnosis is frequently missed, as many patients remain asymptomatic. In this report, we present a pediatric case of bilateral vitreous cysts arising from the non-pigmented ciliary body epithelium and fixed to the far temporal pars plana, with asymmetry in size between the eyes. The larger cyst was associated with a cataract, deep amblyopia, cystoid macular edema (CME), and retinal dragging. We also briefly review the current understanding and management of this condition.
Case Report
A 5-year-old boy presented to the emergency department for an ophthalmology consultation after a failed vision screening. He was initially examined by a local optometrist, who noted a possible retinal hole in the right eye and a cataract in the left eye, prompting referral to the emergency department. The patient’s past medical history was unremarkable; he was born full term and was meeting appropriate developmental milestones. His guardian reported that the patient’s left eye was more light sensitive and that he frequently rubbed it. Otherwise, no visual disturbances were reported.
Upon examination at our facility, the patient’s visual acuity (VA) was 20/30 in the right eye and limited to counting fingers in the left eye. The eyes were orthotropic. Examination under anesthesia revealed intraocular pressures of 13 mm Hg OD and 12 mm Hg OS. The corneas were clear, the anterior chambers were deep and quiet, and the pupils were round and reactive in both eyes (Figure 1, A and B). The right eye lens was clear, but a dense 3+ posterior subcapsular cataract was seen in the left eye. Cycloplegic refraction in the right eye was +3.00 +2.50 × 090, while refraction could not be obtained in the left eye.
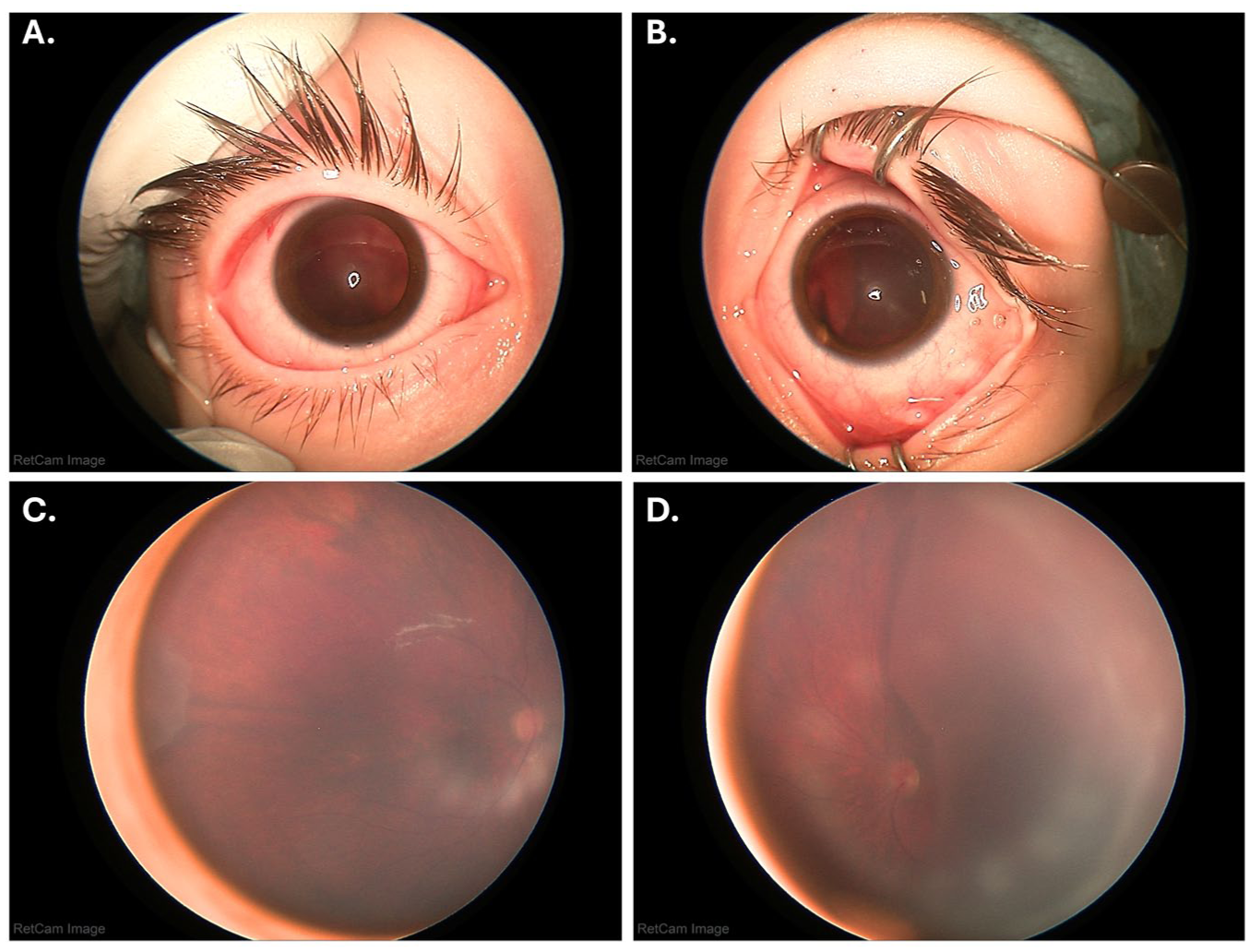
RetCam photographs. (A) Right eye anterior segment. (B) Left eye anterior segment demonstrates a cyst visible behind the lens. (C) Right eye posterior segment shows a vitreous cyst in the temporal periphery adjacent to the long ciliary nerve. (D) Left eye posterior segment demonstrates a large vitreous cyst obscuring the macula and occupying the temporal half of the vitreous cavity.
Dilated fundus examination revealed a normal posterior pole in the right eye; however, a small, gray, partially translucent cyst was noted along the long ciliary nerve, anterior to the equator in the temporal periphery (Figure 1C). The left eye demonstrated a large gray, partially translucent, somewhat mobile cyst occupying about 60% to 70% of the vitreous cavity and occluding the entire temporal retina (Figure 1D). The optic nerve and nasal retina appeared grossly normal.
B-scan ultrasonography demonstrated enclosed hyperechoic cysts with an anechoic center (Figure 2). Axial lengths measured using A-scan ultrasonography were 21.94 mm OD and 22.64 mm OS. Magnetic resonance imaging of the brain and orbits, with and without contrast, was unremarkable. Laboratory evaluation, including complete blood count and comprehensive metabolic panel, was within normal limits. Serologic testing for cysticercosis, toxoplasma, rubella, syphilis, herpes simplex virus, cytomegalovirus, and human immunodeficiency virus was negative. Based on these findings, the patient was diagnosed with bilateral vitreous cysts, along with a visually significant cataract and deep amblyopia in the left eye.
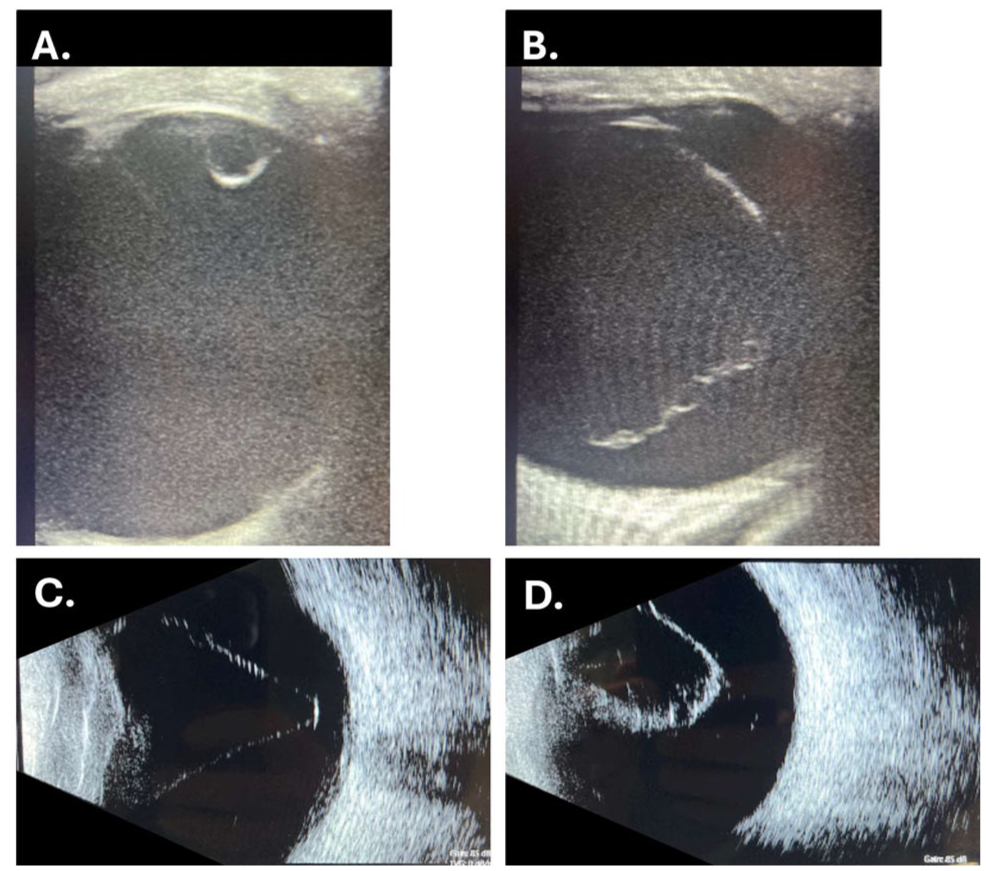
B-scan ultrasonography images show a well-circumscribed cyst with a hyperechoic wall and internal hollowness. (A) Right eye. (B–D) Left eye.
We decided to proceed with lensectomy, pars plana vitrectomy (PPV), and cyst sampling of the left eye. The excised cyst was sent for cytologic evaluation, which revealed a benign-appearing cyst lined by sheaths of cuboidal and spindle cells with bland oval nuclei, without evidence of necrosis or mitosis (Figure 3). The cells had focal attachments to dense vitreous. The epithelial cells had no pigmentation, and there was no evidence of atypia or malignancy. Immunohistochemical staining showed positivity for vimentin, cytokeratin cocktail, and S100, and negativity for smooth muscle actin, glial fibrillary acidic protein, paired box gene 8, human melanoma black 45, and synaptophysin. Together, these findings suggest a cyst originating from the non-pigmented ciliary body epithelium.
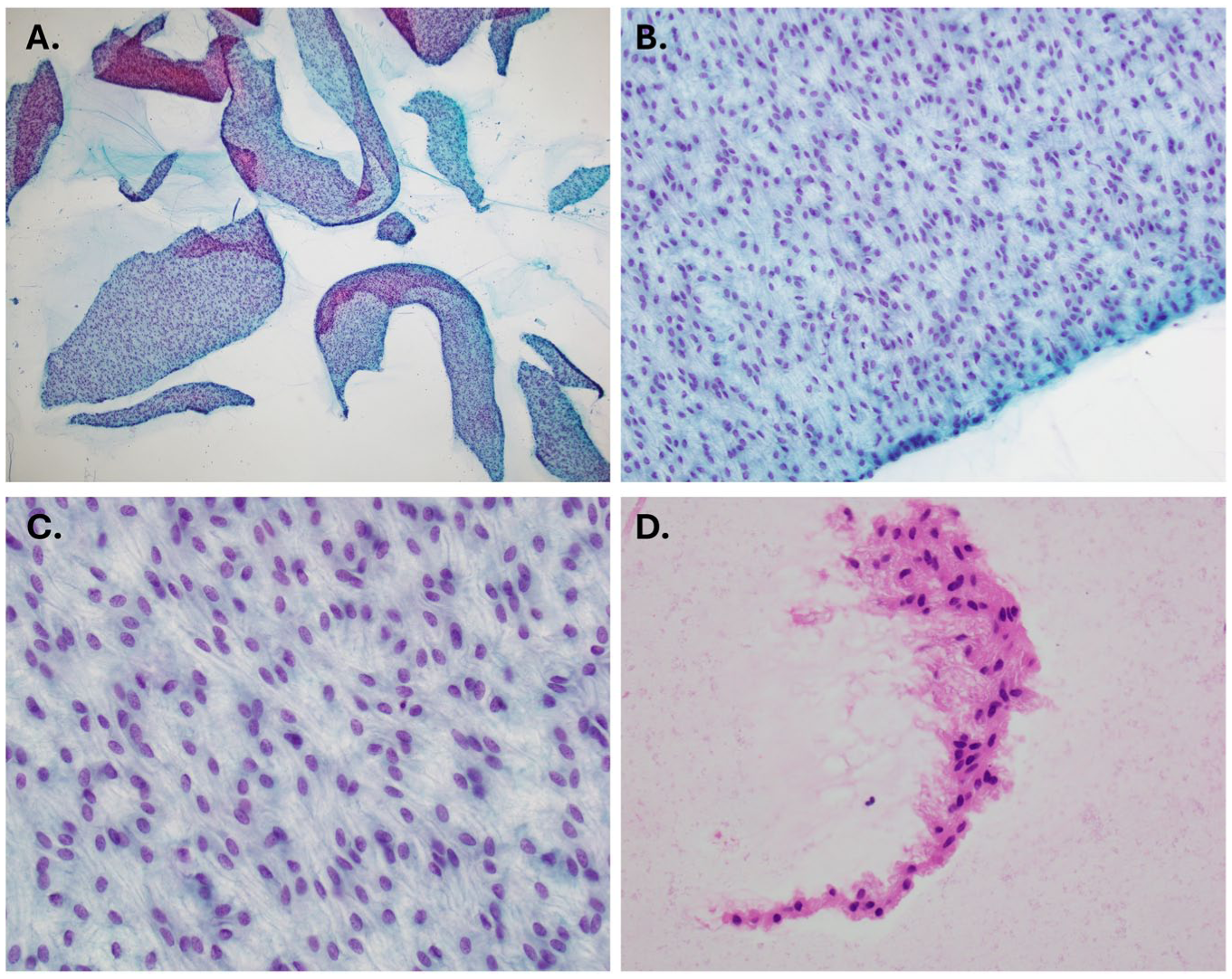
Histopathology slides. (A–C) Papanicolaou stain at different magnifications (40×, 200×, and 400×, respectively) showing benign-appearing sheaths of cuboidal and spindle cells with bland oval nuclei and focal vitreous attachments, without necrosis or mitosis. (D) Cell block section, paraffin-embedded, stained with hematoxylin and eosin stain (400×), shows strips of 1 to 4 layers of bland epithelial cells focally resembling non-pigmented ciliary body epithelium.
Following surgery, the patient’s VA was 20/30 OD and 20/400 OS. He was fitted with an aphakic contact lens and initiated occlusion therapy with patching of the right eye for amblyopia treatment. At a postoperative visit, once the ocular media had cleared, examination revealed blunting of the foveal reflex and blurring of the nasal margins of the optic nerve head in the left eye (Figure 4). The patient subsequently underwent macular optical coherence tomography, which demonstrated poor foveation, CME, and mild optic nerve head edema in the left eye (Figure 4).
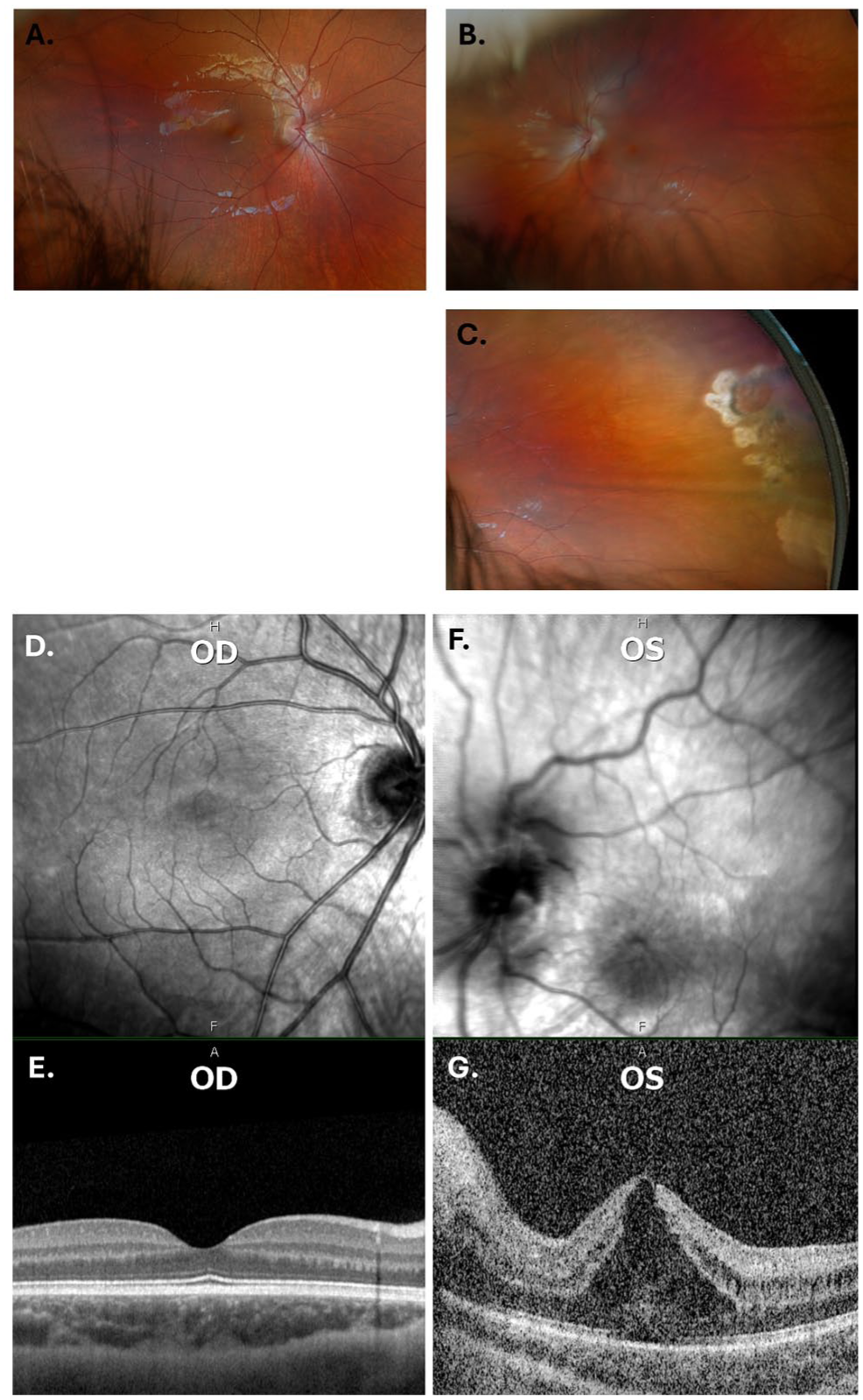
(A–C) Color fundus photographs at postoperative month 2. (A) Right eye macula with unremarkable findings. (B) Left eye macula demonstrates a blunted foveal reflex and blurring of optic nerve head margins. (C) Left eye temporal periphery shows laser spots surrounding areas of retinal thinning and pigmentary changes. (D–G) Macular optical coherence tomography. (D, E) Right eye with unremarkable findings. (F, G) Left eye demonstrates poor foveation, notable cystoid macular edema, elevated optic nerve head, and inferior displacement of the fovea.
Conclusions
Vitreous cysts are an uncommon ocular condition, with only a limited number of cases reported in the literature. They are usually identified incidentally in patients aged 10 to 20 years. 2 Our case is notable because it involves a 5-year-old child presenting with significantly decreased vision. In this patient, it remains unclear whether the large vitreous cyst contributed to the cataract development or whether the cyst and cataract occurred as concurrent congenital entities.
Vitreous cysts are usually asymptomatic but may occasionally present with photophobia, transient blurred vision, or moving shadows in the field of vision when the cyst intermittently crosses the visual axis. 2 In contrast to previously reported cases, our patient was unique in demonstrating bilateral cysts that were sessile, with attachments to the temporal peripheral retina and pars plana. In addition, adjacent chorioretinal scars were present at the sites of adhesion, and the macula of the left eye was obscured by the size of the cyst.
The etiology of primary vitreous cysts remains unclear. In many congenital cases, it is speculated that these cysts originate from incomplete regression of the hyaloid vascular system. Therefore, cysts are often found in Cloquet’s canal, and other hyaloid remnants, such as a Bergmeister papilla or Mittendorf dot, may be observed on examination. 3 Other primary cysts have been proposed to arise from the iris, ciliary body, or retinal pigment epithelium, based on similarities in cellular structure and function.4–6
In contrast, acquired vitreous cysts have been reported in association with various conditions, including ocular trauma, choroidal atrophy, retinitis pigmentosa, retinal detachment, retinoschisis, ciliary body adenomas, and uveitis.2,7–10 In our case, the cysts were located symmetrically in the temporal periphery of both eyes and originated from the ciliary body, a finding confirmed by biopsy. This finding provides new insight into the origin of congenital vitreous cysts, supporting the possibility that they may arise from ciliary body epithelium, a mechanism that has rarely been confirmed.
Vitreous cysts may be slightly pigmented or non-pigmented and are typically semi-translucent.10–12 In our case, the cyst was non-pigmented. Notably, optic nerve head edema and macular edema have not previously been described as clinical manifestations of benign vitreous cysts. Owing to the large size of the cyst, the macula was not visible until right after the surgery; postoperative examination revealed inferior foveal displacement. Chronic vitreous traction can cause retinal and macular swelling, which may explain these findings. 13 While the cyst was somewhat mobile, it had firm posterior attachments to the temporal peripheral retina, suggesting that associated vitreous adhesions may have contributed to the observed macular changes.
While modern surgical techniques have reduced the incidence of postoperative CME in pediatric patients, it is also possible that the macular edema observed in this patient developed as a postoperative complication.14–16
Diagnosis should be made carefully, as vitreous cysts must be differentiated from infectious and neoplastic masses, which carry significantly greater morbidity. Infectious etiologies include cysticercosis, toxoplasmosis, toxocariasis, and echinococcosis. Among these, intraocular cysticercosis typically presents as a cyst containing turbid fluid with an internal scolex. On B-scan ultrasonography, these cysts usually display denser internal echogenicity compared with benign vitreous cysts. 8 In our case, imaging studies and systemic laboratory evaluation did not reveal evidence of infectious and malignant causes, effectively ruling out these alternative diagnoses.
Treatment of vitreous cysts typically depends on the patient’s symptoms and degree of visual impairment. As most vitreous cysts tend to be asymptomatic, they can usually be managed with observation and periodic monitoring. 17 In selected cases where the cyst is visually significant, laser photocoagulation has been used to shrink the cyst.18–20 However, laser treatment may not be suitable if the cyst is tethered near the visual axis or is very large, 21 as treatment in these situations may risk retinal damage or may be ineffective. In such cases, PPV is the preferred treatment option.4,5
In conclusion, vitreous cysts are an exceedingly rare ocular finding and are typically asymptomatic. In this report, we present a 5-year-old child with photophobia and decreased vision in 1 eye who was found to have bilateral congenital vitreous cysts. Notably, one cyst was large enough to obscure the macula and was associated with a visually significant cataract in that eye. The cysts in both eyes were sessile, with adhesions to the temporal pars plana and adjacent to chorioretinal scarring. The child was treated with lensectomy and PPV. Histopathologic evaluation revealed cuboidal and spindle cells, consistent with an origin from the non-pigmented ciliary body epithelium. The postoperative course was notable for the development of CME and foveal dragging.
Footnotes
Ethical Approval
Our institution does not require ethical approval for the publication of individual case reports or case series.
Statement of Informed Consent
The authors certify that they have obtained appropriate verbal and written informed consent from the patient’s guardian. Consent was provided for the publication of clinical information and images in this journal. The guardian understands that the patient’s name and initials will not be published and that efforts will be made to conceal the patient’s identity; however, complete anonymity cannot be guaranteed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.