
Abstract
Keywords
Introduction
Dislocation of intraocular lenses (IOL) can occur shortly after complicated cataract surgery or often years after routine cataract surgery. The latter type of dislocation, which appears to be an increasingly common clinical entity, represents a unique clinical condition related to the techniques of modern phacoemulsification surgery.1,2 An editorial from the Journal of Cataract and Refractive Surgery described the condition as a potential “ticking time bomb” related to the continually increasing incidence of this condition due to the prevalence of pseudophakia and time-dependent tendency for dislocation. 3 Because the condition is generally progressive, often evolving from a highly symptomatic partial to complete dislocation, surgical management is typically indicated.
There is currently no consensus on the best management options for correcting IOL dislocations. 4 When exchange is performed, the IOL–capsular bag complex is first migrated into the anterior chamber, bisected with intraocular scissors, and removed via a limbal or clear corneal incision. Pseudophakia can then be reestablished through a number of techniques, including anterior chamber IOL implantation, scleral suturing of an appropriate IOL, 5 externalized haptic technique of a 3-piece IOL, 6 or iris fixation. A technique with superior outcomes has not yet been established. 7
Alternatively, retention, reposition, and fixation of the existing IOL–capsular complex to the iris or sclera can be done. This method of repair has the inherent advantages of less traumatic surgery and lower associated costs due to the avoidance of the explantation/implantation and wound creation steps, a shorter surgical time, and reuse of the IOL. Another potential advantage is the preservation of the capsular bag. In 2017, Dillon et al 8 described a procedure for iris fixation of dislocated in-the-bag IOLs. Because most implanted IOLs are single-piece acrylic, 9 and these are generally not tolerated when placed outside the capsular bag, reusing them could be of concern. We hypothesize that the presence of an intact, enveloping capsule can protect against complications of uveitis-glaucoma-hyphema (UGH) syndrome and allow safe reuse of the single-piece acrylic IOL.
The current report presents the early and later complications of the repositioning and iris suturing of late single-piece acrylic IOLs that are within an intact capsular bag. Late complications include the UGH spectrum of conditions, such as cystoid macular edema (CME), retinal detachment (RD), IOL redislocation, and corneal edema. In addition, we compare the outcomes of this technique with the standard technique of direct iris suturing of a 3-piece IOL not associated with a capsular bag.
Methods
A retrospective chart review was conducted of patients who underwent iris suture fixation surgery for IOL dislocation by a single retinal physician between January 2018 and September 2024. The New York University institutional review board granted exemption for this study, and this research adhered to the tenets of the Declaration of Helsinki. Informed consent was established before surgery.
The surgical technique for iris fixation of dislocated in-the-bag IOLs has been described previously. 8 There are important aspects of the surgical technique to emphasize. First is the use of posterior infusion to shallow the anterior chamber, thereby stabilizing the IOL bag complex. Second, the need to identify the haptic positions such that they are included in the suture loop. Third, long suture passes to incorporate the haptics and capsular elements. This technique differs significantly from the tighter suture for iris fixation of the smooth, nonencapsulated polymethyl methacrylate haptics of 3-piece IOLs. Finally, an iridectomy is indicated, with attention to the removal of lens material, which may occlude flow. For the 3-piece IOLs not within a capsule, the lens was elevated to an optic capture position and fixated with standard iris suture technique (Figure 1, A and B). Single-piece acrylic lenses that were not within an intact capsule were exchanged by bisecting the lens with intraocular scissors, removing it through a 3-mm corneal incision, and implanting a 3-piece lens secured with iris suture fixation or other fixation methods not described here. Only patients with at least 6 months of postoperative follow-up were included.
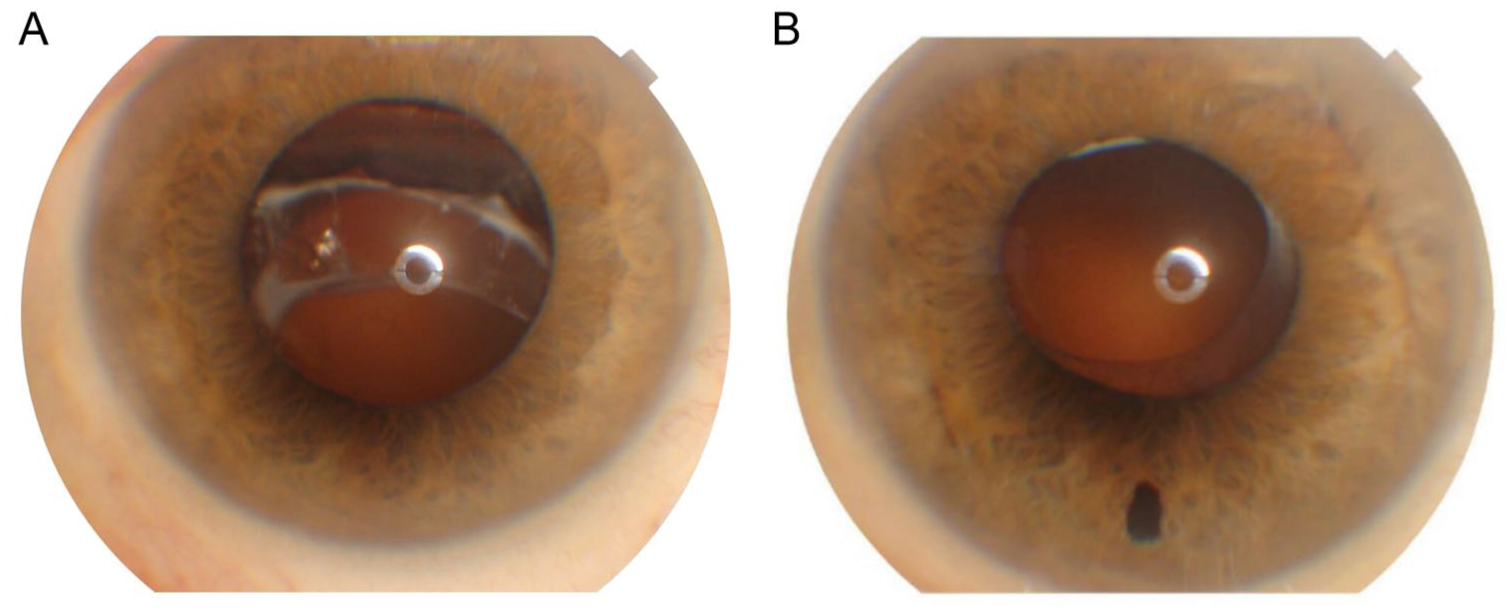
Representative (A) preoperative and (B) postoperative slitlamp photographs of an in-the-bag single-piece acrylic intraocular lens dislocation managed with iris suture fixation.
Medical records for each patient were reviewed for age, type of IOL used for iris fixation, in-the-bag vs out-of-the-bag dislocation, history of trauma, high myopia ≥6.0 diopters, prior pars plana vitrectomy, and pseudoexfoliation. Ocular examinations with Snellen visual acuity (VA), tonometry, slitlamp biomicroscopy, and optical coherence tomography (OCT) imaging of the macula were performed on all patients at both preoperative and postoperative visits.
Outcomes of interest included postoperative uveitis, ocular hypertension (defined as intraocular pressure [IOP] ≥30 mm Hg), CME, hyphema, vitreous hemorrhage (VH), and RD. Complications were recorded only if present after 6 weeks postoperatively and were evaluated at 3 timepoints: ≥6 weeks, ≥3 months, and ≥12 months postoperatively. Due to variability in follow-up adherence, not all patients were evaluated at each timepoint. Some patients presented for an initial postoperative visit at 3 months or later, resulting in higher patient counts at later timepoints, while others were lost to follow-up before 12 months; patients were sometimes followed by their referral doctors. CME was defined as intraretinal cysts visible on OCT. Two-sample t tests were used to compare continuous variables, while χ2 or Fisher exact tests, as appropriate, were applied to compare categorical variables between in-the-bag and out-of-the-bag groups. All statistical analyses were performed using R (R Foundation for Statistical Computing).
Results
A total of 140 eyes of 132 patients were included in the study. Eight patients had both eyes with dislocated IOLs at different timepoints (Table 1). Age and sex were analyzed at the patient level, whereas VA and follow-up duration were assessed per eye. Average follow-up time was similar between groups at 29.0 and 24.5 months, respectively. The average patient age was 76.5 ±10.5 years (range, 57.6-96.5), and age at presentation was significantly greater in patients presenting with in-the-bag dislocations (P < .001). Preoperative VA was significantly worse (P = .003) for patients experiencing out-of-the-bag dislocations. Patient sex was not significantly different between the 2 groups.
Demographic and Eye-Level Characteristics for In-the-Bag and Out-of-the-Bag IOL Dislocations.
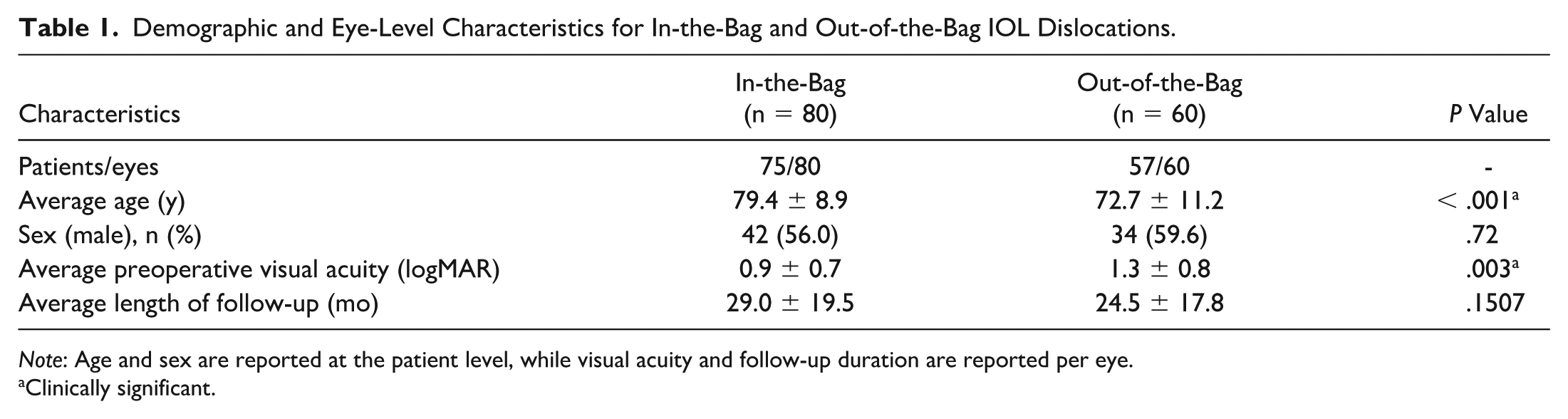
Note: Age and sex are reported at the patient level, while visual acuity and follow-up duration are reported per eye.
Clinically significant.
Thirty-nine eyes (27.9%) that underwent iris suture fixation surgery had pseudoexfoliation, which was significantly associated with having an in-the-bag IOL dislocation (P < .001). No other preoperative risk factors were significantly different among the 2 groups (Table 2).
Clinical Features Between Eyes With In-the-Bag and Out-of-the-Bag IOL Dislocations.
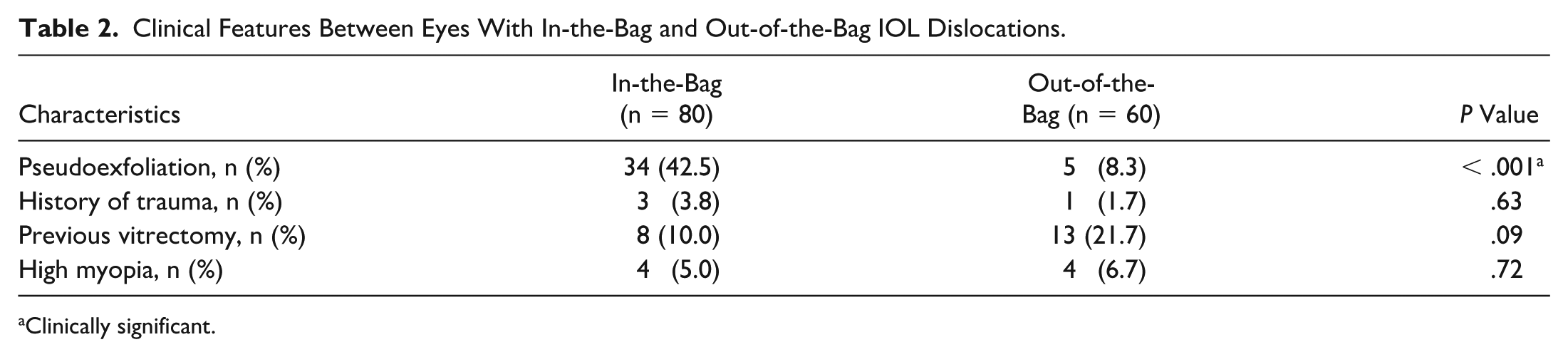
Clinically significant.
Complications were tracked for 3 timepoints: ≥6 weeks postoperatively, ≥3 months postoperatively, and >12 months postoperatively. The differing n values at each timepoint are attributable to variability in follow-up adherence. Complications were only recorded if present after 6 weeks, but 11 eyes were not evaluated beyond postoperative day 1 until at least 3 months after surgery, while 46 eyes were lost to follow-up before 12 months.
A total of 50 eyes (35.8%) experienced at least 1 postoperative complication, including 7 eyes (5.0%) with anterior uveitis, 10 (7.1%) with ocular hypertension, and 38 (27.1%) with CME. VH occurred in 2 cases, 1 in a patient with an out-of-the-bag dislocation and the other in a patient with an in-the-bag dislocation who also experienced the study’s only case of hyphema. No cases of RD were observed.
Patients with postoperative uveitis were treated with steroid drops, and those with ocular hypertension were placed on IOP-lowering drops. At the time of last follow-up, all instances of these complications had resolved. A combination of prednisolone acetate and ketorolac drops was used for patients presenting with CME. The percentage of patients with CME decreased to 6.4% by the last follow-up, 78% (7 of 9) of which were asymptomatic and had VA >20/40.
Overall, there was no statistical difference in postoperative complication rate between eyes with in-the-bag or out-of-the-bag IOL dislocation at either 6 weeks (P = .71), 3 months (P = .84), or 12 months (P = .18). Fisher exact tests for each individually tracked complication found no statistically significant differences between groups at any time point (Table 3). In total, 5 eyes experienced re-subluxation of the lens and required secondary operations. Postoperative complications were counted for these eyes after the second repeat surgery.
Postoperative Complications After Iris Suture Fixation Surgery With In-the-Bag and Out-of-the-Bag IOL Dislocations.
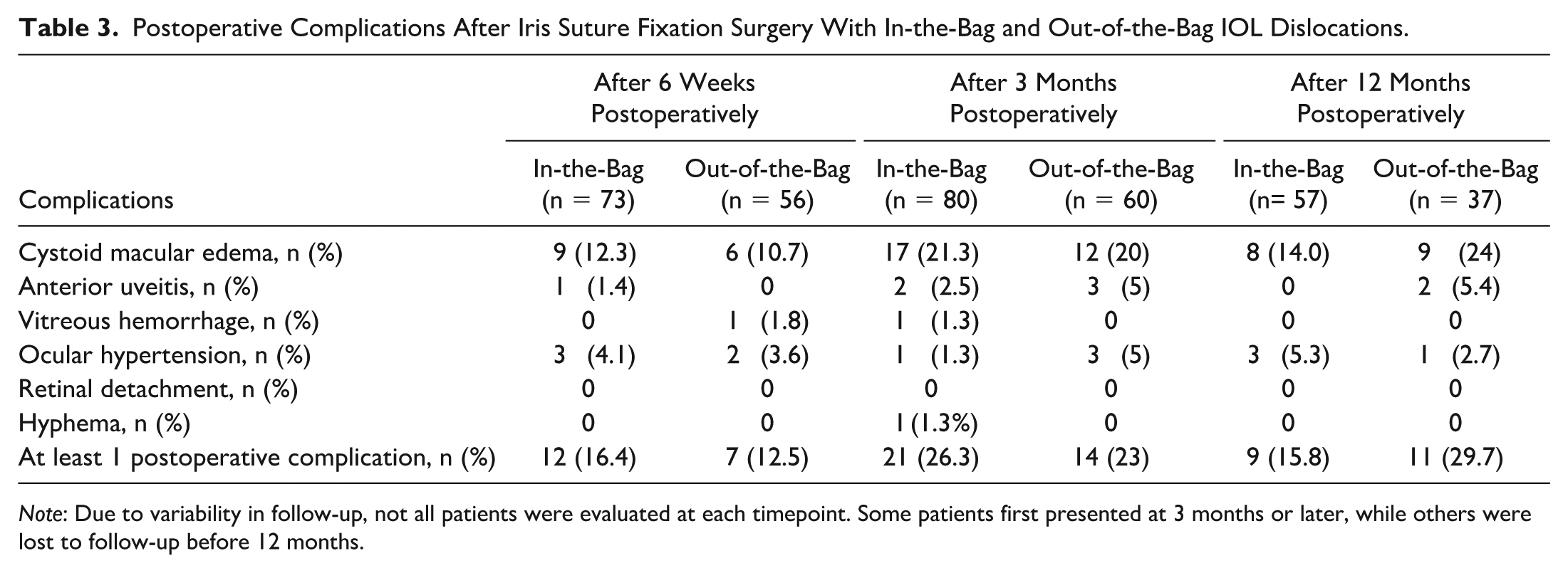
Note: Due to variability in follow-up, not all patients were evaluated at each timepoint. Some patients first presented at 3 months or later, while others were lost to follow-up before 12 months.
Conclusions
It has long been known that, unlike vaulted, 3-piece IOLs with rounded polymethyl methacrylate or polyvinylidene fluoride haptics, single-piece acrylic IOLs cannot be safely placed in the ciliary sulcus or in contact with uveal tissue. However, we have shown that by preserving the capsular bag, a single-piece acrylic can be retained and fixated with a complication rate similar to the standard practice of 3-piece IOL fixation. However, because the vast majority of late IOL dislocations are with single-piece acrylic IOLs, explantation of the lens has been the general method of repair. The explantation sequence includes migrating the IOL bag complex into the anterior segment (often made difficult due to its large diameter and relative pupillary miosis), dissociating the capsular bag and the accumulated lens material from the IOL, and then bisecting (or folding) the IOL to allow removal through a 3.0- to 3.5-mm incision. This is followed by reimplanting a new IOL, which can be fixated by a variety of techniques. These explantation steps are associated with possible iris trauma, corneal endothelial cell loss, vitreous traction with secondary rhegmatogenous consequences, and often protracted or repetitive intraoperative hypotony and its associated risks—especially relevant in the typically affected older adult population. Preservation of the existing IOL requires only the reposition and refixation steps.
Due to the high prevalence and duration of pseudophakia, the incidence of late in-the-bag dislocations is on the rise. Studies have shown that this risk increases over time, with a cumulative risk of IOL dislocation after cataract extraction of 0.1% after 10 years and 1.7% after 25 years. 10 The expected increase in incidence of this condition makes finding a safe and efficient surgical solution essential.
In the current study, VA was significantly different at presentation for in-the-bag vs out-of-the-bag dislocations because most out-of-the-bag dislocations often presented within days of the complex cataract surgery. Associated pathology such as corneal edema, vitreous opacities (blood or lens fragments), or inflammation was typical. In contrast, in-the-bag dislocations typically occurred long after otherwise uncomplicated surgery.
There was a statistically significant difference in age between patients with in-the-bag vs out-of-the-bag IOL dislocations, which was expected. Although the age at the time of cataract surgery was likely equivalent between the 2 groups, out-of-the-bag dislocations typically result from acute surgical complications, whereas in-the-bag dislocations often occur several years postoperatively. Pseudoexfoliation is a risk factor for both early and late IOL dislocation but is more commonly associated with late in-the-bag dislocations. 11 Davis et al 2 explored the role of pseudoexfoliation, specifically for late in-the-bag dislocation, and found that patients with pseudoexfoliation presenting with dislocation were an average of 6 years older than patients without pseudoexfoliation, consistent with our findings.
The high incidence of CME in the current study may be related to the detection technique, compared with that of other reported techniques. We defined CME as any eye exhibiting intraretinal fluid by OCT imaging on any postoperative visit. In our study, spectral-domain or swept-source OCT imaging was performed at each postoperative visit. Using only slitlamp biomicroscopic or VA screening for CME would result in a low incidence. Furthermore, if we used OCT only for those eyes with diminished vision, low incidence would be reported because most of the eyes with CME detected by OCT had good acuity and were asymptomatic. Although a 27.1% rate of CME is slightly higher than some other studies related to IOL dislocation, a 20% to 30% rate of CME after ophthalmic surgery is not uncommon. 12 Additionally, the rate of CME decreased to 9.6% after the 12-month follow-up period, which is similar to previously reported complication rates. 13 Hemorrhagic complications were rare in both groups, consistent with previous studies.14,15 There was 1 case of hyphema, and only 2 patients developed VH early in the postoperative period, both of which were transient. No late-occurring hemorrhages (UGH spectrum) were detected.
One weakness of the current study is the loss of patients to follow-up. UGH syndrome can often occur years after the etiologic operative procedure, 16 and 46 of the original 140 eyes included in the study were not evaluated after 12 months. Perhaps no study of the various surgical techniques for IOL fixation has fully captured the long-term complications due to the sporadic and often late onset of UGH complications. In addition, the iris suture technique has not been compared with the scleral suture fixation techniques, which would allow preservation of the lens capsule.
In conclusion, the late in-the-bag, single-piece acrylic IOL dislocation is an increasingly common condition and represents a challenging surgical problem. Dislocations of single-piece acrylic IOLs are generally considered inappropriate for refixation; however, we have shown that if the single-piece acrylic is within an intact capsule, it is as safe as the 3-piece IOL long used for iris fixation surgery. The implication is that it may be prudent to retain these lenses within the intact capsule and suture fixate to either the iris or possibly the sclera (not studied here), rather than perform an exchange procedure that requires multiple additional complex surgical steps. In addition, the capsular bag would, logically, seem to provide a natural insulation, preventing IOL uveal contact and UGH spectrum complications.
Footnotes
Ethical Approval
This study was granted expedited ethical approval by the New York University Institutional Review Board (IRB study reference number i19-00478). This is an IRB-approved retrospective chart review study; all patient information was de-identified, and patient consent was not required. Patient data will not be shared with third parties.
Statement of Informed Consent
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.