
Abstract
Introduction
Inflammation is a fundamental defense response of the body to injury or infection and involves the interaction of multiple cellular and molecular mechanisms. 1 When inflammation develops in ocular tissues and becomes persistent beyond the physiologic response, the visual prognosis can be adversely affected by the resulting pathologic processes. 2 At the retinal and vitreous level, the inflammatory response is characterized by the release of various cytokines and growth factors, which disrupt ocular homeostasis, induce structural alterations, and trigger fibrotic processes. These changes may lead to macular wrinkling, retinal tears, and tractional complications, ultimately limiting treatment success.3–5
The fundamental mechanism of ocular inflammation involves disruption of the balance between intracellular and extracellular signaling factors. This imbalance triggers inflammatory cascades, enhances cellular proliferation, and ultimately leads to fibrotic remodeling within ocular tissues. 6
Intraocular inflammation (IOI) is a complex, multifactorial process involving a wide range of cytokines and growth factors. 7 Among these, transforming growth factor-β has been extensively studied for its role in inflammatory and fibrotic pathways. However, other mediators, such as fibroblast growth factor-2, platelet-derived growth factor, vascular endothelial growth factor (VEGF), granulocyte-colony stimulating factor, and epidermal growth factor, have also been implicated in this process.8,9 In addition, numerous studies have reported elevated levels of cytokines in intraocular tissue, including interleukin-1β, interleukin-6, tumor necrosis factor-α, interferon-β, and fibronectin. These mediators collectively contribute to cellular proliferation and tissue remodeling, underscoring the complexity of intraocular inflammatory mechanisms.10–15
Intraocular inflammatory and fibrotic processes that exceed physiologic capacity, particularly within the vitreous and retina, can lead to severe tractional changes. These changes may ultimately result in complications such as retinal tears and tractional or rhegmatogenous retinal detachment. 16 The primary treatment in such cases is surgical, typically involving vitrectomy combined with tamponade agents, and when necessary, retinotomy or retinectomy.5,17 In addition, several adjunctive pharmacologic strategies aimed at suppressing cellular proliferation and modulating inflammatory activity have been investigated, and these agents show potential for influencing tractional changes and fibrotic remodeling. 18
In the current study, we used nilotinib, a second-generation tyrosine kinase inhibitor that, to our knowledge, has not previously been evaluated for its efficacy in models of IOI. Nilotinib is widely used in the treatment of chronic myeloid leukemia and exerts its primary effects through inhibition of BCR-ABL and platelet-derived growth factor receptor-α, as well as other kinases involved in fibrotic and inflammatory pathways, including transforming growth factor-β, interleukin-1β, fibroblast growth factor-2, and VEGF.19–22 By inhibiting platelet-derived growth factor receptor-α, nilotinib may suppress downstream signaling cascades, such as the Smad pathway, which are implicated in fibrosis and extracellular matrix production. Compared with other tyrosine kinase inhibitors, such as dasatinib and imatinib, nilotinib demonstrates higher selectivity and potency for platelet-derived growth factor receptor inhibition, which may contribute to its antifibrotic effects.23,24 In the current study, we assessed the impact of nilotinib in a model of IOI, considering its broad kinase inhibition profile, established antifibrotic properties, and potential to modulate key signaling pathways involved in ocular fibrotic and inflammatory processes.19,25–27
Methods
This study received authorization from the ethics committee at Fırat University’s Faculty of Medicine on June 7, 2023 (no. 2023/11-08). A total of 21 Sprague-Dawley rats with an average weight of 250 g were randomly assigned to 3 groups. One eye was used from each of the 21 rats. Throughout the experiment, the rats were kept in specialized enclosures at the Fırat University Experimental Research Center and provided with appropriate feeding conditions. All methods were performed following ethical standards and complied with the tenets of the Declaration of Helsinki.
Throughout the study, rats in Group 1 (control) did not receive any treatments or injections. At the onset of the experiment, rats in Group 2 (sham) were administered 0.07 IU/0.1 mL dispase in a total volume of 0.1 mL. Additionally, a 0.1 mL intravitreal (IVT) dimethyl sulfoxide solution was injected during the eighth week. Similar to Group 2, rats in Group 3 (treatment) received 0.07 IU/0.1 mL dispase in 0.1 mL at the beginning of the experiment. However, in the eighth week, rats in this group were treated with 2 ng/μL IVT nilotinib.
Rats were euthanized in the eighth week, corresponding to the peak activity period of dispase in inducing IOI, and their eyes were subsequently enucleated. The levels of transforming growth factor-β, platelet-derived growth factor, fibroblast growth factor-2, VEGF, and interleukin-1β were evaluated with an enzyme-linked immunosorbent assay.
For anesthesia and analgesia, Groups 2 and 3 received a mixture of ketamine hydrochloride (Ketalar, Eczacıbaşı) at a dosage of 50 mg/kg and xylazine hydrochloride (Rompun, Bayer) at a dosage of 6 mg/kg. Nilotinib (Tasigna, Novartis) was dissolved in dimethyl sulfoxide to create a solution with a concentration of 2 ng/µL. Additionally, dispase (Sigma-Aldrich Chemie GmbH) was reconstituted in dimethyl sulfoxide to obtain a concentration of 0.07 IU/0.1 mL. All drug preparations were conducted in accordance with sterilization protocols. To prevent endophthalmitis, the ocular surfaces of each rat were disinfected with a 10% povidone-iodine solution before administering IVT injections. Subsequently, a 5% povidone-iodine solution was administered to the conjunctiva. After allowing at least 3 minutes for the povidone-iodine to act, a saline solution was used to rinse the conjunctival area of each rat.
Homogenization and Biochemical Evaluation
A total of 21 enucleated eyes were immersed in tubes containing 0.01 M phosphate-buffered saline (pH 7.4). The tissues, prepared at a weight-to-volume ratio of 1:9, were homogenized on ice at 4°C and subsequently centrifuged at 16 000 × g for 3 minutes. The resulting homogenates were then subjected to a second centrifugation at 5000 × g for 15 minutes at 4°C to isolate the supernatants. Protein concentrations in the supernatants were determined using the Lowry assay, 28 which relies on measuring the blue-colored complex formed between proteins and the folin-phenol reagent in an alkaline solution at 650 nm.
The concentrations in the supernatants of VEGF, transforming growth factor-β, platelet-derived growth factor, fibroblast growth factor-2, and interlekin-1β were measured following the manufacturers’ protocols using an enzyme-linked ımmunosorbent assay with specific kits for rats (BT Lab). Absorbance was measured spectrophotometrically at 450 nm using an Epoch 2 microplate reader (BioTek Instruments Inc). The measurement ranges and sensitivities for each analyte are as follows: VEGF: 10 to 3000 pg/mL, sensitivity 5.01 pg/mL; transforming growth factor-β: 10 to 2000 pg/mL, sensitivity 5.21 pg/mL; platelet-derived growth factor: 0.05 to 15 ng/mL, sensitivity 0.023 ng/mL; interleukin-1β: 1 to 300 pg/mL, sensitivity 5.4 pg/mL; fibroblast growth factor-2: 10 to 3000 pg/mL, sensitivity 5.36 pg/mL. All assays exhibited intra-assay coefficients of variation <8% and interassay coefficients of variation <10%. Results were quantified as picograms per milligram of protein (pg/mg protein).
All data analyses were performed using SPSS version 24 for Macintosh (IBM Corp). To assess differences between groups, the Kruskal-Wallis test, a nonparametric method of analysis of variance, was used. Pairwise comparisons were performed with the post hoc Tamhane test. Outcomes were deemed statistically significant when P < .05. In the descriptive analysis, continuous variables are presented with means and SDs, while categorical variables are shown as frequency counts (n) and percentages.
Results
Statistical comparisons among the 3 groups revealed that levels of interleukin-1β were significantly higher in Group 2 compared with Group 1 (P < .05). In contrast, Group 3 showed no significant differences compared with Group 1 (P = .134) or with Group 2 (P = .889). Levels of VEGF were significantly higher in Group 2 than in Group 1 (P < .05). No significant difference was found between Group 1 and Group 3 (P = .955) when comparing VEGF levels, nor between Group 2 and Group 3 (P = .564). A significant increase in platelet-derived growth factor was detected in Group 2 compared with Group 1 (P < .05); however, no significant variance was observed between Group 1 and Group 3 (P = .582) or between Group 2 and Group 3 (P = .529). Levels of transforming growth factor-β were significantly higher in Group 2 compared with Group 1 (P < .05). No significant differences were found between Group 1 and Group 3 (P = 0.996) or between Group 2 and Group 3 (P = .444). Significant differences in fibroblast growth factor-2 were identified between Group 2 and Group 1 (P < .05) as well as between Group 2 and Group 3 (P < .05). However, the comparison between Group 1 and Group 3 was not statistically significant (P = .673). The results of the biochemical parameters and statistical evaluations of the 3 groups are presented in Table 1.
Values of Biochemical Parameters of Groups.
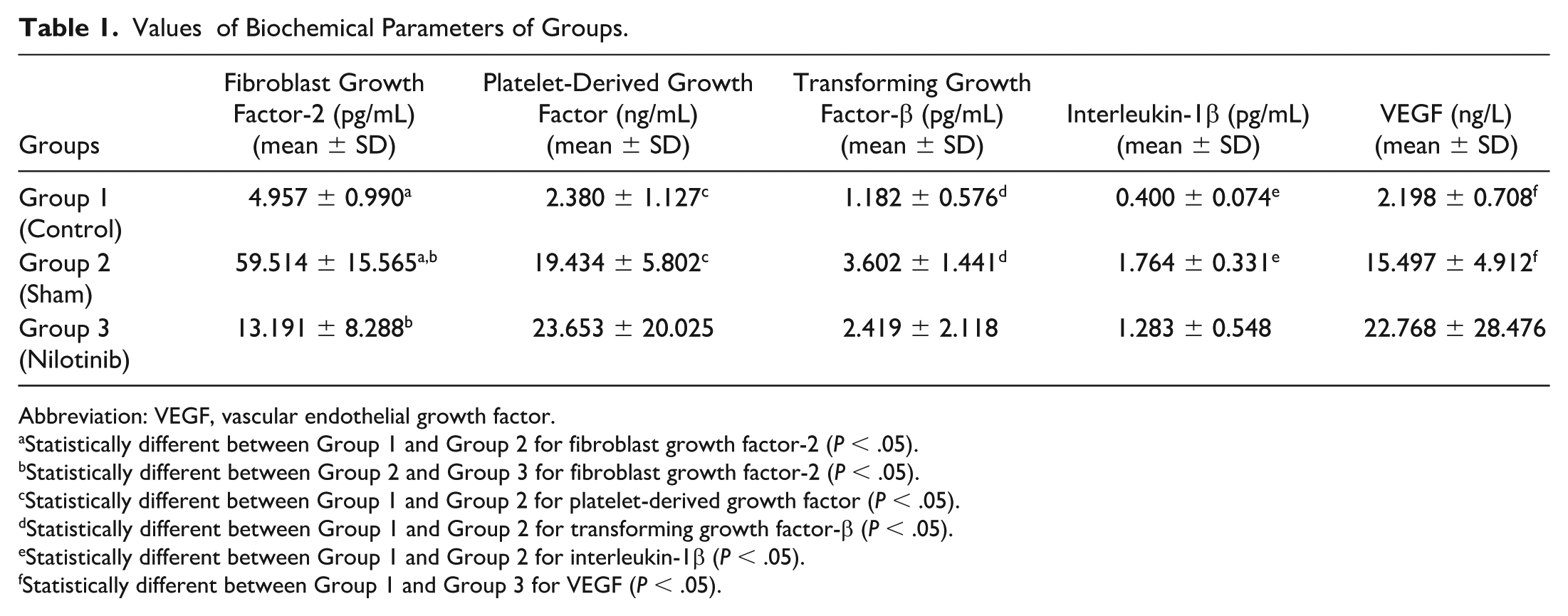
Abbreviation: VEGF, vascular endothelial growth factor.
Statistically different between Group 1 and Group 2 for fibroblast growth factor-2 (P < .05).
Statistically different between Group 2 and Group 3 for fibroblast growth factor-2 (P < .05).
Statistically different between Group 1 and Group 2 for platelet-derived growth factor (P < .05).
Statistically different between Group 1 and Group 2 for transforming growth factor-β (P < .05).
Statistically different between Group 1 and Group 2 for interleukin-1β (P < .05).
Statistically different between Group 1 and Group 3 for VEGF (P < .05).
Conclusions
In this study, we evaluated the biochemical effects of nilotinib in an experimental model of IOI. Our findings indicate that nilotinib may hold promise in this setting, particularly by reducing levels of fibroblast growth factor-2. Further investigations are needed to clarify its impact on fibroblast growth factor-2 and the role it plays in alleviating fibrosis, a key mechanism in intraocular inflammatory and fibrotic processes. Dispase, a proteolytic enzyme derived from Bacillus polymyxa, is a commonly used agent to induce IOI. It has been shown to be effective at doses of 0.05 to 0.07 IU/0.1 mL with an incubation period of 8 to 10 weeks. Dispase was chosen for this study due to its simplicity and cost-effectiveness.29–32
Nilotinib, a second-generation tyrosine kinase inhibitor that primarily targets BCR-ABL and platelet-derived growth factor receptor-α, was used in this study, as well as other kinases involved in fibrotic and inflammatory pathways, such as transforming growth factor-β, interleukin-1β, fibroblast growth factor-2, and VEGF.19–22 Although widely used in chronic myeloid leukemia, the efficacy of nilotinib in models of IOI has not been previously evaluated. Given its broad kinase inhibition and antifibrotic properties, the biochemical effects of nilotinib were analyzed in an experimental model of IOI.33,34
Fibroblast growth factor is a mitogenic agent present in epithelial, endothelial, and stromal cells that binds to high-affinity tyrosine kinase receptors on the cell membrane. By enhancing collagen synthesis, it significantly contributes to the progression of IOI.35–38 Although studies investigating nilotinib’s inhibitory effect on fibroblast growth factor-2 are limited, we are not aware of any ophthalmologic research specifically addressing this issue. Huber et al 22 reported a significant reduction in fibroblast growth factor-2 expression when nilotinib was applied to human papillomavirus cell cultures. In the current study, we assessed the influence of nilotinib on IOI and found that a 2 ng/μL dose effectively decreased fibroblast growth factor-2 levels. Additionally, Uslubas et al 39 investigated the effects of aflibercept, an anti-VEGF agent, in settings of IOI and demonstrated that retinal damage and subsequent fibrotic changes were inhibited. Our findings show that nilotinib at a dose of 2 ng/μL significantly reduces levels of fibroblast growth factor-2, which may be relevant to ocular fibrotic and inflammatory processes. Further studies and additional histopathologic investigations are needed to clarify nilotinib’s clinical potential.
Interleukin-1β is a cytokine central to the inflammatory process and plays a pivotal role in the pathophysiology of IOI. 40 Although multiple studies have shown that nilotinib decreases interleukin-1β levels, our review of the literature did not identify any ophthalmologic research investigating the impact of nilotinib on interleukin-1β. Rhee et al 26 demonstrated that nilotinib decreases interleukin-1β levels in an experimental pulmonary fibrosis model in mice. In our study, nilotinib also reduced interleukin-1β levels, but this decrease was not statistically significant. This may be due to interleukin-1β being regulated by multiple pathways, such as nuclear factor-κB and mitogen-activated protein kinase, beyond platelet-derived growth factor receptor signaling, so platelet-derived growth factor receptor inhibition alone may not sufficiently suppress interleukin-1β in IOI. 41 Further studies are needed to clarify the effects of nilotinib on these inflammatory pathways in experimental models of IOI.
Platelet-derived growth factor stimulates endothelial and fibroblast migration and enhances fibroblast responsiveness to transforming growth factor-β.42–45 Yıldırım et al 46 reported that nilotinib reduced platelet-derived growth factor levels in their experimental corneal neovascularization model in rats. In our study, nilotinib reduced platelet-derived growth factor levels in the model of IOI, but this decrease was not statistically significant. This may be attributed to repeated IVT procedures, which can stimulate platelet-derived growth factor release and maintain elevated levels in the vitreous. Additionally, compensatory mechanisms involving other growth factors or cytokines, such as fibroblast growth factor and transforming growth factor-β, may counteract the reduction in platelet-derived growth factor, thereby limiting the overall effect of nilotinib.
Transforming growth factor-β has been widely studied for its involvement in cell migration, proliferation, and contraction, all of which contribute to the pathogenesis of inflammation. 47 Various studies have demonstrated that nilotinib reduces the expression of transforming growth factor-β. For instance, to inhibit postoperative fibrosis in patients with glaucoma, nilotinib was shown to decrease transforming growth factor levels in cultured human Tenon capsule fibroblasts. 48 In our study, nilotinib reduced transforming growth factor-β levels in the model of IOI, but this decrease was not statistically significant. This may be because transforming growth factor-β is regulated by multiple pathways, such as Smad and mitogen-activated protein kinase, 49 so platelet-derived growth factor receptor inhibition alone may not be sufficient. Further studies are needed to clarify the anti-transforming growth factor-β effects of nilotinib in intraocular inflammatory and fibrotic processes.
VEGF, which regulates cell proliferation and vascular permeability, is significantly increased in the vitreous during IOI. 1 Yıldırım et al 46 found that nilotinib reduced VEGF levels in a rat model of corneal neovascularization. In our study, nilotinib also decreased VEGF levels in IOI, but this reduction was not statistically significant. The lack of a significant decrease may be due to the involvement of multiple cytokines and growth factors in intraocular inflammatory pathways, which can compensate for each other. 50 Additionally, temporal and spatial variability in VEGF expression, as well as the timing of sampling and the local microenvironment, may have influenced the results. Further studies are needed to clarify these findings. 51
To evaluate the cytokines implicated in the pathogenesis of intraocular inflammation, our study compared the control group with the sham group. We observed a statistically significant elevation in the levels of transforming growth factor-β, interleukin-1β, fibroblast growth factor-2, VEGF, and platelet-derived growth factor (P < .05). These findings emphasize the critical role of these cytokines and growth factors in driving intraocular inflammatory processes. In this context, nilotinib demonstrated a notable biochemical effect by significantly reducing fibroblast growth factor-2 levels, although its effect on other cytokines was not statistically significant.
Several studies have investigated the effects of tyrosine kinase inhibitors in models of ocular disease. Umazume et al 52 first demonstrated that dasatinib inhibited retinal pigment epithelium changes associated with IOI in a porcine model. Similarly, Tamiya et al 53 reported that tyrosine kinase inhibitors suppressed epithelial-mesenchymal transition and retinal pigment epithelium cell migration, indicating potential therapeutic value in ocular fibrotic and inflammatory processes. Consistent with these findings, we used nilotinib in a model of IOI and observed improvements in biochemical markers, particularly a significant reduction in fibroblast growth factor-2 levels.
A notable limitation of this study is that it focused solely on cytokine levels and did not include anatomic endpoints, which are important in fibrotic ocular diseases. Additionally, IVT injections used to induce and treat IOI may have contributed to inflammatory responses due to procedural trauma, potentially influencing the study outcomes. Another limitation is that the IVT half-life of nilotinib remains unknown. Future research should incorporate advanced imaging modalities and histopathologic analyses to comprehensively elucidate the structural and antifibrotic effects of nilotinib in experimental models of IOI.
Footnotes
Acknowledgements
We would like to express our gratitude to Prof. Dr. Fatma Ülkü Çeliker, head of the Department of Ophthalmology at Firat University Faculty of Medicine, for her invaluable support throughout our study.
Ethical Approval
This research received authorization from the ethics committee at Fırat University Faculty of Medicine, June 7, 2023, numbered 2023/11-08.
Statement of Informed Consent
No human subjects were involved in this study; therefore, informed consent was not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.