
Abstract
Introduction
Retinitis pigmentosa (RP) is the most common inherited form of blindness in the world, affecting an estimated 1 in 4000 individuals.1,2 It is a clinically and genetically heterogeneous group of inherited retinal disorders characterized by diffuse progressive dysfunction of rod photoreceptors with subsequent degeneration of cone photoreceptors and the retinal pigment epithelium (RPE). Initial loss of rods leads to nyctalopia and visual field constriction in the early phases of the disease. In later stages, the loss of cones manifests as severe visual loss and loss of color discrimination.1–3
Although severe visual acuity (VA) loss due to cone degeneration occurs late in RP, cystoid macular edema (CME) may contribute to the early impairment of VA. Increased central macula thickness in RP patients with CME is a risk factor for lower VA.4–7 Various treatments for RP-associated CME have been reported, but there is limited evidence regarding their efficacy.8,9 Beyond its impact on VA, the presence of CME in patients with RP is frequently one of the exclusion criteria for interventional clinical trials evaluating novel treatments. 10
Prior studies have shown that the prevalence of CME in patients with RP varies from 8% to 77% depending on the diagnostic method.11–13 However, the only big population study to date evaluated CME in the setting of cataract surgery and showed that patients with RP have a higher risk of developing CME after cataract surgery than patients without RP. 14 Therefore, further population studies are needed to understand the characteristics of CME in patients with RP in the United States. This study aims to evaluate the prevalence and characteristics of CME in patients with RP utilizing one of the largest samples available with representation from clinics across the US: the American Academy of Ophthalmology IRIS Registry.
Methods
This retrospective cohort study used data derived from the IRIS Registry from January 1, 2013, through April 14, 2023. The IRIS Registry is a centralized data repository and reporting tool that can be used for research purposes. 15 The data were aggregated in a de-identified manner, with methodology mirroring other IRIS Registry–based research, and investigators did not have access to study identifiers. Because data were de-identified, the study was exempt from approval by the Mass General Brigham Institutional Review Board. This study adhered to the tenets of the Declaration of Helsinki.
All patients with a diagnosis code for RP were included in this study, based on International Classification of Diseases, Tenth Revision (ICD-10) coding. Code H35.52 for pigmentary retinal dystrophy is widely used as specific for a diagnosis of RP. 14 Only patients with 2 or more records of this ICD-10 code on 2 or more separate clinic visits, as well as a minimum of 1 follow-up visit recorded at least 60 days after the RP diagnosis, were included. To reduce intereye correlation for analyses, we randomly selected 1 eye per patient with bilateral RP. We report results based on this final sample.
Among the eyes retained in the study for analysis, we evaluated patient demographics (age, gender, race, and ethnicity as documented in the electronic health record), as well as smoking status at the time of RP diagnosis, VA per eye, and geographic region. Secondary clinical diagnoses based on ICD-10 codes (Supplementary Table S1) were also extracted, including CME, epiretinal membrane (ERM), vitreomacular traction (VMT), any degree of diabetic retinopathy, and retinal vein occlusion. We also evaluated cataract surgery, vitrectomy, and Nd:YAG laser capsulotomy based on Current Procedural Terminology and Healthcare Common Procedural Coding System codes (Supplementary Table S1).
The primary outcomes of interest were the proportion of eyes having CME and, within the CME vs non-CME groups, the proportion of eyes having ERM, VMT, diabetic retinopathy, retinal vein occlusion, cataract surgery, vitrectomy, and Nd:YAG laser capsulotomy. We also assessed the distribution of these factors in RP eyes with CME compared with RP eyes that did not have CME. Patient characteristics were summarized using frequencies and percentages. Demographics in the groups were compared using Pearson chi-square test for categorical variables and the Wilcoxon rank-sum test for any continuous variables.
We employed a multivariate logistic regression model to evaluate associations between patient characteristics and CME occurrence, reporting odds ratios (ORs) with 95% CIs. P values were adjusted for multiple comparisons using the Benjamini-Hochberg correction. We compared mean and median best-corrected VA values between eyes with RP and between RP eyes with or without CME (for eyes with CME diagnosed within 90 days of RP) at the time of RP diagnosis and 2 years (±3 months) after diagnosis of RP using a Wilcoxon rank-sum test. All analyses were conducted in R statistical programming software (version 4.3.1). For all analyses, P values less than .05 were considered statistically significant.
Results
Study Population
In the IRIS Registry, between January 1, 2013 and April 14, 2023, a total of 50 219 patients had a diagnosis of RP and met the inclusion criteria. In analyzing 1 eye per patient among these 50 219 patients, 8495 (16.9% of eyes) had CME. Table 1 shows the characteristics of the patients retained for analysis in our study. The majority of patients were female (57%, n = 28 638). The median age of the study population was 58 years (interquartile range [IQR], 43-69 years). Most patients were White (66.0%, n = 32 963), followed in order of prevalence by Black or African American patients (11.0%, n = 5373) and Asian patients (3.7%, n = 1838). Race was not recorded for 8684 patients (17.0%). Hispanic patients represented 10.0% of the study population (n = 5043). The regional representation of patients included 21 035 (42.0%) from the South, 9766 (19.0%) from the North Central, 10 090 (20.0%) from the West, 8499 (17.0%) from the Northeast, 468 (0.9%) with missing information (marked as Unknown). A total of 29 597 patients (59.0%) had never smoked, while 6207 (12.0%) were former smokers, 4262 (8.5%) were active smokers, and 10 153 (20.0%) did not have their smoking status documented. A total of 9758 eyes (19.4%) had ERM, 1326 eyes (2.6%) had VMT, 2300 eyes (4.6%) had diabetic retinopathy, 576 eyes (1.1%) had retinal vein occlusion, 8579 eyes (17.1%) had cataract surgery, 4700 eyes (9.4%) had Nd:YAG laser capsulotomy, and 558 eyes (1.1%) had pars plana vitrectomy.
Characteristics of Patients With New-Onset RP With or Without CME in the IRIS Registry Between 2013 and 2023.
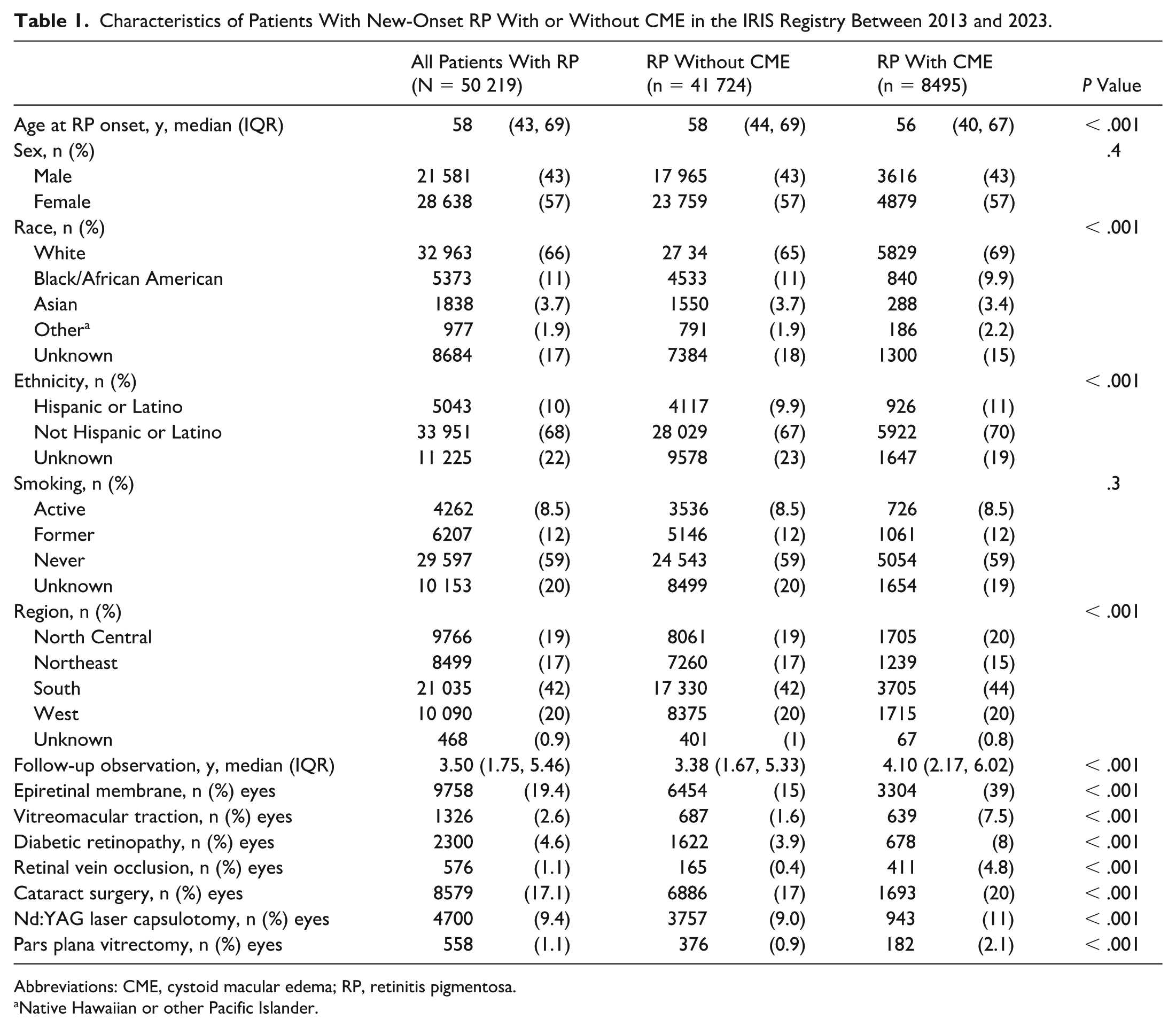
Abbreviations: CME, cystoid macular edema; RP, retinitis pigmentosa.
Native Hawaiian or other Pacific Islander.
Differences in Characteristics of Eyes With RP Based on CME Diagnosis
The median age of patients with CME (56 years) was younger than that of patients without CME (median, 58.0 years; P < .001). The proportions of male patients (43.0%) and female patients (57.0%) were equal between patients with RP with and without CME, with 4879 female patients in the CME group and 23 759 in the no CME group and 3616 male patients in the CME group and 17 965 in the no CME group.
ERM was significantly more frequent in RP eyes with CME (39.0%) than in RP eyes without CME (15.0%; P < .001). In addition, VMT was more frequent in RP eyes with CME (7.5%) than in RP eyes without CME (1.6%; P < .001). Similarly, diabetic retinopathy and retinal vein occlusion were significantly more frequent in RP eyes with CME (8% and 4.8%, respectively) than in RP eyes without CME (3.9% and 0.4%, respectively; P < .001). Cataract surgery and Nd:YAG laser capsulotomy were more frequent in RP eyes with CME (20% and 11%, respectively) than in RP eyes without CME (17% and 9.0%, respectively; P < .001). Finally, pars plana vitrectomy was more frequent in RP eyes with CME (2.1%) than in RP eyes without CME (0.9%; P < 0.001).
Factors Associated With CME in Eyes With RP
Multivariate logistic regression analysis revealed that longer follow-up duration for eyes included in the analysis was associated with increased odds of CME (OR, 1.09, 95% CI, 1.08–1.10). On the other hand, odds of CME occurrence decreased with increased age (OR, 0.90, 95% CI, 0.89–0.91 per decade above age 60 years). Black/African American and Asian patients had decreased odds of CME (OR, 0.90, 95% CI, 0.82–0.98 and OR, 0.80, 95% CI, 0.70–0.92, respectively) compared with White patients. Eyes with RP and ERM or VMT had increased odds of CME compared with those without a history of ERM or VMT (OR, 3.01, 95% CI, 2.85–3.18 and OR, 2.49, 95% CI, 2.18–2.84, respectively). In addition, eyes with RP and diabetic retinopathy or retinal vein occlusion had increased odds of CME compared with those without a history of diabetic retinopathy or retinal vein occlusion (OR, 1.22, 95% CI, 1.09–1.38 and OR, 4.77, 95% CI, 3.81–5.98, respectively). Similarly, eyes with RP that underwent cataract surgery or pars plana vitrectomy had increased odds of CME compared with those that did not undergo these procedures (OR, 1.18, 95% CI, 1.10–1.27 and OR, 1.66, 95% CI, 1.36–2.03, respectively). We did not find a significant association between Nd:YAG laser capsulotomy and CME in eyes with RP (OR, 1.05, 95% CI, 0.97–1.14). All results are shown in Table 2 and Figure 1.
Likelihood of Developing CME by Predictive Factor in Patients With New-Onset RP in the IRIS Registry Between 2013 and 2023.
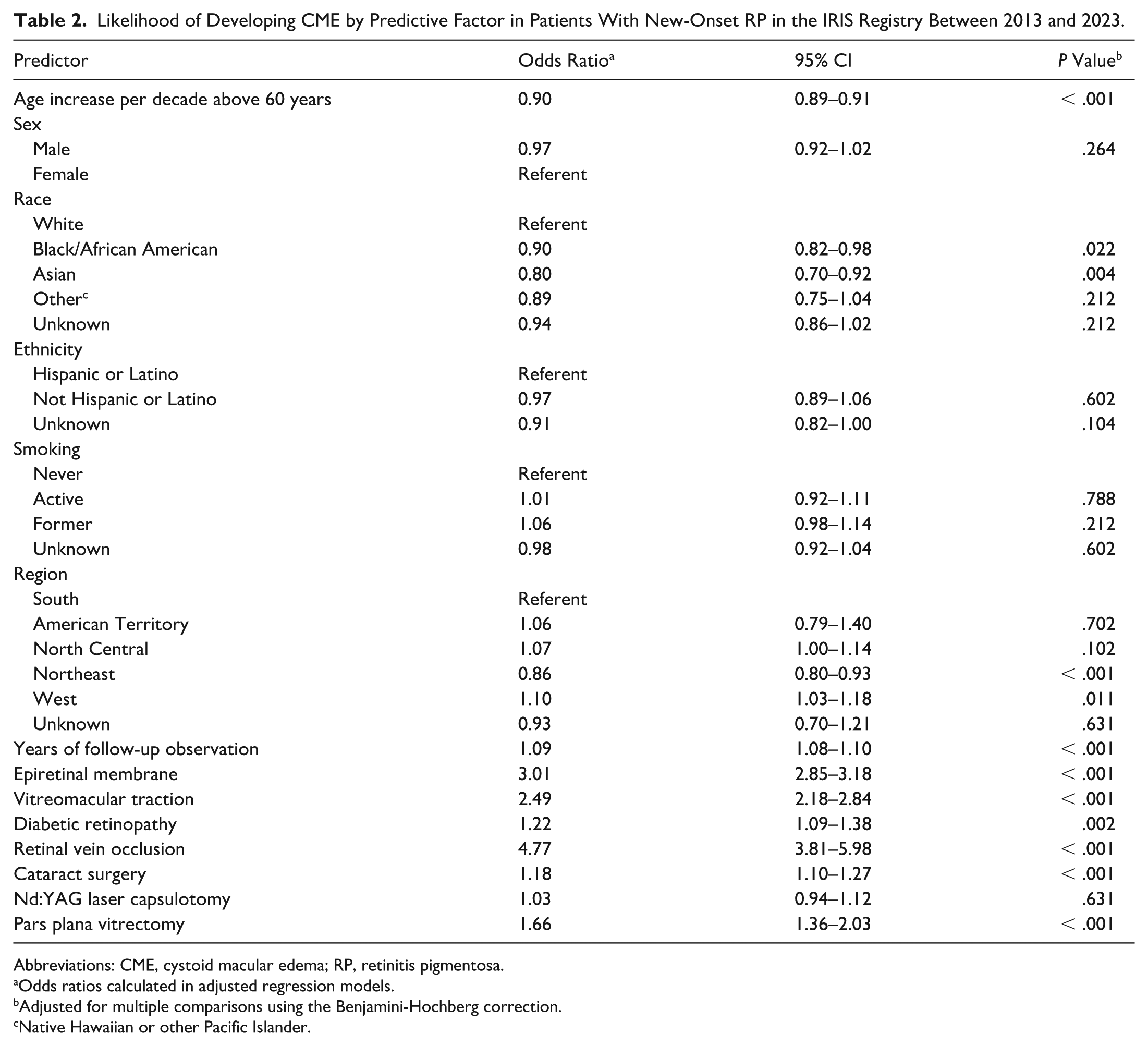
Abbreviations: CME, cystoid macular edema; RP, retinitis pigmentosa.
Odds ratios calculated in adjusted regression models.
Adjusted for multiple comparisons using the Benjamini-Hochberg correction.
Native Hawaiian or other Pacific Islander.
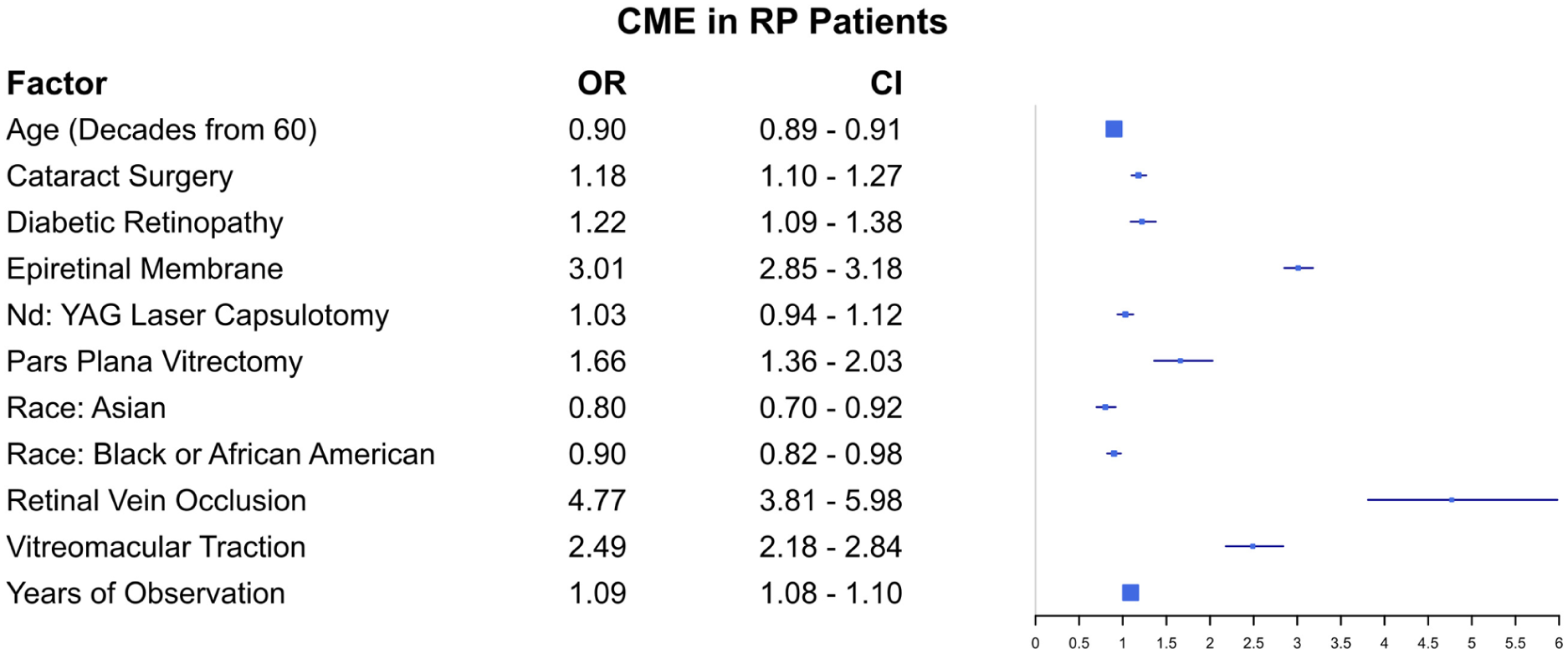
Forest plot showing the odds ratios (OR) with 95% CIs for the likelihood of developing cystoid macular edema (CME) associated with each predictor in eyes with retinitis pigmentosa (RP).
Visual Acuity in Eyes With CME
Data on VA of patients with RP at the time of diagnosis with CME and 2 years thereafter were available for 16 325 patients (30 314 eyes; 32.5% of patients). Among these eyes, 3956 patients (13.1%) had CME. At the time of CME diagnosis, best-corrected VA was worse for RP eyes with CME (median, 0.3 logMAR [IQR, 0.15-0.48]) than in those without CME (median, 0.18 logMAR [IQR, 0.05-0.48]) (Figure 2). Similarly, best-corrected VA at 2 years after CME diagnosis was worse for RP eyes with CME (median, 0.3 logMAR [IQR, 0.14-0.54]) than in those without CME (median, 0.18 logMAR [IQR, 0.05-0.54]) (Figure 2).
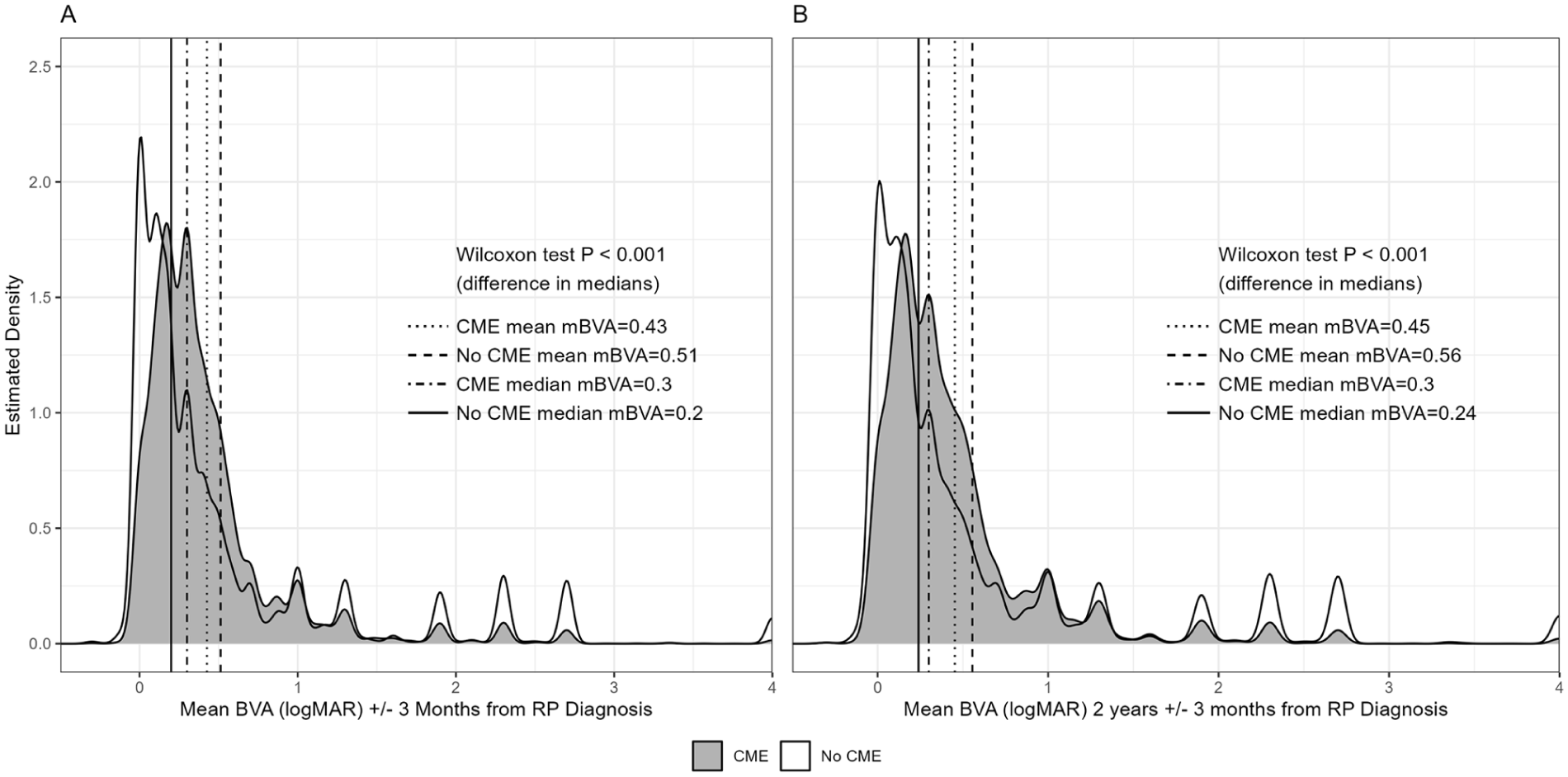
Distribution of mean and median best-corrected visual acuity (BVA) values (in logMAR) computed at (A) the time of diagnosis (0 years ± 3 months) and (B) 2 years ± 3 months after diagnosis in patients with retinitis pigmentosa (RP) with cystoid macular edema (CME) or without CME, as estimated using Kernel density estimation. Density of values was higher, and logMAR values were lower in the no CME group compared with the CME group in both time periods. This difference was statistically significant, as determined by Wilcoxon rank-sum test.
Discussion
The large scale of the IRIS Registry offers a valuable opportunity to investigate the prevalence and features of CME in patients with RP across the US. Our data revealed that 16.9% of eyes with RP had CME. Increased age, as well as Black or African American race and Asian race, was associated with a decreased risk of CME, whereas increased observation time, ERM, VMT, diabetic retinopathy, retinal vein occlusion, cataract surgery, and pars plana vitrectomy in patients with RP were associated with increased odds of CME. Nd:YAG laser capsulotomy was not associated with increased odds of CME. The VA of RP eyes with CME was worse than the VA in those without CME, measured at the time of CME diagnosis and at 2 years after diagnosis.
Past research studying CME prevalence in patients with RP has shown varying rates of CME, which may be partly attributable to the testing modality used. One study demonstrated that fluorescein angiography detected dye leakage indicative of CME in 14% to 77% of patients with RP, with higher rates likely influenced by the detection techniques and the criteria used. 11 However, not all clinically evident CME shows fluorescein leakage. 11 Optical coherence tomography is more sensitive than clinical examination and fluorescein angiography in identifying CME.16–18 In studies involving cohorts of 200 or more patients with RP, CME has been detected using optical coherence tomography in approximately 8% to 38% of the patients, with an average frequency of approximately 25%.5,6,19,20 Our large cohort study revealed that 16.9% of eyes with RP had a diagnosis of CME. The lower rate of CME observed in our study may be attributed to the ophthalmologists’ infrequent use of the CME ICD-10 code if the CME is considered clinically insignificant or does not require treatment. In addition, the lack of standardized criteria to identify CME on optical coherence tomography in patients with RP can lead to a significant variation in the rate of CME, as previously shown.11,17,21
Variable results have been reported regarding the association of RP-associated CME with age and gender, with some studies showing no significant relationship. 6 Other studies reported that macular abnormalities in patients with RP, such as CME, are more common in older patients and in female patients. 19 In contrast, another study showed that CME was associated with younger age but not with gender. 13 A recent large study of insurance claims data in the US showed that, after cataracts surgery, CME developed in patients with RP 3.9 weeks later than in patients without RP and was more common in male patients, but age was not linearly associated with the development of CME in these patients. 14 Our data showed that increased observation time was associated with increased odds of CME, suggesting that routine longitudinal monitoring of patients with RP is important for early detection and treatment of CME. In addition, we showed that older age was associated with a decreased CME occurrence, whereas sex was not. Further studies are needed to investigate the relationship between age and sex Black and CME in patients with RP. To the best of our knowledge, no prior studies have examined the association between CME and race and ethnicity. However, a study using the IRIS Registry to evaluate the risk of CME following cataract surgery found that patients had a higher risk of CME compared with White patients, while Asian patients had a lower risk compared with White patients. 22 Our study revealed that both Black/African American patients with RP and Asian patients with RP exhibited a decreased risk of CME compared with White patients with RP. Further studies are warranted to better understand these associations.
ERM and VMT are vitreomacular interface disorders that are frequently seen in patients with RP.11,13,23,24 The prevalence of ERM in patients with RP ranges between 10.5% and 35% depending on multiple variables, such as the genotype, the criteria employed, and the population studied.11,13,23,24 VMT can be detected in 2.5% of patients with RP. 24 Our data showed that 19.4% and 2.6% of eyes with RP had ERM and VMT, respectively, which is similar to the frequencies reported in prior studies. Patients with RP and CME have previously been reported to have higher rates of these vitreomacular interface disorders than patients with RP without CME, 6 leading to the hypothesis that these conditions are contributing factors to CME in patients with RP.6,11,25 Interestingly, however, other studies have reported that patients with RP and ERM are less likely to have CME and CME after cataract surgery,13,14 indicating the complexity of understanding whether ERMs play a role in the pathophysiology of RP and CME. Our data revealed that ERM and VMT are associated with higher odds of CME (ORs of 3.01 and 2.49, respectively), suggesting a possible role for vitreomacular interface disorders in CME in patients with RP. However, our data do not differentiate CME associated solely with RP from CME secondary to VMT or ERM, which are more prevalent in RP, and causation cannot be inferred from these data.
As expected and similar to patients without RP, 26 our data showed that diabetic retinopathy and retinal vein occlusion were associated with increased odds of CME in eyes with RP. Pseudophakia and intraocular surgery, in general, are risk factors for CME. 11 A large cohort study of patients with RP showed that the cataract surgery–related risk of CME in patients with RP was 4.83 times that of individuals without RP. 14 However, some studies suggest that cataract surgery does not increase the probability of CME in patients with RP.5,6,11,13 Our data revealed that eyes with RP having cataract surgery or pars plana vitrectomy at any point had increased odds of CME (ORs of 1.18 and 1.66, respectively), suggesting that intraocular surgery in patients with RP is associated with CME. On the other hand, Nd:YAG laser capsulotomy in eyes with RP did not increase the odds of CME. Further studies are needed to investigate the effect of intraocular surgery and procedures on CME in patients with RP, including assessing whether there is a time-limited impact on the odds of CME.
Variable results regarding the relationship between VA and CME in patients with RP have been reported. Several studies in patients with RP have failed to find a correlation between VA and the presence or absence of CME or between VA and central macular thickness, as measured with optical coherence tomography, in eyes with CME.6,11,16,17,21,27,28 On the other hand, other studies have found that patients with unilateral CME have significantly worse VA in the eye with CME as compared with the fellow eye 6 and that VA declines with increased central macular thickness in patients with RP,5–7,11,29 supporting the possible detrimental impact of CME on VA in patients with RP. Our data revealed that the VA of eyes with CME was worse than the VA of eyes without CME, both at the time of CME diagnosis and at 2 years after CME diagnosis, suggesting that CME may contribute to vision impairment in patients with RP and emphasizing the importance of monitoring patients for the development of this condition. However, our findings are significantly limited by the absence of VA data for a substantial proportion of RP and CME cases. Further studies are needed to evaluate the effect of CME on VA in patients with RP.
Our study is limited by several factors, including missing data, reliance on code-based data in the IRIS Registry (with inherent risk for coding imprecision or inaccuracies), lack of genetic testing results that can allow us to investigate the relationship between the genotype of RP and CME characteristics, lack of imaging data that can enable us to evaluate the features and severity of CME and whether it is solely due to RP or other underlying or coexisting conditions (such as ERM, VMT, retinal vein occlusion, or diabetic macular edema), and lack of clinical data to evaluate responses to treatment. In addition, although the IRIS Registry database has a very large number of unique patients, it does not include data from all practices in the US, particularly including many tertiary academic centers where many patients with inherited retinal disorders are followed up.
In conclusion, this large-scale analysis of patients with RP in the IRIS Registry demonstrates that CME was observed in 16.9% of eyes and that increased age was associated with a decreased risk of CME. On the other hand, increased observation time, ERM, VMT, diabetic retinopathy, retinal vein occlusion, cataract surgery, and pars plana vitrectomy were associated with increased odds of CME in eyes with RP. Nd:YAG laser capsulotomy did not show a relationship to CME. Finally, the VA of eyes with CME was worse than that of eyes without CME. Further studies are needed to investigate the epidemiology and risk factors of CME in patients with RP, as well as to evaluate treatment regimens and outcomes.
Supplemental Material
sj-xlsx-1-vrd-10.1177_24741264261438470 – Supplemental material for Prevalence and Risk Factors of Cystoid Macular Edema in Patients With Retinitis Pigmentosa in the United States: IRIS Registry Analysis
Supplemental material, sj-xlsx-1-vrd-10.1177_24741264261438470 for Prevalence and Risk Factors of Cystoid Macular Edema in Patients With Retinitis Pigmentosa in the United States: IRIS Registry Analysis by Ahmad Al-Moujahed, Eric Goldberg, Connor Ross, Kirill Zaslavsky, Tobias Elze, Lucia Sobrin, Joan W. Miller, Alice Lorch, Rachel Huckfeldt and Dan Gong in Journal of VitreoRetinal Diseases
Footnotes
Ethical Approval
This study was exempt from approval by the Institutional Review Board of Mass General Brigham because the analysis did not constitute human subject research. The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Statement of Informed Consent
Informed consent was not obtained because of the de-identified IRIS Registry data; investigators did not have access to study identifiers.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Miller has received financial support from Bausch + Lomb, Drusolv Therapeutics, Lowy Medical Research Institute, Massachusetts Eye and Ear Clinical Data Science Institute, ONL Therapeutics, QLT, and Sumitomo Pharma America, Inc, and. No conflicting relationship exists for any other author.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Elze was partially supported by NIH grant P30 EY003790. Dr. Lorch was supported by the Massachusetts Eye and Ear Clinical Data Science Institute.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.