
Abstract
Keywords
Introduction
Retinitis pigmentosa (RP) is a group of inherited retinal degenerations characterized by progressive photoreceptor dysfunction, primarily affecting rods and leading to gradual vision loss. It is one of the most common hereditary causes of blindness, with a global prevalence of approximately 1 in 3000 to 1 in 5000 individuals.1,2 Traditionally, the fundus findings in RP include bone spicule-like pigmentation, attenuation of retinal vessels, and waxy optic disc pallor; however, our recent study identified loss of peripheral retinal vessels as a consistent and objective feature, which may be more reliable than optic disc pallor. 3
Fluorescein angiography (FA) has previously been used to evaluate retinal vasculature in RP. Early FA studies from the 1970s described attenuation of peripheral retinal vessels, choroidal atrophy with associated pigment clumping, delayed fluorescein clearance in areas of choroidal vascular loss, and hyperfluorescent leakage involving the macula, optic disc, and vascular arcades.4–6 However, these studies were limited by the imaging technology available at the time, which allowed visualization of only approximately 30 degrees of the retina. Although some studies attempted to capture peripheral retinal images, a significant portion of the peripheral retina remained beyond the field of view.6,7
With the advent of ultra-widefield FA, imaging capabilities have vastly improved, allowing visualization of up to 200 degrees of the retina in a single capture. This expanded field of view enables a more comprehensive assessment of peripheral vascular changes in retinal diseases. While retinal vascular attenuation in patients with RP has been well documented at the posterior pole, peripheral vascular changes remain insufficiently characterized using modern imaging modalities. To our knowledge, no study has systematically evaluated the retina in patients with RP using ultra-widefield FA. Therefore, this study aims to provide a detailed assessment of both central and peripheral retinal vasculature in RP, with potential implications for diagnosis, disease staging, and therapeutic interventions.
Methods
This retrospective, cross-sectional study was conducted at an academic tertiary referral center. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Southern California. Patient data were de-identified before analysis, and the requirement for informed consent was waived. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. 8
Cohort Selection
Eligible patients included patients who underwent ultra-widefield FA at the USC Roski Eye Institute between April 2016 and April 2024. The study population consisted of patients with a confirmed diagnosis of syndromic or nonsyndromic RP. Diagnoses were established based on a combination of clinical symptoms, fundus findings, and, when available, electroretinography. Patients with suspected alternative inherited retinal diseases were excluded.
A comparator cohort included a group of age-matched controls who underwent ultra-widefield FA in the same time period for clinical indications unrelated to diffuse retinal vascular disease (eg, suspected central serous retinopathy, optic neuritis, macular drusen, myopic fundus evaluation, or subjective visual disturbances) and demonstrated no angiographic evidence of significant retinal vascular pathology. Patients with a history of retinal vascular disease, inflammation, retinal detachment, or any pathology that could alter the peripheral retinal structure or vasculature were excluded. Ultra-widefield FA was performed using the Optos California FA/ICG system (Optos Inc.). Only eyes with high-quality images, clear visualization of the retinal periphery, and adequate fluorescein filling were included.
Imaging Procedure
All images included in the study were acquired according to a standard procedure. Patients received an intravenous injection of 10% sodium fluorescein (Fluorescite; Novartis Pharma), and the camera timer was initiated simultaneously to record fluorescein transit times. Images were captured initially in the previously determined “transit eye,” with sequential images obtained at regular intervals of several seconds, followed by alternating between eyes for up to 6 minutes following dye injection. All imaging was performed by certified ophthalmic photographers at the USC Roski Eye Institute. Captured images were subsequently uploaded to OptosAdvance imaging software for further analysis.
In addition to FA, ultra-widefield pseudocolor fundus photography and FAF images, acquired concurrently, were used to correlate retinal lesions with angiographic findings.
Image Assessment
All angiographic features were independently assessed by 2 masked graders, and discrepancies were adjudicated by a fellowship-trained retina specialist. To account for any inadvertent delay between dye administration and the FA timer being started, transit times were measured relative to the initial appearance of choroidal vessels (choroidal flush) in the transit eye. Measured parameters included the time to appearance of dye in the central retinal artery (start of the arterial phase), the time to complete arterial filling within the central arcades and retinal periphery (arterial phase), and the time to complete venous filling of the central arcades and retinal periphery (venous phase). For this study, and consistent with previous ultra-widefield imaging studies in RP and retinopathy, central retinal vessels were defined as those within a circular region centered on the fovea with a radius equal to twice the distance from the optic nerve head to the fovea, while peripheral retinal vessels were classified as those outside this boundary.3,9 Patients with RP demonstrating extensive peripheral atrophy and absent peripheral vasculature were excluded from peripheral angiographic timing analysis but remained included in other analyses, including central retinal vessel timing and descriptive assessment of the entire retina.
In both the transit and nontransit eyes of each study participant, the presence or absence of distinctive angiographic patterns—including peripheral vascular dropout, bone spicule-associated blocking, granular peripheral staining and window defects, late capillary leakage, relative hyperfluorescence or hypofluorescence of the posterior pole, hypofluorescent macular legions, and cystoid macular edema (CME), among others—was recorded for tabulation (Figures 1 and 2).
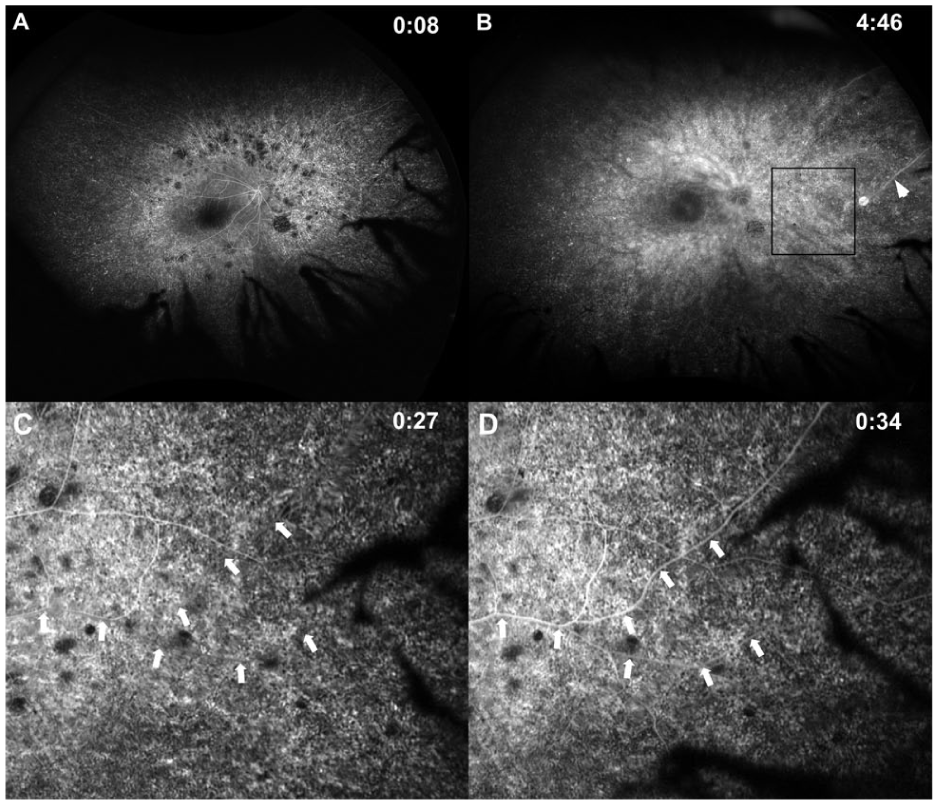
Representative ultra-widefield fluorescein angiogram of a patient with retinitis pigmentosa. (A) Early phase (8 seconds after choroidal flush) shows attenuated retinal vessels, increased visibility of choroidal vessels, diffuse background punctate hyperfluorescence and hypofluorescence, macular hypofluorescence, numerous nummular patches of hypofluorescence, and lack of perfusion of some peripheral veins. (B) Late phase (4 minutes and 46 seconds after choroidal flush) demonstrates filling of peripheral veins with mild leakage from a nasal vein (arrowhead), as well as diffuse capillary leakage in the posterior pole, more prominent along the superior arcade. Persistent macular hypofluorescence and more diffuse background hyperfluorescence are also noted. The black box indicates the regions magnified in panels (C) and (D). (C) Magnified view demonstrating incomplete filling of peripheral nasal veins (arrows) 27 seconds after choroidal flush. (D) The same region at 34 seconds after choroidal flush, now demonstrating complete filling of the peripheral nasal veins (arrows).
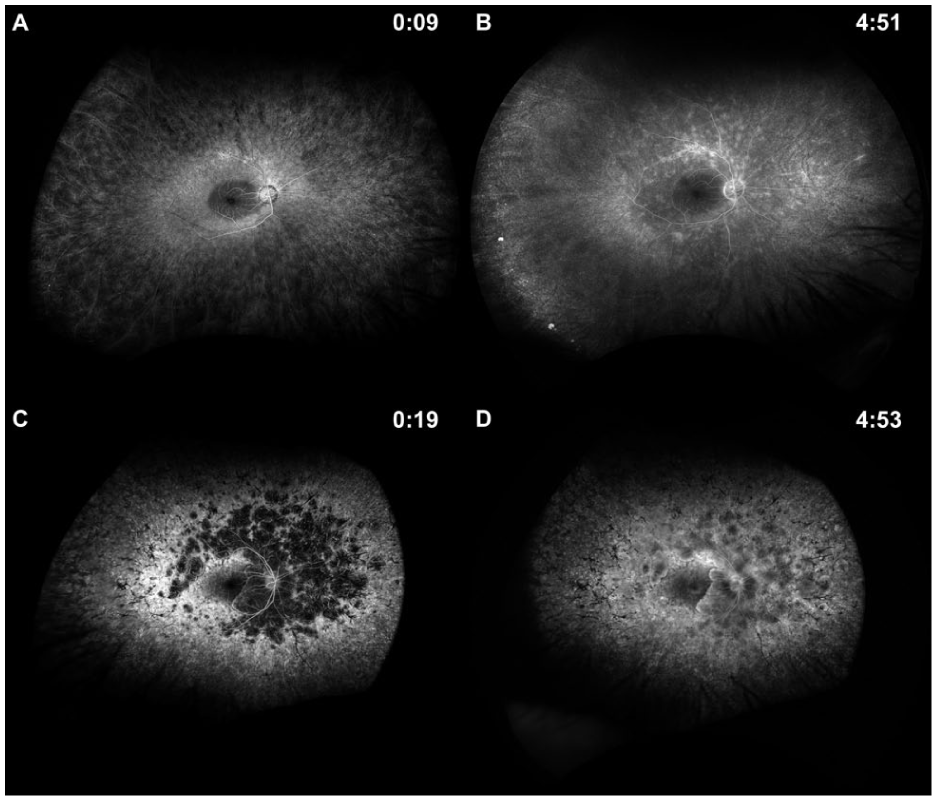
Early- and late-phase ultra-widefield fluorescein angiograms from 2 patients with retinitis pigmentosa demonstrating some common features. (A) Early phase (9 seconds after choroidal flush) demonstrates attenuated retinal vessels, diffuse granular background hyperfluorescence, peripheral capillary dropout, and patchy hypofluorescent blocking corresponding with peripheral pigment clumping. Central macular hypofluorescence is present with surrounding ring-like hyperfluorescence in the posterior pole. (B) Late phase (4 minutes, 51 seconds after choroidal flush) shows increased diffuse background hyperfluorescence with late capillary and large-vessel leakage, more prominent along the vascular arcades, with persistence of central macular hypofluorescence. (C) Early phase (19 seconds after choroidal flush) demonstrates coalescent nummular hypofluorescent window defects with surrounding hyperfluorescent rims present throughout the posterior pole, including the nasal macula. Linear hypofluorescence from pigment clumping is observed along retinal vessels, along with peripheral vascular dropout. (D) Late phase (4 minutes, 53 seconds after choroidal flush) shows that the coalescent nummular hypofluorescent window defects are less distinct, while linear hypofluorescence along vessels and peripheral vascular dropout persist. Additionally, petaloid hyperfluorescence in the macula is indicative of angiographic cystoid macular edema.
Statistical Analysis
Continuous variables were summarized using means and SDs or medians and interquartile ranges, as appropriate, while categorical variables were described using frequencies and percentages. Differences between groups were analyzed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. All statistical analyses were conducted using Stata software (version 17.0; StataCorp), with a P value < .05 considered statistically significant.
Results
A total of 30 eyes from 15 patients with qualifying ultra-widefield imaging were included in the study. The age-matched control group included 28 eyes from 14 participants who underwent ultra-widefield imaging for other indications. The mean age in the RP group was 40.6 ± 16.4 years, while that in the control group was 41.4 ± 12.6 years (P = .88). The RP group included 7 female participants (46.7%) and 8 male participants (53.3%), whereas the control group included 6 male participants (42.8%) and 8 female participants (57.2%) (P = .57). A causative gene was identified in 9 patients with RP, including RHO in 3 and NR2E3 in 2, with single cases of USH2A, EYS, RP1L1, and ABCA4. In total, 5 patients had no documented genetic findings, and 1 had an unclassified variant.
Arteriovenous Transit Times
The mean time to appearance of dye in the central retinal artery was similar between groups (RP: 2.7 ± 1.8 seconds; Control: 2.6 ± 1.7 seconds, P = .91), with comparable medians (RP: 2 [interquartile range (IQR), 2–3] seconds, Control: 2 [IQR, 2–2.8] seconds) (Table 1). Mean time to complete arterial filling of the central arcades was also comparable (RP: 7.1 ± 7.4 seconds; Control: 3.8 ± 1.7 seconds, P = .28), with similar median values (RP: 5 [IQR, 2.5–8.5] seconds, Control: 4 [IQR, 2.3–4.8] seconds). In contrast, the mean duration of the laminar flow arteriovenous phase was significantly prolonged in the RP group (8.1 ± 2.4 seconds; median, 8 [IQR, 7.3–9] seconds) compared with the control group (5.5 ± 1.2 seconds; median, 6 [IQR, 4.3–6] seconds) (P = .001). The mean time to complete venous filling along the central arcades remained similar between the groups (RP: 16.5 ± 4.5 seconds; Control: 15.8 ± 3.3 seconds; P = .70), with similar medians (RP: 16 [IQR, 14–19] seconds, Control: 15.5 [IQR, 13.3–17] seconds).
Comparison of Vascular Transit Times Between Patients with Retinitis Pigmentosa and Age-Matched Controls.
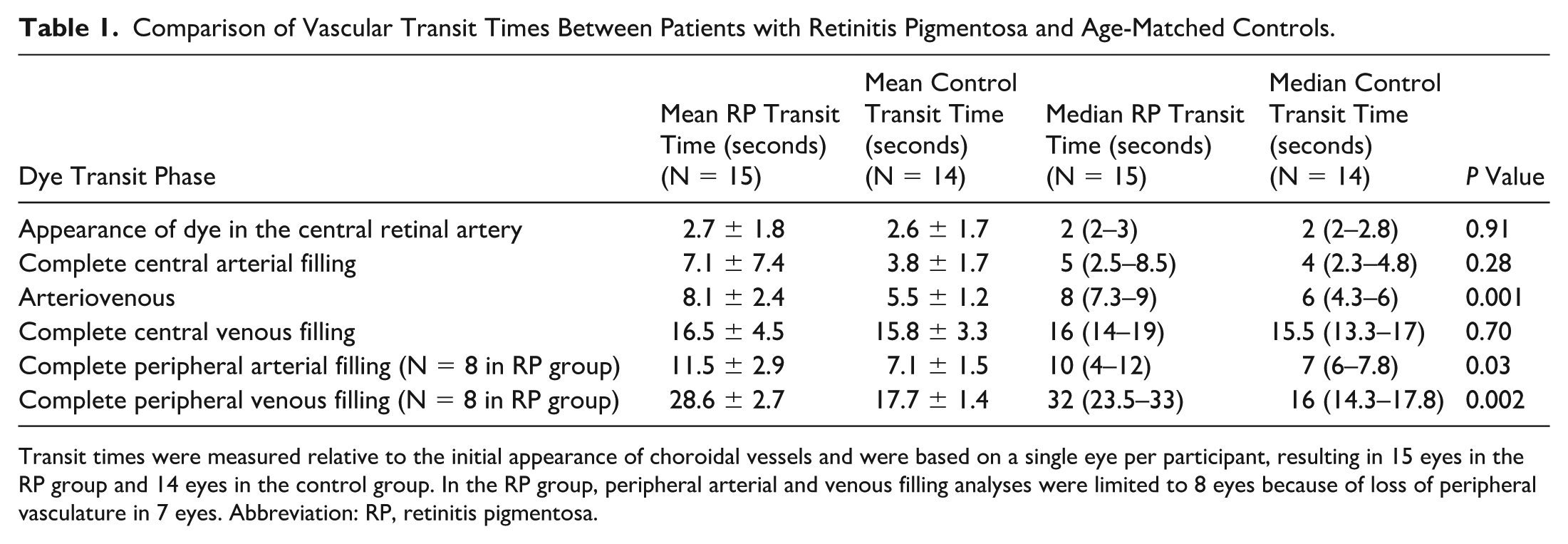
Transit times were measured relative to the initial appearance of choroidal vessels and were based on a single eye per participant, resulting in 15 eyes in the RP group and 14 eyes in the control group. In the RP group, peripheral arterial and venous filling analyses were limited to 8 eyes because of loss of peripheral vasculature in 7 eyes. Abbreviation: RP, retinitis pigmentosa.
In the retinal periphery, mean arterial filling times were significantly longer in the RP group compared with the control group (RP: 11.5 ± 2.9 seconds; Control: 7.1 ± 1.5 seconds; P = .03), with corresponding differences in median values (RP: 10 seconds [IQR, 4–12] vs Control: 7 [IQR, 6–7.8] seconds). Mean peripheral venous filling time was also significantly prolonged in the RP group (28.6 ± 2.7 seconds) compared with the control group (17.7 ± 1.4 seconds) (P = .002), with greater median values (RP: 32 seconds [IQR, 23.5–33] vs Control: 16 seconds [IQR, 14.3–17.8]).
Common Angiographic Features in RP
The most common angiographic features observed in the RP group were peripheral vascular dropout (28/30, 93%), bone spicule-associated peripheral blocking (26/30, 87%), peripheral granular staining and window defects (22/30, 73%), central hypofluorescence (20/30, 67%), and ring-like hyperfluorescence in the posterior pole (16/30, 53%). Ring hyperfluorescence corresponded to the border between intact and degenerating photoreceptors on optical coherence tomography (OCT). Less common findings included hypofluorescent in the posterior pole corresponding to areas of chorioretinal atrophy on fundus autofluorescence (FAF) (6/30, 20%), perivascular linear hypofluorescence (6/30, 20%), baring of choroidal vessels (6/30, 20%), parafoveal window defects (4/30, 13%), and significant peripheral hypofluorescence (1/15, 7%).
Late leakage from central retinal capillaries was observed in 18 of 30 eyes (60%), and late leakage from peripheral retinal capillaries was observed in 16 of 30 eyes (53.3%). Large-vessel leakage was observed in 14 of 30 eyes (46.7%). Angiographic CME was observed in 10 of 30 eyes (33%) on late ultra-widefield FA. An additional 5 eyes demonstrated faint late macular leakage without a distinct petaloid pattern. On same-day OCT, CME was present in 13 of 30 eyes (43%). In total, 6 eyes showed CME on both modalities, 7 eyes had CME detected on OCT without corresponding angiographic CME, and 4 eyes demonstrated angiographic CME without corresponding OCT findings.
Conclusions
Although FA is not routinely used in the diagnosis or management of RP, familiarity with ultra-widefield FA features may aid in the evaluation of atypical cases. In this study, we used ultra-widefield FA to assess both central and peripheral angiographic changes in patients with RP compared with age-matched controls. Our findings demonstrate that while central arcade vascular flow was generally comparable between groups, the laminar arteriovenous phase and peripheral retinal vasculature were significantly impaired in RP, particularly with delayed venous filling.
We recently demonstrated that the number of peripheral retinal vessels in patients with RP is significantly reduced compared with those with normal eyes. 3 Consistent with this finding, we observed a trend toward longer vascular filling times in RP, although most differences were not statistically significant. These findings are largely consistent with prior FA studies of RP, which have reported similar retinal pigment epithelium (RPE)-related changes and vascular abnormalities in the posterior retina. Newsome et al described RPE-level leakage at the macula, optic disc, and peripheral retina in the majority of patients with RP, while Abraham et al and Hyvärinen et al documented delayed dye transit and vascular narrowing in affected retinal quadrants.4,6,10
The delayed venous filling observed in patients with RP may be secondary to diminished overall blood flow in the peripheral retina, likely related to decreased vessel density, which may, in turn, slow the transit of dye to the peripheral veins.11,12 Although intense background fluorescence limited direct visualization of peripheral capillaries in this study, prior OCT angiography studies have consistently demonstrated capillary loss in the central retina.13–16 It is therefore reasonable to infer that similar, or possibly more extensive, capillary loss occurs in the peripheral retina.
In addition to alterations in vascular transit times, ultra-widefield FA revealed characteristic angiographic patterns unique to RP. Peripheral vascular dropout and bone spicule patterns of blocking were observed in most patients. The presence of granular staining and window defects, central hypofluorescence, and ring-like hyperfluorescence within the posterior pole likely reflects a combination of RPE degeneration and photoreceptor loss. The ring-like hyperfluorescence observed in our study corresponded to previously described hyperautofluorescent rings seen on FAF, which delineate the transition zone between healthy and degenerated photoreceptors on OCT. 17 Additionally, late capillary and large-vessel leakage was present in more than 50% of eyes despite the absence of clinical signs of intraocular inflammation. This prevalence exceeds that reported in a prior ultra-widefield FA case series from a tertiary referral center, in which only 1 of 8 patients with RP demonstrated significant leakage, suggesting potential differences in cohort composition, referral patterns, or disease stage and highlighting the need for larger, systematic studies. 18
Several prior reports have suggested that CME in RP may occur without corresponding leakage on FA, including early studies demonstrating angiographic leakage in less than 50% of OCT-confirmed cases.19,20 More recent OCT-based series report CME prevalence ranging from 17% to 59%, likely reflecting variability in detection methods and study populations.21–23 In our cohort, angiographic CME was identified in 33% of eyes, consistent with prior reports. Only 6 of 13 eyes (46%) with OCT-detected CME demonstrated corresponding angiographic CME, and leakage was often subtle on late frames, supporting previous observations that FA may underestimate CME in RP.
Comparison with ultra-widefield FA data from normal eyes supports the reliability of our control cohort. Shah et al reported peripheral arterial filling times of 8.65 ± 2.54 seconds, and She et al observed a range of 3.39 to 8.98 seconds, findings similar to the arterial filling times observed in our control cohort (7.1 ± 1.5 seconds).24,25 Although our controls demonstrated slightly longer venous filling times (17.7 ± 1.4 seconds) than those reported in these studies, the venous phase consistently remained longer than the arterial phase, in agreement with previous findings. These minor differences may be attributable to variations in imaging protocols, operator technique, or differences in participant characteristics, including subclinical ocular or systemic factors. Additionally, definitions of the retinal periphery have varied across studies. In the present study, the peripheral retina was defined using an objective measurement based on the optic nerve head-to-fovea distance, whereas prior studies have relied on qualitative features such as background mottling, peripheral bands of fluorescence, or vascular leakage to define the far periphery.
Several limitations of this study must be acknowledged. Transit times were measured relative to the initial appearance of choroidal vessels; however, in RP, RPE atrophy and window defects may render the choroidal circulation visible earlier and more prominently than in controls, in whom an intact RPE partially masks the choroid. As a result, apparent differences in early transit timing may be influenced by altered choroidal visibility rather than true vascular acceleration. The cross-sectional design precludes assessment of temporal changes in vascular function and their relationship to disease progression. Additionally, our cohort included a relatively small sample of patients with sufficient peripheral vessels for angiographic analysis, which may limit generalizability to advanced stages of RP, where extensive atrophy precludes peripheral evaluation. Interpretation of angiographic images may be complicated by stippled fluorescence and overlap of retinal and choroidal vessels; however, independent grading with adjudication by a retina specialist increases confidence in these assessments. Finally, although ultra-widefield FA provides excellent visualization of mid- and large-caliber vessels, it does not resolve peripheral capillaries. Future integration with widefield OCT angiography may allow more detailed assessment of microvascular loss in RP. 26
In conclusion, this study provides a systematic assessment of peripheral retinal vasculature in RP using ultra-widefield FA. In patients with RP and residual peripheral vessels, venous filling was significantly prolonged. Peripheral vascular attenuation and dropout, linear hypofluorescence, and ring-like hyperfluorescence with central hypofluorescence were the most commonly observed angiographic features of patients with RP. The frequent presence of angiographic leakage in eyes without clinical signs of inflammation further highlights the complexity of vascular involvement in RP. These findings may aid ophthalmologists in the interpretation of fluorescein angiography in RP. Further research is needed to elucidate the longitudinal implications of these vascular alterations and to explore their role in disease monitoring and guiding therapeutic interventions.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of the University of Southern California.
Consent to Participate
Patient data were de-identified before analysis, and the requirement for informed consent was waived.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Ophthalmology of the USC Roski Eye Institute received an unrestricted grant from Research to Prevent Blindness. The funding organization had no role in the design or conduct of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.