
Abstract
Introduction
Antivascular endothelial growth factor (anti-VEGF) agents (eg, bevacizumab, ranibizumab, aflibercept) currently represent the cornerstone of intravitreal treatment for retinal diseases with an exudative component, such as neovascular age-related macular degeneration (AMD), diabetic macular edema (DME), and retinal vein occlusion (RVO). Since their introduction into clinical practice more than a decade ago, these drugs have radically transformed the prognosis of these conditions, which constitute some of the leading causes of irreversible blindness both in working-age adults and in individuals older than age 65 years. 1 Their mechanism of action—based on inhibition of pathologic angiogenesis and reduction of vascular permeability—has been consistently shown to decrease macular edema and improve or stabilize visual acuity in large pivotal clinical trials. 2 Nevertheless, despite their proven efficacy, the main limitation of these agents in clinical practice is the need for repeated intravitreal injections and frequent follow-up visits, which significantly increase the burden on patients, caregivers, and healthcare systems. This factor directly impacts therapeutic adherence and explains why, in real-world settings, functional outcomes are often inferior to those achieved in clinical trials. 3
Faricimab (Vabysmo; Genentech) has emerged as an innovative alternative antiangiogenic treatment, being the first bispecific antibody designed to simultaneously neutralize VEGF-A and angiopoietin-2 (Ang-2). By inhibiting these 2 pathways—the VEGF-dependent angiogenesis and the vascular disruption, inflammation, and permeability promoted by Ang-2—faricimab not only blocks the development of pathologic neovascularization but also promotes vascular stabilization and edema resolution. 4 Unlike conventional anti-VEGF agents such as ranibizumab, aflibercept, or bevacizumab, which in most treatment protocols require monthly administration, phase II and phase III clinical trials, including the AVENUE, STAIRWAY, and TENAYA/LUCERNE trials in patients with neovascular AMD5 –7 and the YOSEMITE/RHINE trial in patients with DME, 8 have demonstrated that faricimab can maintain comparable functional and anatomic outcomes with superior durability. In a significant proportion of patients, injection intervals could be extended to 12 to 16 weeks, thereby reducing visit frequency and treatment burden without compromising efficacy. These findings suggest not only equivalence in efficacy but also potential benefits in terms of treatment burden, patient adherence, and associated direct and indirect costs.
The present study sought to evaluate the efficacy of faricimab in managing clinical and paraclinical parameters (best-corrected visual acuity [BCVA] and central macular thickness [CMT]) after administration of the first dose, even questioning the need for additional loading doses. Confirming this hypothesis could support treatment regimens based on a single dose or schemes with extended intervals between doses and fewer injections, leading to potential benefits, including cost reductions, improved adherence, and fewer risks of adverse effects associated with intravitreal therapy.
Methods
A prospective, observational, longitudinal study was conducted to assess the functional and structural effects of a single dose of intravitreal faricimab in patients requiring antiangiogenic therapy, as indicated by a retina specialist for treatment of diseases such as DME, macular edema secondary to RVO, noninfectious neovascular membranes, or central serous chorioretinopathy. Criteria for inclusion included being older than age 18 years, having an indication for intravitreal faricimab during the recruitment period between January and June 2024, providing informed consent for participation, and being available for follow-up checks. Excluded patients were those who had infectious ocular conditions, had significant concomitant ocular diseases that could contribute to a decrease in visual acuity, had received intravitreal injections within 3 months prior to the beginning of the study, or had undergone intraocular surgery within 6 months prior to the beginning of the study.
For each patient, the BCVA was registered as the functional outcome, and CMT was measured by optical coherence tomography (OCT) as the structural outcome. These outcomes were evaluated prior to the intervention and at follow-up weeks 4, 8, 12, and 16 after the initial injection. Data were included for patients who were considered eligible for continued observation after a single dose of faricimab. To determine whether continuing extension of the first dose should be considered, the criteria applied were whether the patient had a decrease, resolution, or absence of subretinal or intraretinal fluid or had experienced improvement in BCVA compared with the previous visit. If these parameters were not met, patients were required to receive the next loading dose.
An exploratory data analysis was conducted for description of the general sample. A subgroup analysis was conducted in which patients were classified into subgroups of treatment-naive eyes, if it was the first time they had received intravitreal therapy, and treatment-switch eyes, if they had previously been exposed to other antiangiogenic agents. CMT, measured in micrometers, was compared across the study period and between subgroups. For BCVA, data were converted from the Snellen chart to logMAR units. To evaluate differences in BCVA across the study period and between subgroups, changes in BCVA of >0 to 0.3 logMAR were considered mild, >0.3 to 0.6 logMAR were considered moderate, and >0.6 logMAR were considered significant.
To evaluate statistically significant differences, Student t tests were performed. P values less than .05 were considered significant. Statistical analysis was conducted using Real Statistics software (version 9.6.1 for Excel, September 2025).
Results
Forty-nine eyes of 41 patients were included, of which 28 were treatment-naive eyes, having never been previously exposed to antiangiogenics, and 21 were eyes of patients for whom a switch from their previous antiangiogenic regimen had been indicated due to little or no response. Mean age of participants was 61.5 years (range, 29–88 years). The diagnosis for which antiangiogenic therapy had been indicated was DME in 63.3% of cases (31 eyes), AMD in its wet form in 24.5% (12 eyes), RVO in 10.2% (5 eyes), and central serous chorioretinopathy in 2.0% (1 eye). Time from initial diagnosis in the treatment-switch group was a mean 7.4 years (range, 3–15 years). The majority of patients in the treatment-switch group had previously been treated with aflibercept, receiving a mean of 3.2 previous applications (range, 2–7 doses).
Structural and functional outcomes after patients received a single dose of intravitreal faricimab were evaluated at weeks 4, 8, 12, and 16 after injection. In clinical follow-up, during which BCVA data were collected, it was necessary to exclude 10 eyes during the study period, with a final sample of 39 eyes by week 16, considering that these patients had an indication for additional loading doses as worsening of CMT occurred in 3 eyes and only partial improvement occurred in 7 eyes. A second injection was necessary in 9 of these cases and a third injection was necessary in 1 case during the follow-up period. Furthermore, for CMT analysis, 11 additional eyes were lost to follow-up, as patients continued to attend clinical follow-up visits but did not attend the assigned OCT follow-up appointments, and therefore complete data were not obtained. Thus, the final sample by week 16 was 28 eyes.
For structural analysis, changes in CMT were evaluated. At the 4-week follow-up, a mean CMT reduction from 370.0 µm to 252.5 µm was observed, representing a difference of 117.5 µm from baseline. This reduction was maintained at weeks 8, 12, and 16, with decreases of 118.0 µm, 98.5 µm, and 101.4 µm from baseline, respectively. These changes in CMT reached statistical significance in all cases.
In the subgroup analysis, it was found that the treatment-naive group, who were being treated with antiangiogenics for the first time, had an initial CMT reduction from a mean 367.9 µm to 248.2 µm at 4 weeks, representing a mean difference of 119.7 µm. Again, this reduction was maintained during follow-up, with mean differential values of 129.5 µm at 8 weeks, 117.7 µm at 12 weeks, and 135.0 µm at 16 weeks from baseline. Similar to the general sample, mean changes from baseline in CMT in the treatment-naive group all reached statistical significance.
For the treatment-switch group, whose patients had a history of intravitreal therapy, CMT decreased from a mean 372.8 µm initially to 258.2 µm at 4 weeks, representing a mean reduction from baseline of 114.6 µm. This difference in CMT lasted until week 8, with a mean reduction of 103.8 µm, but these changes were not sustained by weeks 12 and 16, with mean differential values of 70.3 µm and 48.2 µm, respectively. Decreases in CMT were statistically significant in the treatment-switch group at weeks 4 and 8, but not at weeks 12 and 16. Reductions in CMT in both the general sample and the subgroups are presented in Table 1.
Changes in CMT in Patients Treated With a Single Dose of Intravitreal Faricimab, in Total and by Treatment Subgroup.
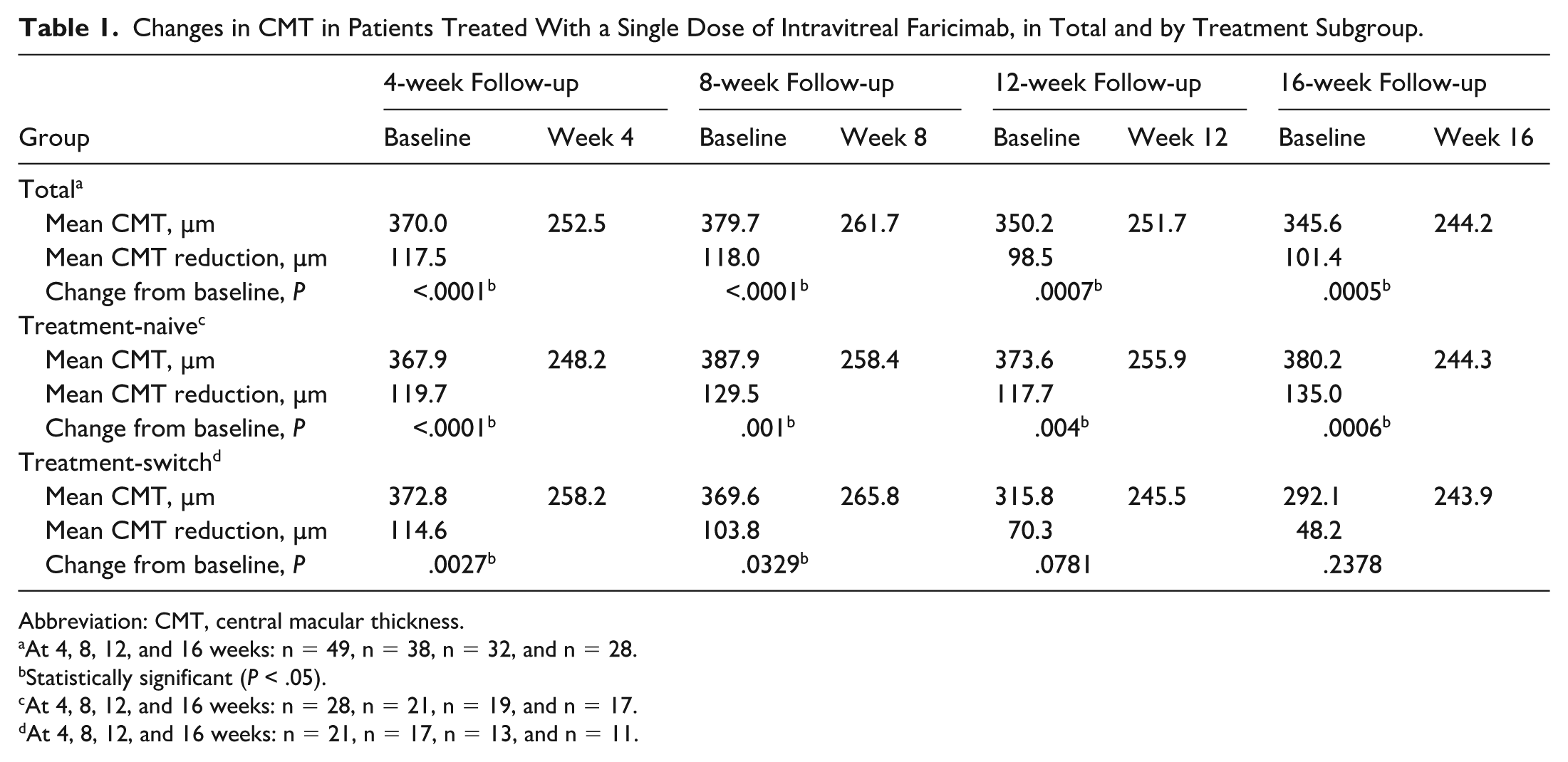
Abbreviation: CMT, central macular thickness.
At 4, 8, 12, and 16 weeks: n = 49, n = 38, n = 32, and n = 28.
Statistically significant (P < .05).
At 4, 8, 12, and 16 weeks: n = 28, n = 21, n = 19, and n = 17.
At 4, 8, 12, and 16 weeks: n = 21, n = 17, n = 13, and n = 11.
In order to avoid possible biases originating from the noticeable drop in total sample size for structural analysis, baseline CMT was compared between patients who completed all 16 weeks (completer group; n = 28) and those who did not (dropout group; n = 21). The mean baseline CMT was 345.6 µm for the completer group and 402.6 µm for the dropout group. It was to be expected that the mean CMT would be somewhat higher in the dropout group because the 10 eyes that required further doses of antiangiogenic treatment (as worsening or only partial improvement of CMT was observed) were included, but even with this consideration, the differences did not reach statistical significance (P = .148). Therefore, it could be concluded that the anatomic characteristics at baseline were similar between the 2 groups, and even more so, that the final 28 eyes included for structural analysis by week 16 were representative of the starting cohort.
The main diagnoses indicating antiangiogenic treatment in the initial sample were DME and AMD. Considering that these 2 diseases may behave differently in terms of inflammatory load and anti-VEGF response, a separate analysis was conducted to assess the anatomic response to treatment for each diagnosis. For patients with a diagnosis of DME, the mean CMT reduction at 4 weeks was 84.2 µm. The CMT showed fluctuations at weeks 8, 12, and 16, with mean decreases from baseline of 66.0 µm, 77.1 µm, and 80.5 µm, respectively. Although the differences in CMT from baseline were smaller than that observed in the overall sample, the mean differential values reached statistical significance at all time points except week 8.
In subgroup analyses among patients with DME, treatment-naive patients demonstrated a greater reduction in CMT compared with the treatment-switch group, with an initial mean CMT reduction of 85.3 µm by week 4, and mean reductions of 83.1 µm, 93.8 µm, and 98.1 µm at weeks 8, 12, and 16, respectively. Again, these changes in CMT reached statistical significance at all time points except week 8.
For the treatment-switch group of patients with DME, an initial mean decrease in CMT of 82.4 µm from baseline was observed at 4 weeks, but then the mean CMT dropped by 43.8 µm, 46.3 µm, and 48.8 µm at 8, 12, and 16 weeks, respectively. None of the changes reached statistical significance.
For patients with AMD, the mean reduction in CMT from baseline was 92.2 µm by week 4, 117.8 µm by week 8, 81.4 µm by week 12, and 61.7 µm by week 16. Changes in CMT reached statistical significance at all time points except week 16.
In subgroup analyses among patients with AMD, treatment-naive patients showed even greater reductions in CMT, with a mean difference from baseline of 121.2 µm by week 4, 130.3 µm by week 8, 107.2 µm by week 12, and 90.3 µm by week 16. The CMT reductions at weeks 4 and 8 reached statistical significance.
For the treatment-switch group of patients with AMD, the reduction in CMT was less favorable, with mean differences from baseline of 63.2 µm, 99.0 µm, 50.6 µm, and 27.4 µm at weeks 4, 8, 12, and 16, respectively. None of these reductions reached statistical significance. Table 2 summarizes the reductions in CMT by diagnosis and subgroup.
Changes in CMT in Patients Treated With a Single Dose of Intravitreal Faricimab, by Diagnosis and Treatment Subgroup.
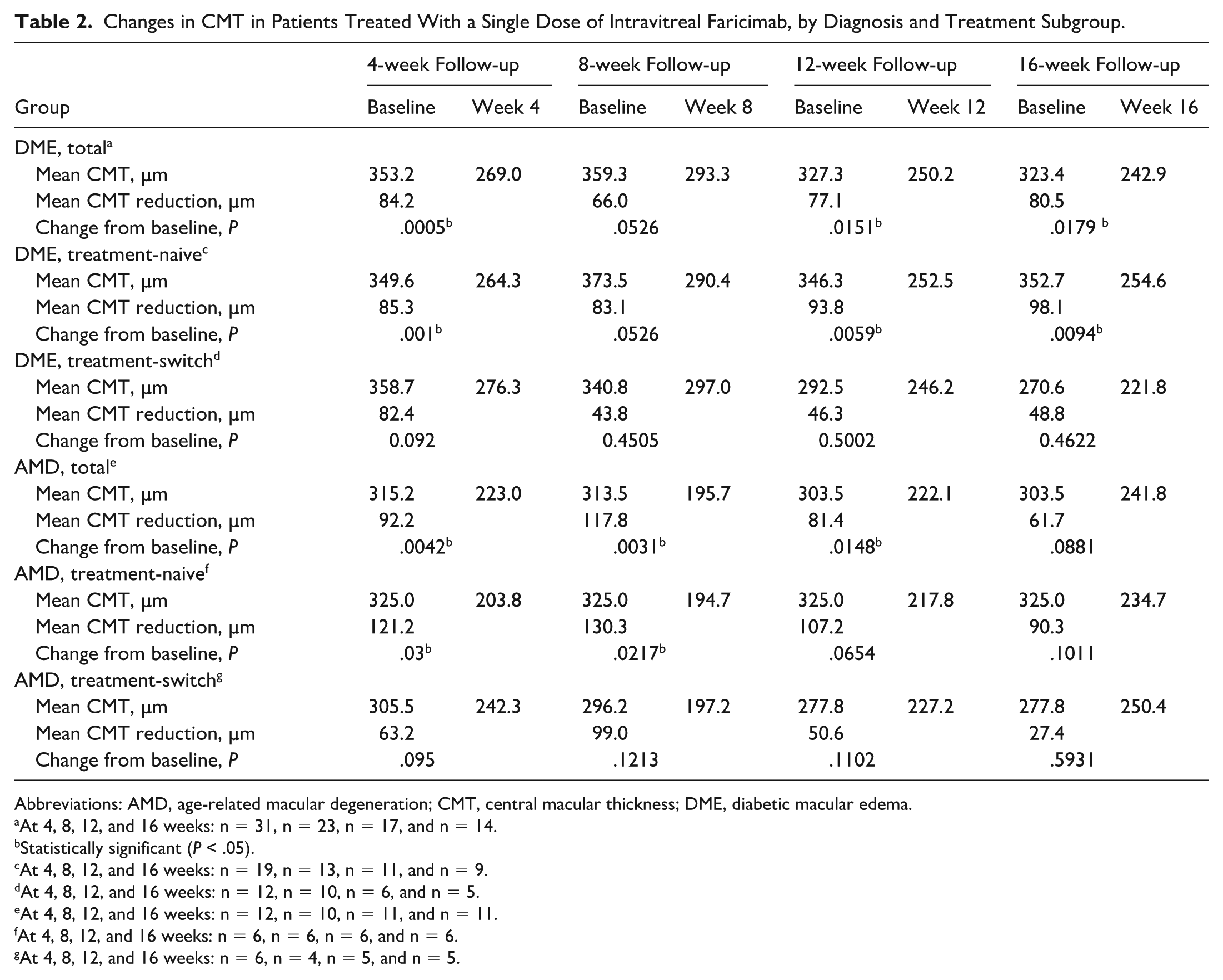
Abbreviations: AMD, age-related macular degeneration; CMT, central macular thickness; DME, diabetic macular edema.
At 4, 8, 12, and 16 weeks: n = 31, n = 23, n = 17, and n = 14.
Statistically significant (P < .05).
At 4, 8, 12, and 16 weeks: n = 19, n = 13, n = 11, and n = 9.
At 4, 8, 12, and 16 weeks: n = 12, n = 10, n = 6, and n = 5.
At 4, 8, 12, and 16 weeks: n = 12, n = 10, n = 11, and n = 11.
At 4, 8, 12, and 16 weeks: n = 6, n = 6, n = 6, and n = 6.
At 4, 8, 12, and 16 weeks: n = 6, n = 4, n = 5, and n = 5.
For functional analysis, changes in BCVA were assessed. In the general sample, the mean BCVA was 0.61 logMAR (equivalent to 20/80 on the Snellen chart), improving to a mean 0.49 logMAR (Snellen equivalent 20/60) at 4 weeks, and remaining at this level at weeks 8, 12, and 16. It was found that 36.7% of eyes did not have any changes in vision, while 53.1% presented some degree of visual improvement and 10.2% had some degree of visual deterioration at the 4-week follow-up. By weeks 8, 12, and 16, visual improvement was maintained in 54.4%, 61.0%, and 56.4% of eyes, respectively. In contrast, BCVA remained unchanged in 34.8%, 26.8%, and 28.2% of eyes by weeks 8, 12, and 16, respectively, while some decrease in BCVA occurred in 10.8%, 12.2%, and 15.4% of eyes, respectively. None of these values reached statistical significance.
Patients in the treatment-naive group presented with a mean BCVA of 0.49 logMAR (Snellen equivalent 20/60), which initially improved to a mean 0.37 logMAR (Snellen equivalent 20/50) at 4 weeks and then improved to a mean 0.33 logMAR (Snellen equivalent 20/40) at 8 weeks. In the treatment-naive group, the percentage of patients who experienced some degree of BCVA improvement was 53.6%, 59.2%, 69.5%, and 63.6% at 4, 8, 12, and 16 weeks, respectively. However, despite more patients in the treatment-naive group showing vision improvement compared with the general cohort, statistical significance was not achieved during the study period.
The treatment-switch subgroup had a somewhat worse BCVA at baseline, at a mean 0.77 logMAR (Snellen equivalent 20/125), which improved to a mean 0.65 logMAR (Snellen equivalent 20/80) at 4 weeks and then dropped to 0.67 logMAR (Snellen equivalent 20/100) at 8 weeks, followed by stabilization of BCVA (mean, 0.64 [Snellen equivalent 20/80]) at week 12 and 0.66 at week 16. Percentages of eyes with vision improvement were also lower than that observed in the general sample, with 52.4% at 4 weeks, 47.3% at 8 weeks, 50.0% at 12 weeks and 47.0% at 16 weeks showing improvement, although none of the changes were statistically significant. Changes in BCVA for the general sample and the subgroups are shown in Table 3.
Changes in BCVA Following a Single Dose of Intravitreal Faricimab, in Total and by Treatment Subgroup.
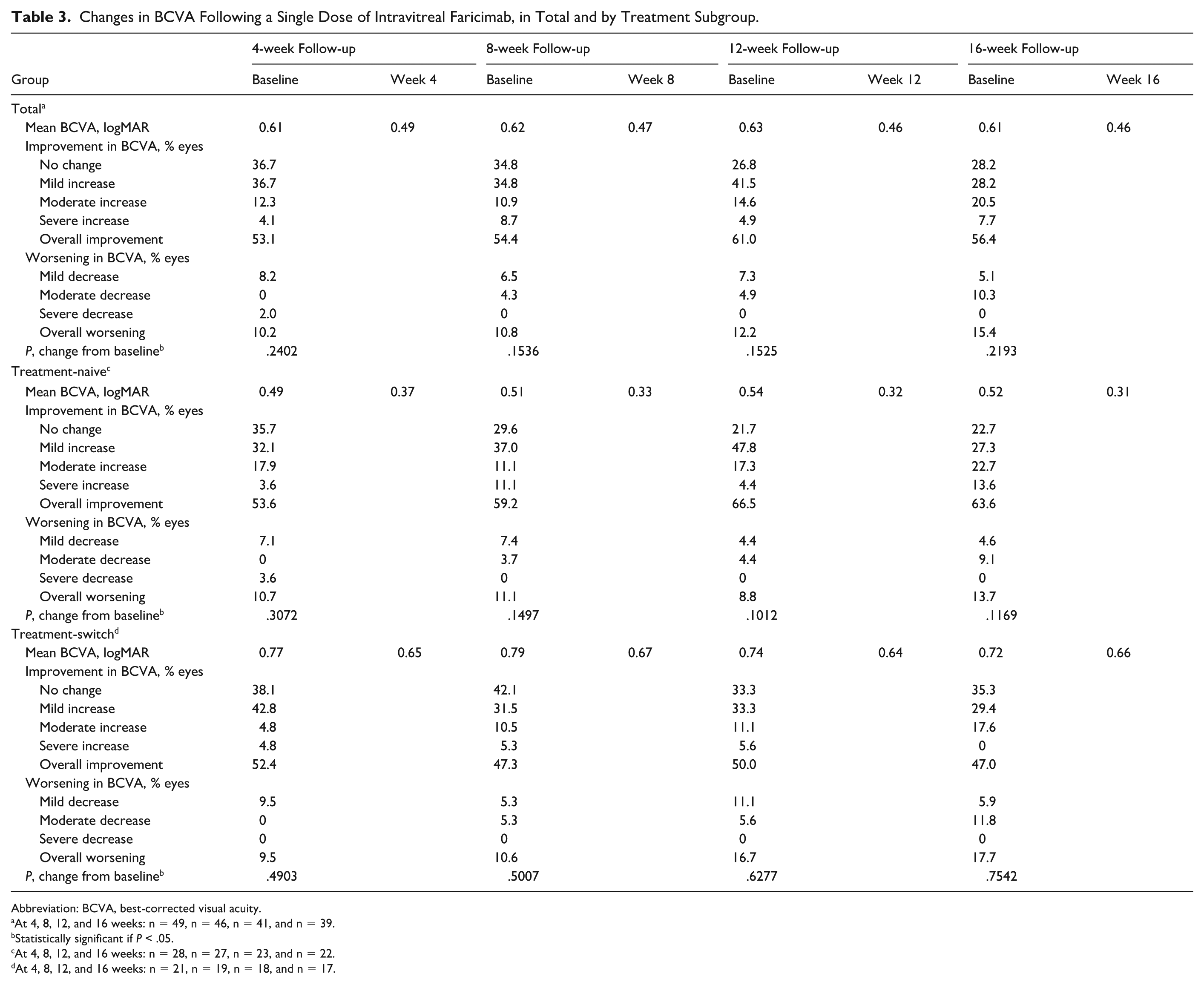
Abbreviation: BCVA, best-corrected visual acuity.
At 4, 8, 12, and 16 weeks: n = 49, n = 46, n = 41, and n = 39.
Statistically significant if P < .05.
At 4, 8, 12, and 16 weeks: n = 28, n = 27, n = 23, and n = 22.
At 4, 8, 12, and 16 weeks: n = 21, n = 19, n = 18, and n = 17.
Conclusions
In the present cohort, the reduction in CMT after a single intravitreal dose of faricimab was the most relevant finding, with a mean decrease of 117.5 µm at 4 weeks, which remained stable in subsequent measurements at 8, 12, and 16 weeks, all with statistical significance. This pattern of early and sustained response aligns with the evidence from pivotal faricimab trials, which have documented rapid and long-lasting anatomic reductions in macular thickness in various exudative retinal diseases. In the AVENUE and STAIRWAY studies, conducted in patients with neovascular AMD, a rapid resolution of intraretinal and subretinal fluid was observed, with marked decreases in macular thickness after the initial doses and maintained anatomic stability even with extended treatment intervals of up to 12 and 16 weeks.5,6 Similarly, in the YOSEMITE and RHINE trials for treatment of DME, mean reductions in CMT ranged between 150 µm and 250 µm during the first year, with sustained stability under personalized dosing regimens. 8
Although our results were from a small sample and short follow-up period, they confirm a significant reduction in CMT from the very first injection, suggesting an early anatomic effect of faricimab even after a single administration. This finding is consistent with real-world cohorts that have reported the phenomenon of “first-dose dryness,” meaning near-complete resolution of macular fluid and a marked reduction in edema after the first faricimab application. 4 This phenomenon reflects the potency of dual VEGF-A and Ang-2 inhibition, which promotes more effective closure of endothelial junctions and stabilizes the blood–retinal barrier.
The magnitude of anatomic reduction observed in our population is comparable to that reported in the TENAYA and LUCERNE trials, where faricimab demonstrated efficacy and durability similar to that observed for aflibercept, with the possibility of extending injections to every 16 weeks. 7 This is clinically relevant, as the need for multiple loading doses and frequent visits is one of the main limitations of conventional anti-VEGF therapies. Nevertheless, in our study, 10 eyes (20.4%) required additional doses of antiangiogenic therapy during follow-up, mainly due to persistent or recurrent macular edema. This would suggest that a considerable proportion of patients may indeed require loading doses in order to maintain adequate anatomic control. Treatment regimens should therefore be individualized based on patient needs.
Furthermore, 11 eyes were lost to OCT imaging follow-up, which, in addition to the 10 eyes that required further treatment, represents a loss of 42.8% of the initial cohort. While it is plausible that patients with good anatomic responses were less likely to require or seek imaging, it is also very probable that, conversely, the nonresponders decided to withdraw from the study. This last scenario introduces an important risk of survivorship bias of the best responders, forcing us to view the results less optimistically and to interpret them carefully.
While loading-dose regimens were not formally evaluated in the present study, our findings suggest that a mandatory loading phase may not be universally required to achieve short-term anatomic benefit in all patients. This contrasts with the design of pivotal clinical trials and most previously reported cohorts, in which loading doses were systematically administered as part of standardized treatment protocols. In our real-world cohort, a substantial proportion of eyes demonstrated early and sustained anatomic improvement after a single faricimab injection, supporting the concept of an individualized treatment approach rather than a fixed loading strategy. Importantly, this anatomic benefit did not consistently translate into statistically significant visual improvement, underscoring that anatomic drying alone should not be interpreted as a surrogate for functional success. This dissociation between structure and function is well recognized in chronic retinal disease and highlights the need for cautious interpretation when considering reduced initial dosing strategies. Given the limited sample size and follow-up duration, these findings should be regarded as exploratory and warrant confirmation in larger prospective studies with longer follow-up to better define which patient subgroups may safely benefit from a reduced initial treatment burden.
The subgroup analysis showed a differential response depending on prior treatment status. In treatment-naive patients, the reduction in CMT was consistent and statistically significant at all follow-up time points, with decreases in CMT averaging between 119.7 µm and 135.0 µm, suggesting a marked and sustained anatomic response. In contrast, treatment-switch patients previously treated with aflibercept showed an initially favorable response (mean reduction in CMT of 114.6 µm at 4 weeks and 103.8 µm at 8 weeks), but these changes did not maintain statistical significance at weeks 12 and 16. This pattern matches reports in the published literature, where treatment-naive patients tended to show better anatomic and functional responses as compared with previously treated patients. Indeed, pivotal faricimab trials predominantly included treatment-naive individuals, while real-world studies in treatment-switch populations have documented more modest and shorter-lasting anatomic improvements, likely associated with structural retinal damage, fibrosis, or irreversible vascular changes due to chronic disease.7,8
Regarding functional outcomes, all groups demonstrated mild clinical improvement in BCVA after the first faricimab injection, but none of the changes reached statistical significance in temporal comparisons. In the overall sample, the mean BCVA improved from 0.61 logMAR to 0.49 logMAR at 4 weeks (mean difference, −0.12 logMAR), with the mean BCVA remaining near the 4-week value at 8 to 16 weeks (mean difference, −0.15 to −0.17 logMAR). However, despite being clinically noticeable, these gains in BCVA cannot be considered statistically significant, because at all time points, the P value was >.05, and therefore, from a statistical point of view, these visual changes were not distinguishable from baseline.
The magnitude of visual improvement observed falls within the expected range described in the literature for faricimab and other anti-VEGF agents. Pivotal trials and published analyses for faricimab (phase II/III) and other anti-VEGF therapies typically report mean gains in visual acuity of ~1 to 3 Early Treatment Diabetic Retinopathy Study lines (equivalent to a mean reduction of ~0.1–0.3 logMAR) in the first months of follow-up, with variations depending on population (treatment-naive vs chronic), target disease (neovascular AMD vs DME), and dosing regimen. Therefore, our findings are clinically consistent with previous reports, despite not reaching statistical significance.5 –8
Results of the subgroup analyses were consistent with those previously reported. Treatment-naive patients presented better baseline BCVA (mean, 0.49 logMAR; Snellen equivalent 20/60), which improved to a mean 0.37 logMAR at 4 weeks and 0.33 logMAR at 8 weeks (mean difference, −0.12 to −0.18 logMAR). Although a considerable proportion of patients experienced some degree of visual improvement (53.6% at 4 weeks, up to 63.6% at 16 weeks), changes did not reach statistical significance (P = .10–.31). The treatment-switch group, despite starting with a worse baseline BCVA (mean, 0.77 logMAR; Snellen equivalent 20/125), also showed a notable initial response (mean change in BCVA in the first month, −0.12 logMAR), but the improvement was less sustained, and improvement rates were slightly lower at intermediate time points. These findings align with previous publications showing that although anatomic improvement with faricimab may be rapid, the translation into visual gain is more modest and more variable, particularly in previously treated populations, due to structural and chronic factors.5 –8
This difference in functional outcomes between groups should be interpreted cautiously. The better baseline visual acuity in the treatment-naive group may give the false impression of a more favorable response; however, this initial difference also introduces a ceiling effect, reflecting a greater functional visual reserve. This makes direct comparison of changes between groups challenging, considering that treatment-switch patients, previously exposed to other anti-VEGF agents, often present chronic retinal structural alterations such as photoreceptor atrophy, fibrosis, or irreversible vascular changes that limit the potential for visual recovery even when clear anatomic improvement is achieved. Therefore, the smaller visual gain observed in the treatment-switch group is likely related more to previous retinal damage than to reduced pharmacologic efficacy of faricimab. OCT biomarkers associated with a poorer response to antiangiogenic therapy have been described previously. In patients with DME, the presence of hyperreflective retinal foci, a disrupted ellipsoid zone or external limiting membrane, hyperreflective choroidal foci, and disorganization of retinal inner layers have been associated with worse visual acuity outcomes at 12 months of treatment. 9 In patients with AMD, the presence of pigment epithelial detachment, geographic atrophy, and both intraretinal fluid and subretinal fluid have been described as the main 3 biomarkers predicting reduced visual acuity despite treatment. 10 In this study, no formal analysis of OCT biomarkers was performed. Nevertheless, we recognize the importance of identifying OCT biomarkers to establish the patient’s prognosis and as a guide to define the interval of treatment extension.
From a health economics perspective, intravitreal anti-VEGF therapy represents a substantial financial burden for both patients and healthcare systems, particularly in chronic retinal diseases that require repeated injections over prolonged periods. Published economic evaluations consistently identify drug-acquisition costs and injection frequency as the principal drivers of overall treatment expense. Recent comparative cost and budget-impact analyses have shown that the per-injection acquisition cost of anti-VEGF agents ranges approximately USD$1,700 to $1,900 for aflibercept, USD$1,900 to $2,100 for ranibizumab, and USD$2,100 to $2,300 for faricimab, depending on the healthcare system and pricing framework. Importantly, when treatment durability and injection frequency are incorporated into economic models, therapies allowing fewer injections per year—such as faricimab—demonstrate a lower or comparable annual per-patient cost despite a higher unit price, largely due to reduced injection frequency and associated procedure-related costs. 11
In this context, a treatment strategy in which a subset of patients achieves sustained anatomic stability after a single initial faricimab injection could further amplify these economic advantages. Compared with standard loading regimens requiring 3 to 4 monthly injections, a single-dose approach would theoretically reduce direct drug-acquisition costs during the initial treatment phase, in addition to lowering indirect costs related to clinic visits, imaging, transportation, caregiver involvement, and productivity loss. Although formal cost-effectiveness analyses specifically evaluating a single-dose faricimab strategy are currently lacking, our findings provide preliminary real-world evidence supporting the biologic plausibility of a reduced injection burden in selected patients, which may translate into meaningful economic and accessibility benefits when applied within an individualized treatment framework.
For further research, we suggest that multicenter clinical trials be designed with inclusion of larger populations and longer follow-up periods (of at least 12 months), standardized OCT grading protocols, and prospective biomarker-based subgroup analyses to evaluating OCT biomarkers associated with a poorer treatment response and better identify candidates who would benefit from extended treatment in order to compare single-dose vs loading-dose treatment approaches. We also suggest conducting studies to develop short- and long-term budget impact models, ideally for various anti-VEGF agents, in order to objectively assess the economic benefits that longer treatment durations, as those achieved with faricimab, could bring.
In summary, in this real-world cohort, a single intravitreal injection of faricimab was associated with a clinically and statistically significant reduction in CMT that was evident as early as 4 weeks and remained stable throughout the 16-week follow-up period. This anatomic response was particularly pronounced in treatment-naive eyes, supporting the concept that patients receiving anti-VEGF therapy for the first time may have greater structural reserve and a higher potential for early anatomic recovery. Importantly, ~58% of eyes for which complete follow-up data were available demonstrated sustained anatomic improvement on OCT without requiring additional antiangiogenic treatment during the observation period.
However, the observed anatomic benefit did not consistently translate into statistically significant improvements in BCVA. Although mild and clinically perceptible visual gains were observed in a proportion of patients, none of the temporal comparisons reached statistical significance. This dissociation between anatomic and functional outcomes has been widely described in chronic retinal diseases and likely reflects the influence of irreversible factors such as photoreceptor loss, ischemia, fibrosis, and chronic vascular damage, which may limit visual recovery despite effective reduction of macular edema. Consequently, anatomic drying alone should not be interpreted as a surrogate for functional success, and visual outcomes must remain a central consideration when evaluating treatment strategies.
Notably, more than 20% of eyes required additional antiangiogenic injections during follow-up due to incomplete or recurrent anatomic response, underscoring that a single-dose strategy is not universally effective. These findings indicate that while a subset of patients may achieve short-term anatomic stability after a single faricimab injection, a substantial proportion still requires additional treatment to maintain adequate disease control. As such, loading doses remain necessary for many patients, particularly those with chronic disease, prior treatment exposure, or suboptimal early response.
Taken together, these results suggest that mandatory monthly loading doses may not be required for all patients to achieve short-term anatomic benefit, but they should not be omitted indiscriminately. Rather, our findings support an individualized treatment approach guided by early anatomic response, close functional monitoring, and disease-specific characteristics. In this context, the observed 31.7% reduction in CMT at 4 weeks suggests that early anatomic response thresholds—such as a ~30% reduction in CMT—could potentially serve as pragmatic markers to help identify patients who may benefit from continued treatment extension vs those who may require conventional loading regimens.
From a real-world perspective, these findings are clinically relevant, particularly in settings where access to intravitreal therapy is limited by economic, geographic, or healthcare system constraints. Nevertheless, any potential reduction in treatment burden must be carefully balanced against the risk of undertreatment, especially given the absence of statistically significant visual gains and the notable proportion of patients requiring additional injections.
The present study is limited by its relatively small sample size, short follow-up duration, and attrition related to the need for rescue therapy, which may have influenced functional outcomes and limited subgroup analyses. Therefore, these results should be interpreted as exploratory rather than as practice-changing. Larger prospective studies with longer follow-up, incorporation of additional structural biomarkers, and direct comparisons with standard loading regimens are required to better define which patient subgroups may safely benefit from reduced initial dosing strategies.
In conclusion, while faricimab demonstrates a robust and early anatomic effect after a single injection in a substantial proportion of patients, this response is not universal and does not consistently translate into significant visual improvement. These findings reinforce the need for personalized treatment strategies rather than fixed dosing paradigms and highlight the importance of cautious interpretation when considering deviations from established loading protocols.
Footnotes
Acknowledgements
The authors would like to acknowledge all staff at Fundación + Luz for making the development of this project possible.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethics Committee in accordance with the Declaration of Helsinki of 1975, as revised in 2000, and local regulations.
Consent to Participate
Informed consent for participation was obtained from each participant, and confidentiality in the processing of sensitive personal data was guaranteed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request, seeking to safeguard confidentiality of the participants’ sensitive personal data.