
Abstract
Purpose:
To report the clinical and microbiological characteristics of 5 cases of postsurgical endophthalmitis caused by Ralstonia mannitolilytica and to review the relevant literature.
Methods:
Medical records of patients diagnosed with endophthalmitis due to Ralstonia mannitolilytica were retrospectively reviewed. The organism was identified using an automated VITEK system, while antibiotic susceptibility testing was conducted using standard microbiologic protocols. Primary outcome measures included infection control, visual improvement at 4 to 6 weeks of follow-up, and the antibiotic sensitivity profile of Ralstonia.
Results:
Infection control was achieved in all cases. Visual outcomes were excellent in 3 out of 5 cases. All isolates demonstrated in vitro susceptibility to ciprofloxacin but differential sensitivity to ceftazidime.
Conclusions:
To our knowledge, this is the first reported case series of culture-proven R. mannitolilytica endophthalmitis. This series highlights the importance of accurate identification and antibiotic susceptibility-tailored management in infections caused by rare organisms such as Ralstonia.
Introduction
Postoperative endophthalmitis is one of the most dreaded complications following ocular surgery worldwide. With advances in sterilization techniques and the implementation of strict aseptic measures, the incidence of endophthalmitis has decreased from as high as 2% from the 1920s to the 1940s to 0.03% in recent years.1,2 Postoperative endophthalmitis is predominantly caused by gram-positive bacteria, followed by gram-negative bacteria and fungi. 3
Members of the genus Ralstonia are aerobic gram-negative bacteria that have emerged as opportunistic nosocomial pathogens. This genus comprises 3 species of relevance in humans: Ralstonia (R.) insidiosa, R. mannitolilytica, and R. pickettii. Ralstonia species can cause infections ranging from asymptomatic colonization to fatal septicemia.4–15 Ralstonia are prolific biofilm formers, which makes them highly virulent and resistant to empirical antibiotics.5,16 Endophthalmitis caused by Ralstonia species is rare, with only 1 previously reported case series describing endophthalmitis caused by R. pickettii. 17
We report 5 cases of postoperative endophthalmitis caused by R. mannitolilytica over 4 years at a tertiary eye care center, suggesting that this organism may be more prevalent and virulent than previously recognized.
Methods
This retrospective observational case series included 5 culture-proven cases of postoperative endophthalmitis caused by Ralstonia species. While reviewing the microbiological data from cases of postoperative endophthalmitis in a tertiary eye center since 2016, Ralstonia species were identified in isolates obtained between 2022 and 2025. In all these cases, intraocular specimens were examined using Gram staining for bacteria and potassium hydroxide/calcofluor white mount for fungi. Specimens were cultured on blood agar, chocolate agar, brain–heart infusion broth, and Sabouraud dextrose agar. The cultures grew gram-negative bacilli within 24 to 48 hours that were identified as R. mannitolilytica using the VITEK 2 automated identification and antimicrobial susceptibility testing system (bioMérieux), which demonstrated excellent identification ability. Antibiotic susceptibility testing for Ralstonia species included amikacin, cefotaxime, ciprofloxacin, moxifloxacin, gentamicin, piperacillin–tazobactam, ceftazidime, colistin, and tobramycin. The results were interpreted according to the Clinical and Laboratory Standards Institute criteria established for Pseudomonas aeruginosa ATCC 27853, as Clinical and Laboratory Standards Institute susceptibility breakpoints for Ralstonia species are currently unavailable.
The decision to perform intravitreal (IVT) antibiotic injection or pars plana vitrectomy (PPV) was based on clinical judgment and did not necessarily adhere to the Endophthalmitis Vitrectomy Study protocol. Eyes with early infection and minimal vitritis received IVT antibiotics, whereas eyes with severe infections characterized by dense anterior chamber and vitreous exudates underwent primary vitrectomy. Cases showing a poor response to initial IVT therapy were subsequently managed with vitrectomy. The frequency of repeat IVT injections and changes in antibiotic treatment were determined by the treating clinician based on the clinical response and antibiotic sensitivity. The 5 cases were managed by 4 clinicians, with 1 clinician managing 2 cases. Infection control was defined clinically as resolution of hypopyon and vitreous exudates, along with restoration of fundus visibility up to the third-order retinal vessels on serial follow-up examinations.
Medical records of these patients were reviewed for information regarding the preoperative, intraoperative, and postoperative course, with a follow-up duration of at least 4 weeks. Institutional review board approval was obtained for the study. The study adhered to the tenets of the Declaration of Helsinki.
Case 1
A 35-year-old man underwent uneventful phacoemulsification with capsular tension ring and posterior chamber intraocular lens implantation for a posttraumatic subluxated cataract in the left eye. On postoperative day (POD) 1, mild corneal edema with a hazy fundus view was noted, and ultrasonography demonstrated moderate vitreous echoes; therefore, the patient was closely monitored. By POD 2, visual acuity (VA) had worsened to hand movements (HM), accompanied by increased vitreous echoes (Figure 1A). An anterior chamber tap with IVT vancomycin, ceftazidime, and dexamethasone was performed. Gram-negative bacilli were identified on smear examination, and vitrectomy with repeat IVT vancomycin, ceftazidime, and dexamethasone was performed the next day due to poor clinical response.
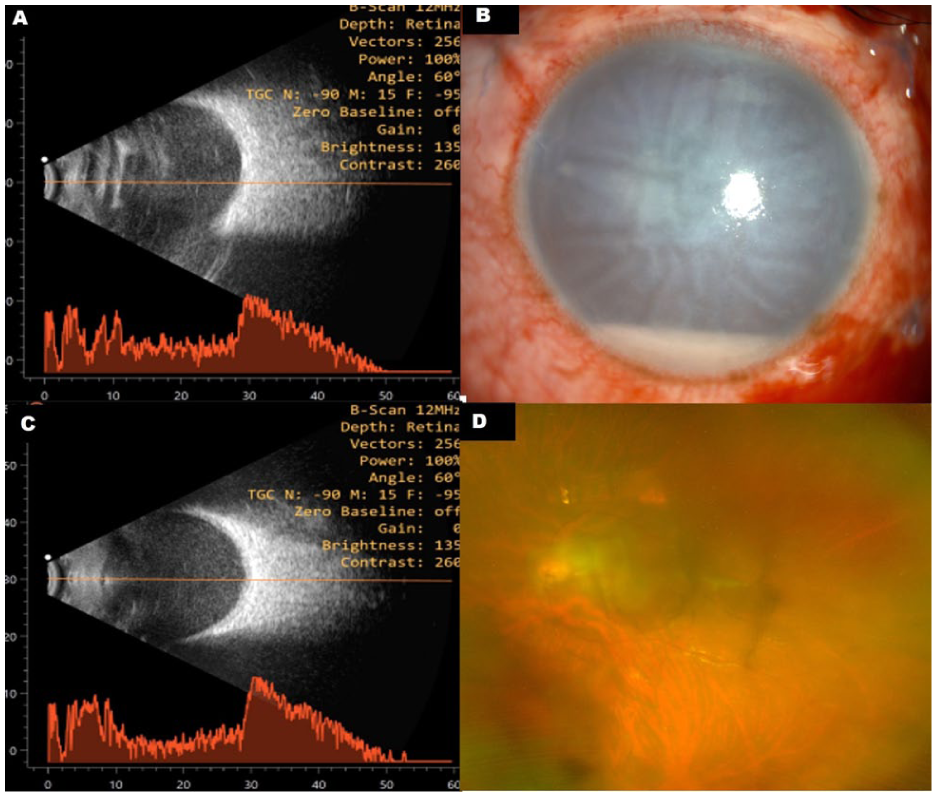
Clinical images of Case 1. (A) Baseline B-scan ultrasonography demonstrating dense vitreous echoes at presentation. (B) Slitlamp image obtained on post-vitrectomy day 3 showing worsening hypopyon and corneal edema despite vitrectomy and repeat intravitreal injections of vancomycin, ceftazidime, and dexamethasone. (C) Corresponding B-scan ultrasonography demonstrating worsening vitreous echoes. The patient subsequently responded to 2 intravitreal injections each of ciprofloxacin and piperacillin–tazobactam. (D) Ultra-widefield fundus image at 6 weeks showing resolution of infection with improved fundus visibility.
On post-vitrectomy day 2, worsening corneal edema, hypopyon (Figure 1B), and increased vitreous echoes on ultrasonography (Figure 1C) were observed. Culture grew R. mannitolilytica, which demonstrated resistance to most antibiotics, including ceftazidime, but sensitivity to ciprofloxacin and piperacillin–tazobactam. The R. mannitolilytica isolate in this case, as well as isolates from all other cases in this series, were resistant to vancomycin, as expected for most gram-negative bacteria. IVT and intravenous ciprofloxacin produced limited improvement, following which IVT piperacillin–tazobactam (225 µg/0.1 mL) was administered. Infection was controlled after 2 injections. At 6 weeks, best-corrected visual acuity (BCVA) improved to 6/45, with an attached retina, stable intraocular lens, foveal thinning, and minimal residual corneal haze (Figure 1D).
Case 2
A 69-year-old woman underwent uneventful phacoemulsification with intraocular lens implantation in the left eye. On POD 1, the eye was quiet. However, on POD 4, she presented with complaints of diminished vision associated with pain. Examination revealed a fibrinous reaction and hypopyon in the anterior chamber, vision restricted to HM, and numerous vitreous echoes in ultrasonography, with an attached retina. The patient underwent PPV with IVT vancomycin, ceftazidime, and dexamethasone administered at the end of surgery. On POD 2 following vitrectomy, repeat IVT injections of vancomycin, ceftazidime, and dexamethasone were administered, and the patient was started on oral corticosteroids.
On POD 4, R. mannitolilytica was isolated from the culture, which was resistant to ceftazidime but sensitive to ciprofloxacin. Accordingly, treatment was switched to IVT ciprofloxacin and dexamethasone. After 3 alternate-day IVT injections of ciprofloxacin and dexamethasone, the infection was controlled. At 1-month follow-up, BCVA improved to 6/9.
Case 3
A 53-year-old man with a history of diabetes mellitus and hypertension presented with vitreous hemorrhage and tractional retinal detachment in the right eye. VA in the affected eye was counting fingers close to the face. He underwent IVT antivascular endothelial growth factor injection followed by phacoemulsification, intraocular lens implantation, PPV, and endolaser photocoagulation in the right eye. On POD 1, the patient was comfortable, with clear ocular media and an attached retina. However, on POD 4, he presented with pain and eyelid swelling. Examination revealed chemosis, conjunctival congestion, and a fibrinous reaction in the anterior chamber with hypopyon. VA had deteriorated to perception of light. Ultrasonography demonstrated multiple low-reflective dot and membranous vitreous echoes.
The patient underwent vitreous lavage with IVT vancomycin, ceftazidime, and dexamethasone. R mannitolilytica was isolated from the culture, which was sensitive to most antibiotics, including ceftazidime. Intraoperatively, retinal detachment with areas of retinal necrosis was noted, and silicone oil tamponade was performed. The infection was controlled after 6 IVT injections of vancomycin, ceftazidime, and dexamethasone, and the eye was successfully salvaged. However, the retina remained necrotic and detached, and the final VA was limited to perception of light.
Case 4
A 68-year-old man who had undergone uneventful phacoemulsification with intraocular implantation in the left eye presented on POD 15 with pain, redness, and diminished vision (Figure 2A). On examination, BCVA was 2/60. Slitlamp examination revealed hypopyon, and fundus examination showed vitreous exudates with hazy visualization of the optic disc and first-order retinal vessels (Figure 2B). Ultrasonography demonstrated a moderate number of vitreous echoes with an attached retina (Figure 2C). An anterior chamber tap was performed, followed by IVT administration of vancomycin, ceftazidime, and dexamethasone. The patient showed symptomatic improvement, with a reduction in anterior chamber inflammation and gradual resolution of vitreous exudates. Culture from the anterior chamber tap grew R. mannitolilytica that was sensitive to ciprofloxacin and showed intermediate sensitivity to ceftazidime.
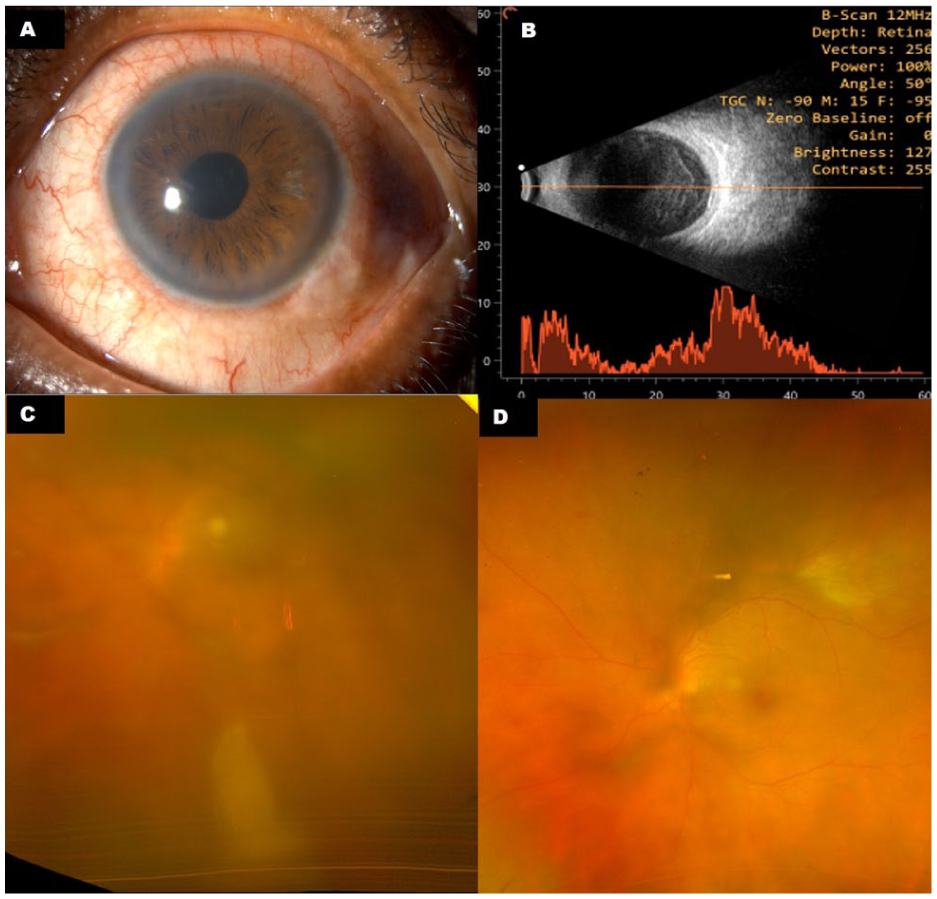
Clinical images of Case 4. (A) Slitlamp image at presentation showing ciliary congestion, mild corneal haze, and moderate anterior chamber reaction without hypopyon. (B) B-scan ultrasonography demonstrating dense vitreous echoes with an attached retina. (C) Pseudocolor fundus image at presentation showing dense vitreous exudates with hazy fundus visualization. (D) Pseudocolor fundus image obtained 15 days after treatment demonstrating reduction of vitreous exudates and improved media clarity after a single intravitreal injection of vancomycin, ceftazidime, and dexamethasone.
Despite the unfavorable in vitro susceptibility profile, the patient responded well to a single IVT injection of vancomycin, ceftazidime, and dexamethasone. Treatment was subsequently switched to oral ciprofloxacin along with oral corticosteroids, and the patient was monitored closely. He showed gradual improvement (Figure 2D), and the BCVA improved to 6/6 at the 1-month follow-up.
Case 5
A 79-year-old woman underwent uneventful phacoemulsification combined with trabeculectomy in the left eye. The intraoperative period and POD 1 examination were unremarkable. However, on POD 5, she presented with hypopyon and a hazy fundus view, and BCVA had deteriorated to HM. The filtering bleb appeared clear. Ultrasonography demonstrated numerous low-reflective dot and membranous vitreous echoes with an attached retina.
The patient was started on intravenous cefotaxime 1 g twice daily and underwent PPV with IVT vancomycin, ceftazidime, and dexamethasone administered at the end of surgery. On post-vitrectomy day 2, repeat IVT injections of vancomycin, ceftazidime, and dexamethasone were administered. On POD 4, R. mannitolilytica was isolated from culture that was resistant to amikacin; sensitive to cefotaxime, tobramycin, and ciprofloxacin; and demonstrated intermediate sensitivity to ceftazidime. Due to a suboptimal clinical response to ceftazidime, treatment was switched to IVT ciprofloxacin and dexamethasone. After 3 IVT injections of ciprofloxacin and dexamethasone on alternate days, the infection was controlled. At the 1-month follow-up visit, VA in the left eye had improved to 6/18, and intraocular pressure was adequately controlled with antiglaucoma medications.
The clinical presentation, microbiological characteristics, treatment details, and outcomes of the 5 cases of postoperative endophthalmitis caused by R. mannitolilytica are summarized in Table 1.
Summary of Clinical, Microbiological, and Treatment Characteristics of Patients Diagnosed With Ralstonia mannitolilytica Endophthalmitis.
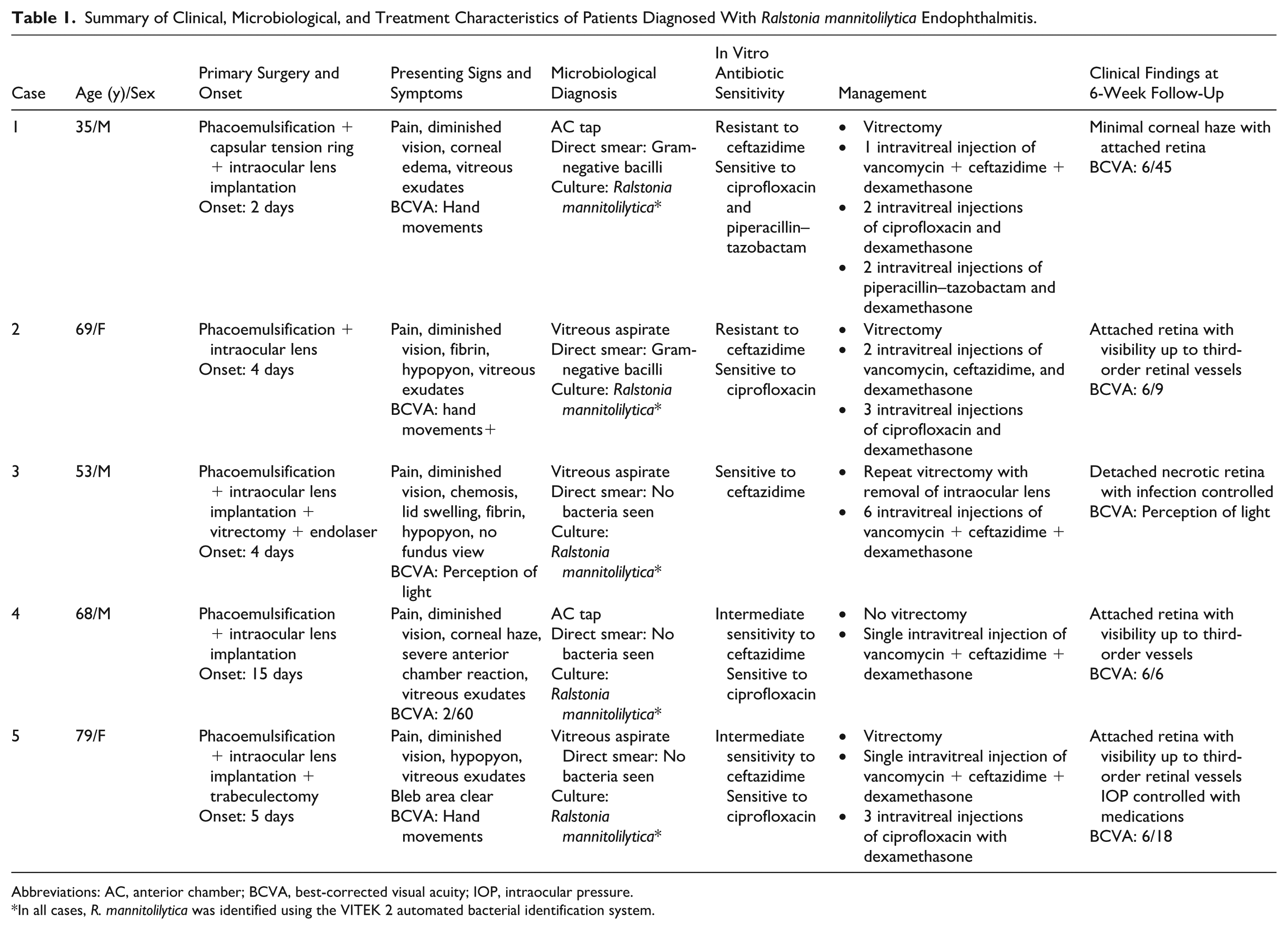
Abbreviations: AC, anterior chamber; BCVA, best-corrected visual acuity; IOP, intraocular pressure.
In all cases, R. mannitolilytica was identified using the VITEK 2 automated bacterial identification system.
Conclusions
Ralstonia species are emerging global opportunistic pathogens that affect immunocompromised hosts and have been documented to cause bloodstream and device-related nosocomial infections. 5 These organisms are aerobic, gram-negative, oxidase-positive, nonfermentative rods that are widely distributed in our surrounding habitats, such as water, including hospital water supplies, soil, and plants. 5 Their ability to pass through 0.2 µm filters increases the risk of contamination of medical products and solutions, thus causing nosocomial infections associated with medical devices, hospital equipment, water, and contaminated parenteral solutions.9–11 Ralstonia infections have been reported in conditions such as meningitis, peritonitis, osteomyelitis, catheter-related bacteremia, hemodialysis units, neonatal intensive care units, and transplant recipients. Infections have also been described in patients with risk factors including chemotherapy, mechanical ventilation, corticosteroid use, and diabetes mellitus.12–15 Biofilm formation contributes to virulence, environmental persistence, and antibiotic resistance.5,16
To date, there have been no documented reports of R. mannitolilytica causing endophthalmitis or other ocular infections. A related species, R. pickettii, has previously been reported to cause endophthalmitis following IVT methotrexate injection, which was linked to contaminated vials. 17
Water contamination is considered a major source of Ralstonia outbreaks, including those associated with contaminated saline solutions and multidose flushes.18–21 Despite extensive review of surgical protocols, consumables, and operative practices in our cases, the source of infection could not be identified, highlighting the need for vigilant monitoring of intraoperative fluids, hospital water systems, and manufacturer compliance. 20 In addition, all possible environmental sources, such as water purifiers, reservoirs, and autoclave systems, were thoroughly investigated for microbial contamination; however, no source could be identified.
Ralstonia infections are likely underreported as a result of misidentification with routine biochemical tests. Species identification is particularly challenging, as R. mannitolilytica shares several biochemical characteristics with R. pickettii. In the present series, R. mannitolilytica was identified using the VITEK 2 system, which includes specific tests that can differentiate these 2 species (Figure 3). VITEK 2 is an automatic system designed for the identification and antimicrobial susceptibility testing of clinically important bacteria, including gram-negative rods.22,23 Other advanced techniques used for identification of Ralstonia species include matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and 16S ribosomal RNA gene sequencing.12,15
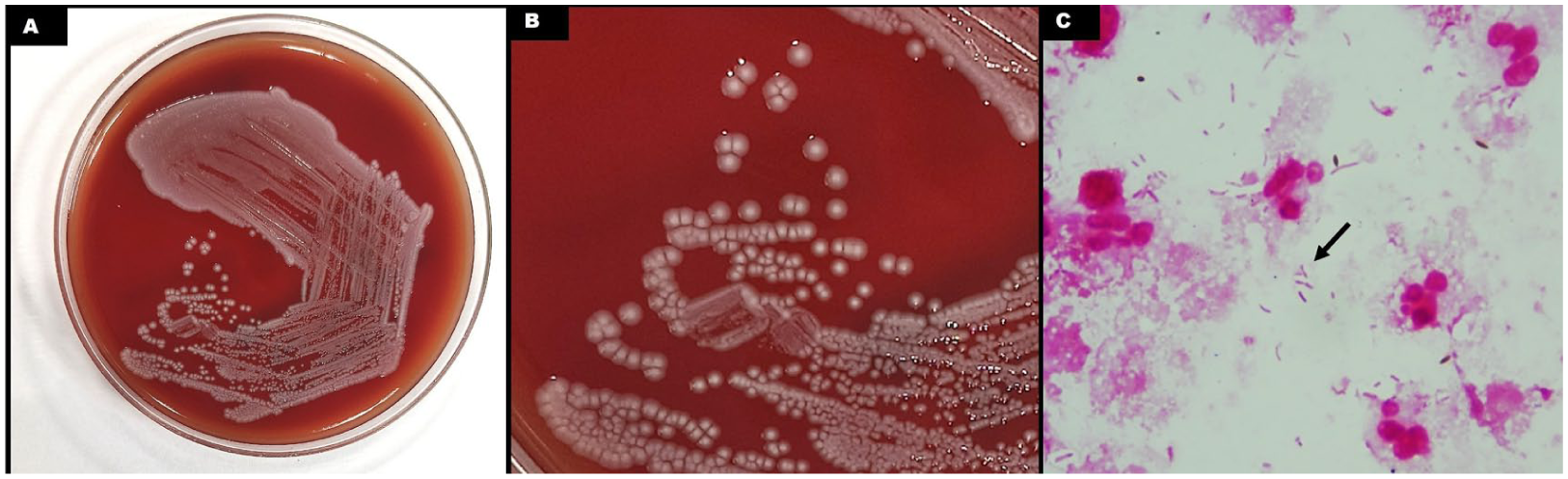
Microbiological images of Ralstonia mannitolilytica isolated from patients in the present study. (A) Growth of gram-negative bacilli identified as R. mannitolilytica on blood agar culture from the vitreous aspirate of a patient. (B) Magnified view of the colonies isolated from another patient demonstrating gray, moist, and translucent non-hemolytic colonies approximately 2 mm in diameter with round morphology and entire margins. (C) Gram stain of vitreous aspirate showing multiple slender gram-negative bacilli (black arrow), along with polymorphonuclear leukocytes and a few uveal pigments.
There are currently no established treatment guidelines or Clinical and Laboratory Standards Institute susceptibility breakpoints for Ralstonia species. Consequently, antibiotic susceptibility results are interpreted by comparison with standard Pseudomonas aeruginosa strains. Antibiotic susceptibility patterns are variable, with frequent resistance to aminoglycosides, ceftazidime, and carbapenems, mediated by multiple β-lactamase and carbapenemase genes.15,24–28 In the present series, isolates demonstrated variable sensitivity to ceftazidime, necessitating the use of alternative IVT antibiotics such as ciprofloxacin and piperacillin–tazobactam. Given that ceftazidime remains the first-line empirical antibiotic for endophthalmitis, awareness of the resistance patterns associated with Ralstonia species is crucial.
The management of R. mannitolilytica endophthalmitis is particularly challenging because of variable resistance to multiple antibiotics, including aminoglycosides, amoxicillin–clavulanic acid, cephalosporins, colistin, and carbapenems, as well as the limited availability of antibiotics suitable for intravitreal administration. The poor penetration of intravenous antibiotics further complicates treatment.
Basso et al reported a case of persisting and relapsing bacteremia caused by concurrent infection with R. pickettii and R. mannitolilytica. 26 Species-level identification is therefore important, as 2 species of the same genus may exhibit different antibiotic susceptibility patterns. 26
Although most systemic antibiotics show poor vitreous penetration, ciprofloxacin, which was commonly used in this series, achieves relatively higher intraocular concentrations and has previously been explored as systemic prophylaxis for postoperative endophthalmitis. 29 Human pharmacokinetic studies have demonstrated vitreous concentrations of approximately 0.5 to 0.64 µg/mL, which may exceed the minimum inhibitory concentration for some gram-negative and coagulase-negative staphylococcal organisms, although not for Staphylococcus aureus or Pseudomonas aeruginosa.30,31 In addition, ocular inflammation or trauma may further enhance intraocular penetration by disrupting the blood–retinal barrier. 32 However, these concentrations remain significantly lower than those achieved with IVT therapy. Therefore, systemic ciprofloxacin should be considered an adjunctive rather than primary treatment modality in the management of endophthalmitis. 29
The major limitation of this study is its small sample size. Further studies involving larger cohorts may provide better insights into the clinical profile of ocular Ralstonia infections, including their antibiotic susceptibility patterns and optimal treatment strategies.
In conclusion, this series highlights key considerations in postoperative endophthalmitis caused by the emerging pathogen R. mannitolilytica. Persistent infection despite standard IVT therapy should raise suspicion for atypical organisms such as Ralstonia, which can be accurately identified using advanced diagnostic platforms such as the VITEK system.
The variable susceptibility to ceftazidime observed in this series underscores the importance of early culture-directed therapy, acknowledging possible discrepancies between in vitro susceptibility profiles and in vivo clinical response. Ciprofloxacin showed consistent susceptibility across isolates and may serve as a useful adjunct when resistance to standard therapy is suspected. Furthermore, given the environmental resilience of Ralstonia species, identification of this organism should prompt careful surveillance for potential environmental sources of infection.
Footnotes
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from the patients before performing the procedures.
Consent for Publication
Written informed consent was obtained from the patients for the publication of all photographs and images included in the case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.