
Abstract
Purpose:
To evaluate the use of Densiron Xtra tamponade for inferior and complicated rhegmatogenous retinal detachments (RRD).
Methods:
A retrospective case series was conducted between January 2019 and December 2023. Cases involving ocular trauma or follow-up of less than 12 months were excluded.
Results:
The median patient age was 66 years, and 39.5% of the patients were female. All 123 eyes had inferior RRDs; 42.3% had a history of prior retinal detachment, 85.4% had proliferative vitreoretinopathy grade C/D, and 67.5% had macula-off retinal detachments. The mean tamponade duration was 10.4 weeks, and the mean follow-up duration was 16.3 months. Primary and final anatomic success rates were 75.6% and 96.8%, respectively, with a mean logMAR improvement in visual acuity of 0.4 (P < .001). Complications before oil removal included anterior chamber dispersion (11.4%) and retinal breaks (4.1%). After oil removal, complications included anterior chamber dispersion requiring washout (15.5%), cataract formation (13.8%), posterior capsular opacification (15.5%), hypotony (8.1%), intraocular inflammation (4%), temporary macular thinning (4%), and emulsification (2%).
Conclusions:
Densiron Xtra tamponade demonstrated excellent anatomic and visual outcomes in eyes with inferior and complicated RRDs, with low complication rates.
Keywords
Introduction
Heavy silicone oils are denser than water and consist of a mixture of silicone oil and partially fluorinated alkanes. Densiron 68 (Fluoron GmbH), hereafter referred to as high-viscosity heavy silicone oil, has been used to treat rhegmatogenous retinal detachments (RRD) with or without proliferative vitreoretinopathy (PVR), giant retinal tears, and macular holes.1–13 It is composed of 69.5% 5000 millipascal-second polydimethylsiloxane and 30.5% partially fluorinated 3.5 millipascal-second perfluorohexyloctane, resulting in a viscosity of 1400 centistokes. This formulation provides effective tamponade of the inferior retina and posterior pole. High-viscosity heavy silicone oil has demonstrated favorable anatomic and functional outcomes in complex and recurrent retinal detachments.14–20
Densiron Xtra (Labtician Ophthalmics), hereafter referred to as low-viscosity heavy silicone oil, is a newer-generation heavy silicone oil formulation. It consists of 69.5% polydimethylsiloxane, of which 90% is 1000 millipascal-second silicone oil and 10% is very-high-molecular-weight polydimethylsiloxane (432 kDa). The remaining 30.5% is composed of perfluorohexyloctane, a semifluorinated alkane with low viscosity that acts as a thinning agent, resulting in an overall viscosity of 1200 centistokes. The long polymer chains of the very-high-molecular-weight polydimethylsiloxane increase chain entanglement, thereby enhancing structural integrity and resistance to oil stretching and droplet formation. Together, these properties provide a balance between lower viscosity for improved surgical handling and enhanced resistance to emulsification while maintaining effective tamponade of inferior retinal pathologies.21–23
To date, few studies have examined the outcomes of low-viscosity heavy silicone oil. Existing case series are limited by small sample sizes and include relatively few retinal detachments complicated by PVR,16,24 making it difficult to assess the effectiveness of this tamponade in complex cases. Therefore, we evaluated the outcomes of RRD treated with low-viscosity heavy silicone oil tamponade in a cohort in which most cases were complicated by PVR.
Methods
Study Design and Participants
This single-center retrospective case series was approved by the Wayne State University Institutional Review Board. All patients were treated at Windsor Eye Associates (ON, Canada) under a reliance agreement. Patients aged 18 years or older with RRD who underwent surgery with low-viscosity heavy silicone oil tamponade between January 2019 and November 2023, with follow-up through November 2024, were included. Exclusion criteria included aphakia, ocular trauma, choroidal hemorrhage, and a follow-up of less than 12 months.
Data Collection
Demographic, clinical, and surgical characteristics are described in Tables 1 and 2. PVR grade was defined according to the Retinal Society classification system. 25 Hypotony was defined as an intraocular pressure of less than 5 mm Hg, 26 and elevated intraocular pressure was defined as greater than 21 mm Hg. Temporary macular thinning was identified on optical coherence tomography imaging by 2 independent reviewers (PY and VR) as disruption or loss of retinal layers within the fovea. The primary surgical success rate was defined as retinal attachment for at least 3 months after initial removal of low-viscosity heavy silicone oil without additional retinal surgeries. Final success rate was defined as reattachment of the retina maintained for at least 12 months after the final heavy silicone oil removal. Time to redetachment was defined as the duration (in months) between low-viscosity heavy silicone oil placement or removal and subsequent retinal detachment. Best-corrected visual acuity was determined using the Snellen visual acuity (VA) chart and converted to logMAR values. LogMAR equivalents for counting fingers, hand motion, light perception, and no light perception were assigned values of 1.85, 2.3, 2.7, and 3.0, respectively, based on values established in the literature.27,28
Baseline and Preoperative Characteristics.
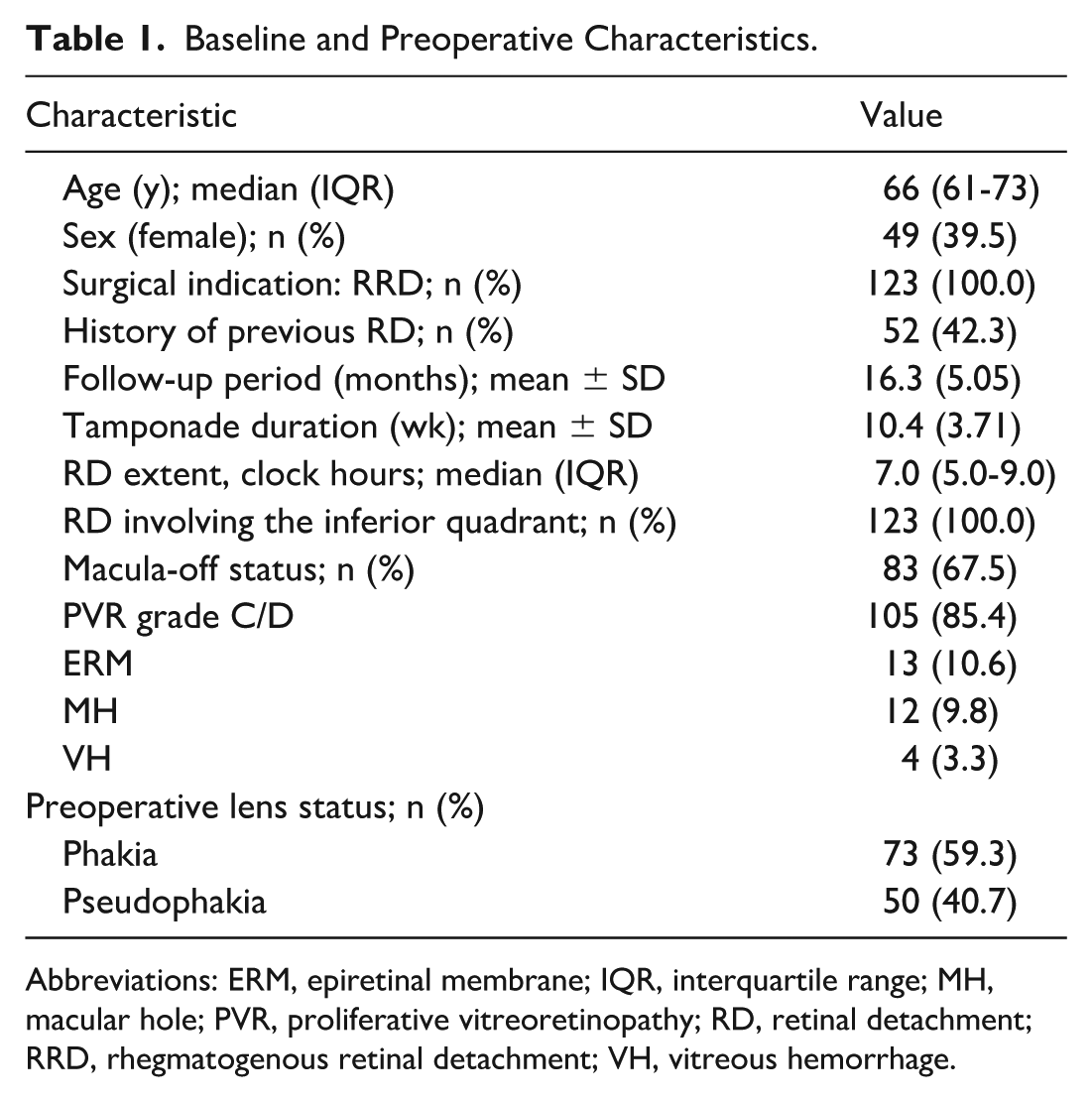
Abbreviations: ERM, epiretinal membrane; IQR, interquartile range; MH, macular hole; PVR, proliferative vitreoretinopathy; RD, retinal detachment; RRD, rhegmatogenous retinal detachment; VH, vitreous hemorrhage.
Postoperative Outcomes and Complications.
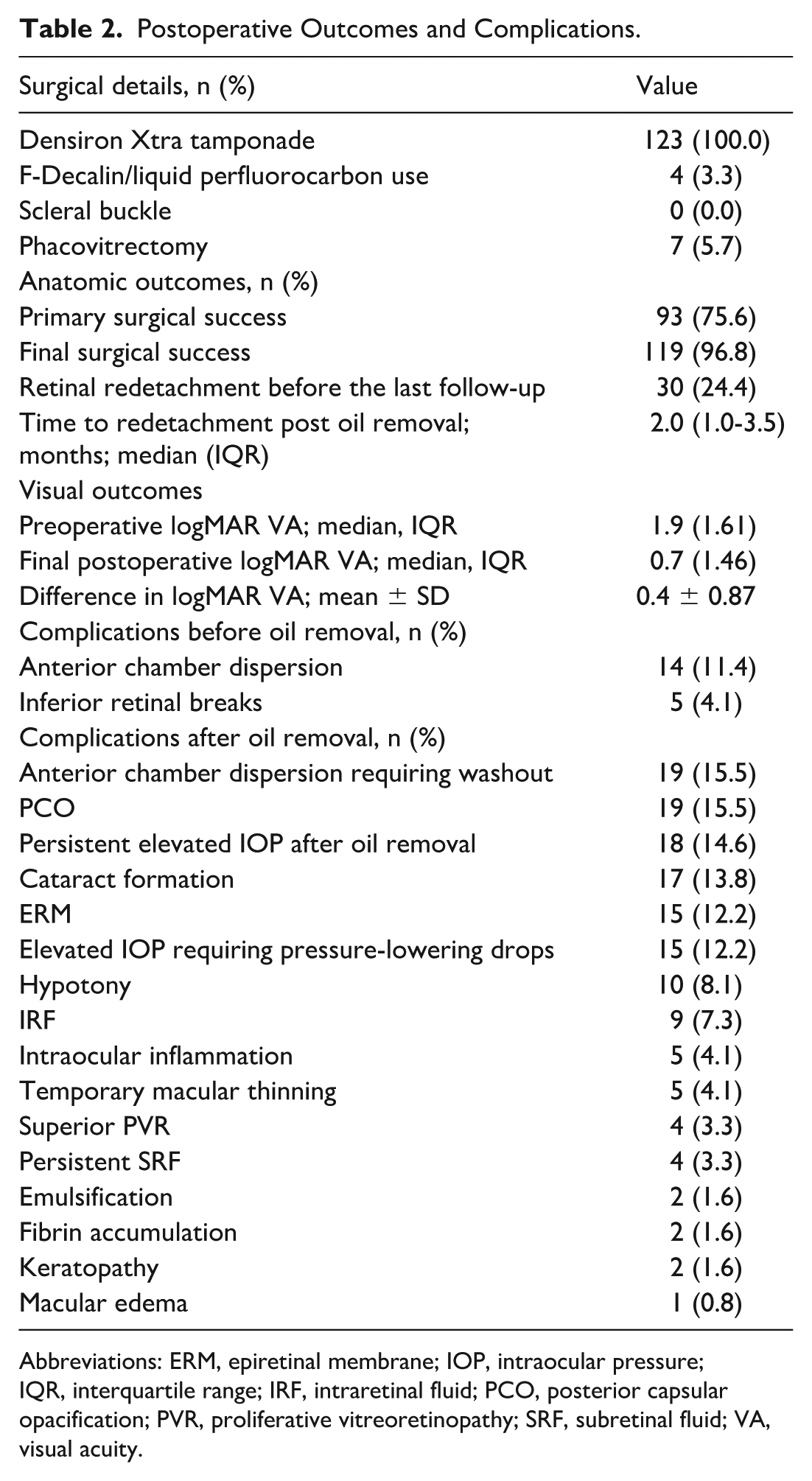
Abbreviations: ERM, epiretinal membrane; IOP, intraocular pressure; IQR, interquartile range; IRF, intraretinal fluid; PCO, posterior capsular opacification; PVR, proliferative vitreoretinopathy; SRF, subretinal fluid; VA, visual acuity.
Surgical Procedure
All surgeries were performed by an experienced vitreoretinal surgeon (PY) using a standard 3-port pars plana vitrectomy technique with scleral depression and peripheral vitreous shaving to the vitreous base. Vitrectomy was combined with retinotomy, retinectomy, membrane peeling, or the addition of perfluorocarbon liquid, as required. Endolaser photocoagulation was applied around retinal breaks, and low-viscosity heavy silicone oil was infused into the vitreous cavity. No eyes underwent 360-degree laser photocoagulation or scleral buckling. Low-viscosity heavy silicone oil was removed in all cases using standard 23-gauge viscous fluid extrusion tubing attached to a syringe. Surface tension maintained the oil bubble at the extrusion tip, and in rare instances where droplets settled on the macula, a 25-gauge cannula was used for removal.
Data Analysis
All statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS, Inc.). Continuous variables were expressed as mean ± SD or median and interquartile range (IQR), as appropriate, and categorical variables were reported as numbers and percentages. Analysis of variance was used to evaluate differences between preoperative and postoperative logMAR VA according to the following covariates: age, primary retinal detachment status, number of retinal detachment quadrants, PVR grade C/D, lens status, and macular status. Multivariable logistic regression analysis was performed to assess factors associated with retinal redetachment during the study period and at the final follow-up, including age, primary retinal detachment status, extent of retinal detachment in clock hours, macular status, and PVR grade C/D. Variables were determined based on existing literature.3,29,30 Statistical significance was defined as P < .05.
Results
Baseline demographic and clinical characteristics are summarized in Table 1. Of the 123 patients, 49 (39.5%) were women, with a median age of 66 (IQR, 61-73) years. All 123 eyes represented unique cases of RRD, and 52 eyes (42.3%) had a history of a prior retinal detachment. The mean follow-up duration was 16.3 ± 5.05 months, and the mean tamponade duration was 10.4 ± 3.71 (range, 3–26) weeks. All cases had inferior RRD involving a median of 7 (IQR, 5.9-9.0) clock hours. Macula-off detachments were present in 83 eyes (67.5%), and 105 eyes (85.4%) had PVR grade C/D. Epiretinal membrane (ERM), macular hole, and vitreous hemorrhage were present in 13 (10.6%), 12 (9.8%), and 4 (3.3%) eyes, respectively. With regard to lens status, 73 patients (59.3%) were phakic and 50 (40.7%) were pseudophakic.
Table 2 describes the surgical features and outcomes. No cases required scleral buckle placement during the initial surgery or any subsequent surgeries. Perfluorocarbon liquid was used in 4 eyes (3.3%), and combined phacovitrectomy was performed in 7 eyes (5.7%). Primary and final surgical success rates were 75.6% and 96.8%, respectively. Retinal redetachment occurred in 30 eyes (24.4%), at a median of 2 (IQR, 1.5-3.0) months after oil placement and 2 (IQR, 1.0-3.5) months after oil removal. Among eyes with redetachment, 23 (76.7%) required 1 additional surgery, and 3 (10.0%) required 2 additional surgeries. Four eyes (13%) failed to achieve retinal reattachment despite 2 additional surgeries with low-viscosity heavy silicone oil. Of these, 2 eyes subsequently underwent placement of Siluron, whereas 2 patients declined further intervention. The mean improvement in logMAR VA was 0.4 ± 0.87 (P < .001).
Postoperative complications before oil removal included anterior chamber dispersion in 14 eyes (11.4%) and inferior retinal breaks in 5 eyes (4.1%). After oil removal, postoperative complications included anterior chamber dispersion requiring washout in 19 eyes (15.5%), posterior capsule opacification (PCO) in 19 eyes (15.5%), persistent elevated intraocular pressure after heavy silicone oil removal in 18 eyes (14.6%), cataract formation in 17 eyes (13.8%), epiretinal membrane formation in 15 eyes (12.2%), elevated intraocular pressure requiring pressure-lowering drops in 15 eyes (12.2%), hypotony in 10 eyes (8.1%), intraretinal fluid in 9 eyes (7.3%), intraocular inflammation in 5 eyes (4.1%), temporary macular thinning in 5 eyes (4.1%), superior PVR in 4 eyes (3.3%), persistent subretinal fluid in 4 eyes (3.3%), emulsification in 2 eyes (1.6%), fibrin accumulation in 2 eyes (1.6%), keratopathy in 2 eyes (1.6%), and macular edema in 1 eye (0.8%).
Multivariate regression showed no significant associations with retinal redetachment during the study period or at the end of the study. Similarly, analysis of variance demonstrated no significant differences in preoperative-to-postoperative changes in logMAR VA across the evaluated covariates.
Figure 1 presents a representative case of a patient treated with low viscosity HSO tamponade. Figure 2 illustrates a case exhibiting temporary macular thinning.
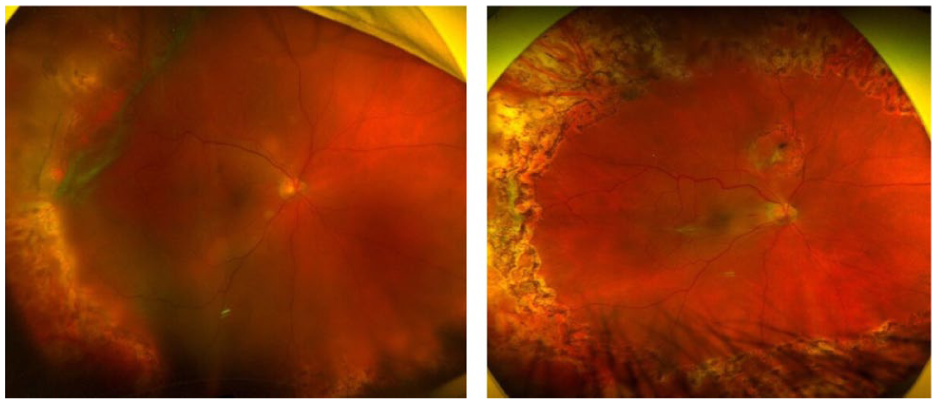
Representative case of a 77-year-old patient with rhegmatogenous retinal detachment complicated by proliferative vitreoretinopathy before surgery (left), treated with Densiron Xtra tamponade. The retina remained fully attached at 12 months after postoperative removal of Densiron Xtra tamponade (right).
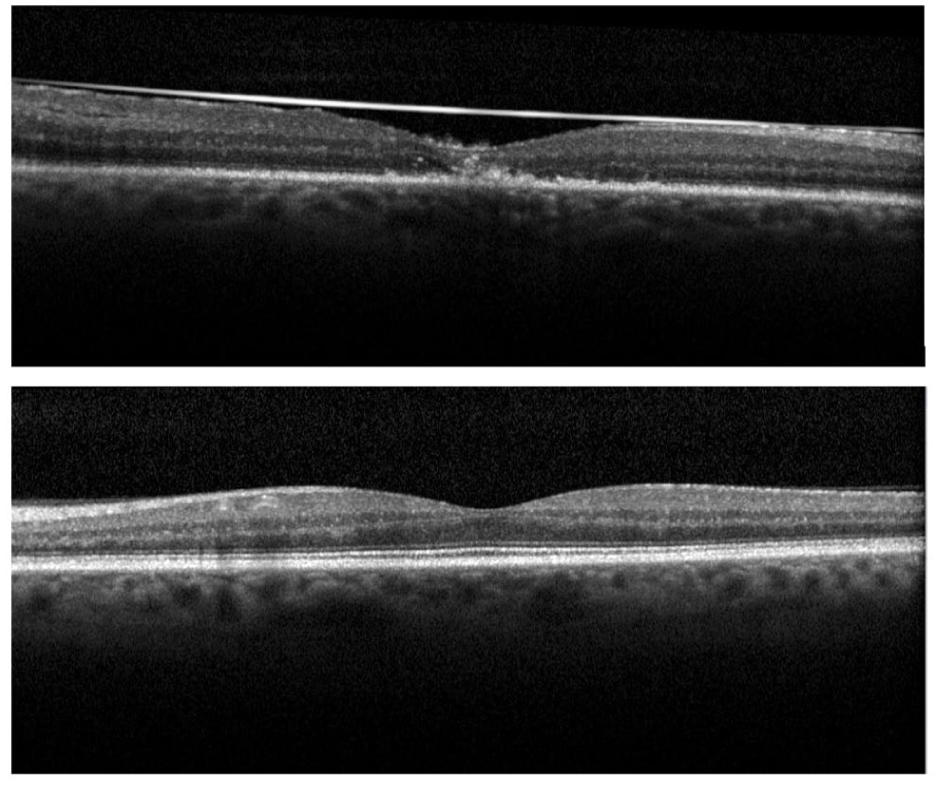
Representative optical coherence tomography images from a 68-year-old patient demonstrating temporary foveal atrophy after placement of Densiron Xtra tamponade (top), with complete recovery of foveal architecture 3 months after oil removal (bottom).
Conclusions
In our case series, which included a large subset of cases complicated by PVR, low-viscosity heavy silicone oil achieved excellent anatomic and functional outcomes with low complication rates, supporting its role as a reliable and safe tamponade for inferior and complex RRD.
We observed a significant improvement in final VA, consistent with findings from previous case series evaluating low-viscosity heavy silicone oil.16,24 Our results further support the efficacy of low-viscosity heavy silicone oil in achieving favorable visual outcomes for complex RRD.
Our final anatomic success rate of 96.8% is comparable to rates of 97.5% 24 and 100% 16 reported in other case series evaluating low-viscosity heavy silicone oil. Despite a higher proportion of eyes with PVR in our cohort compared with these studies, retinal redetachment rates did not differ according to PVR status. Similarly, no difference was observed in redetachment rates based on lens status, underscoring the efficacy of low-viscosity heavy silicone oil for retinal reattachment. These findings support the effectiveness of low-viscosity heavy silicone oil in providing tamponade support for the inferior and posterior retina in RRD with PVR.
We observed a retinal redetachment rate of 24.4%. Of the 30 redetachments, 5 occurred from inferior retinal breaks before oil removal, 4 (3.3%) were associated with superior PVR after oil removal, and the remaining 21 resulted from inferior retinal breaks after oil removal. Although prior studies on low-viscosity heavy silicone oil did not specifically discuss retinal redetachment rates,16,24 our findings compare favorably with reported rates of 38.7% and 33.3% in separate studies evaluating high-viscosity heavy silicone oil in complex recurrent retinal detachments.2,31
Dispersion refers to the mechanical breakup of large oil bubbles into smaller droplets in the absence of biological surfactants or migration of inflammatory factors.15,32 Among the 14 patients (11.4%) with anterior chamber dispersion before oil removal, oil bubbles disappeared in 8 patients after oil removal, likely due to posterior settling related to the high specific gravity of the oil. The remaining 6 patients were observed without intervention, and the dispersed bubbles resolved within 3 months after oil removal. Dispersion to the anterior chamber after oil removal was observed in 19 patients (15.5%) who underwent anterior chamber washout. Although prior case series evaluating low-viscosity heavy silicone oil series did not report dispersion rates, our findings are lower than reported rates of up to 38.8% for high-viscosity heavy silicone oils.
Emulsification occurs when dispersed oil droplets are stabilized by inflammation or surfactants, rendering simple drainage ineffective and necessitating more extensive removal techniques such as air–fluid exchange. 32 Emulsification occurred in 2 eyes (2%), consistent with or lower than rates reported for both low-viscosity16,24 and high-viscosity heavy silicone oils (0%–16%).1,33 In our series, VA improved in 1 patient following successful oil removal and remained unchanged in another patient in whom emulsified oil could not be completely extracted. Low-viscosity heavy silicone oil is less prone to both dispersion and emulsification compared with high-viscosity heavy silicone oil, because the higher-molecular-weight silicone compounds increase extensional viscosity and resistance to shearing forces.21–23 Additionally, the mean tamponade duration in our series was 10.4 weeks, which is shorter than the 6-month threshold associated with an increased risk of emulsification.34,35
Intraocular inflammation and fibrin accumulation occurred in 5 eyes (4.1%) and 2 eyes (1.6%), respectively. Our rate of intraocular inflammation was slightly higher than the 0% rate previously reported in a small series of 3 eyes treated with low-viscosity heavy silicone oil, likely reflecting the small sample size of that study. 16
Inflammation rates of up to 40.7% have been reported with high-viscosity heavy silicone oil and have been associated with longer tamponade duration.23,36,37 Keratopathy, cataract formation, and PCO occurred in 1.6%, 13.8%, 15.5% of the eyes, respectively, which is consistent with or lower than rates reported for both low-viscosity16,24 and high-viscosity heavy silicone oils.5,17 The low incidence of inflammation and anterior segment pathologies in our series likely reflects the enhanced resistance of low-viscosity heavy silicone oil to emulsification. Emulsified droplets may activate phagocytic cells, contributing to postoperative inflammation, cataract formation, and PCO.38,39 Emulsification may also contribute to keratopathy through mechanical blockage in the cornea. 34
In our cohort, 5 eyes (4.1%) demonstrated temporary macular thinning that resolved within 6 months after tamponade removal, accompanied by improved visual function. Although this finding has not previously been reported for low-viscosity heavy silicone oil, reversible macular thinning after oil removal has been described with high-viscosity heavy silicone oil.11,40 Proposed mechanisms include mechanical stress or retinal dehydration associated with the hydrophobic oil.41–44 Importantly, this thinning often improves or resolves following oil removal, indicating recovery of retinal function rather than permanent structural damage. 45
The limitations of this study include its retrospective design, lack of a comparator group, and absence of treatment randomization. In addition, all cases were managed at a single surgical center conducted by the same surgeon, which may limit the generalizability of our findings.
In conclusion, our study demonstrates that low-viscosity heavy silicone oil provides excellent anatomic and visual outcomes with low complication rates, supporting its safety and effectiveness as a tamponade for inferior RRD complicated by PVR. Recent comparative studies indicate that newer-generation heavy silicone oils achieve higher primary reattachment rates and greater visual improvement compared with standard silicone oils, with or without scleral buckle placement, in RRD with inferior breaks and PVR.14,24 These findings reinforce the clinical advantages of low-viscosity heavy silicone oils in the management of complex inferior retinal detachments.
Footnotes
Acknowledgements
The authors thank all staff members who assisted with data collection.
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board at Wayne State University (Detroit, MI, USA) (approval no. 021319MP2X/1902002026).
Consent to Participate
Informed consent was waived for the present study because inclusion in the study posed no substantial risk to participants, and data analysis consisted of de-identified data obtained through retrospective review.
Consent for Publication
Informed consent for publication of clinical data was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to patient confidentiality considerations but are available from the corresponding author upon reasonable request.