
Abstract
Keywords
Introduction
A cataract is the opacification of the native lens of the eye, most commonly occurring secondary to advanced age, but also can be related to ocular trauma, congenital infection, or systemic disease. 1 The current gold standard surgical management for cataract removal is phacoemulsification with intraocular lens (IOL) implantation into the capsular bag. 2 Primary IOL placement into the capsular bag is preferred in the setting of adequate capsular and zonular support, as it mimics the anatomic position of the natural lens. 3 Zonular instability can arise due to a variety of conditions, including advanced age, genetic collagen malformation, and pseudoexfoliation syndrome, as well as in the setting of trauma. 4 Posterior capsule rupture leading to inadequate capsular support can also occur secondary to external trauma or during complicated phacoemulsification surgery.5,6 In the setting of zonular instability or inadequate capsular support, an alternative site for IOL placement is considered, such as within the anterior chamber, fixated to the iris, or fixated to the sclera, or sutured to the sclera using 2-point or 4-point fixation.3,7
Since their introduction, there has been significant improvement in the materials and techniques for placement of alternative-site IOLs, yielding improved outcomes and increasing physician use.8–14 Although each IOL has been studied independently, there is little consensus in the literature on a superior alternative-site IOL location. The scleral-sutured IOL is thought to have a strong ocular safety profile due to its placement and stability.14,15 The scleral-sutured IOL is fixed to the sclera using sutures, which pass through the lens haptics, as well as sclerotomies, which are generally 2 to 3 mm posterior to the limbus, in order to place the lens in the ciliary sulcus.10,16 This location most closely mimics the natural anatomy of a crystalline lens and ideally spares operative damage to the corneal endothelium or iris.15,17 Avoiding these ocular structures may make the scleral-sutured IOL a safer option in patients with diabetes, who have increased risk of inflammation due to compromised vascular permeability, in patients with low endothelial cell counts, and in patients with a shallow anterior chamber, who are poor candidates for anterior chamber IOL. 17 In eyes of younger patients, the scleral-sutured IOL has been proposed as a superior, long-term alternative to the anterior chamber IOL or iris-fixated IOL, which have been reported to be associated with significant loss of endothelial cell density over time.18,19 However, comparative data on long-term complications are lacking due to the relative novelty of the scleral-sutured lens technique.
Scleral-sutured IOLs have been extensively studied in the literature, with most studies being meta-analyses, case studies, or case series that primarily report visual, refractive, and complication outcomes following the surgery. There are also continued modifications and advancements in scleral-sutured IOL surgical techniques, including the recent emergence of sutureless scleral fixation. 20 Though the efficacy and positive outcomes of scleral-sutured IOLs have been consistently demonstrated, factors influencing postoperative refractive and vision success are still scarcely described. This retrospective study utilized the robust number of IOL placements performed at the Cole Eye Institute and subsequent thorough electronic medical record (EMR) documentation 21 in the Cleveland Clinic Foundation (CCF) system to close this literature gap. The goal of this study was to explore whether patient-specific or operative factors are associated with visual and refractive success in patients following scleral-sutured IOL placement.
Methods
Participants
This was a retrospective cohort study of eyes that received a scleral-sutured IOL at a large academic medical center between January 1, 2013, and July 31, 2022. Chart review proceeded after approval from the Cleveland Clinic Investigational Review Board. Inclusion criteria were being at least age 18 years at the time of IOL insertion and having at least 1 follow-up visit within the CCF network following the surgery. Eyes receiving an IOL were identified based on Current Procedural Terminology codes 66985 and 66986, and scleral-sutured IOL cases were identified through review of surgical procedure notes. Exclusion criteria were having a concurrent ophthalmic procedure (defined as any additional surgical intervention besides pars plana vitrectomy, including but not limited to cataract removal, epiretinal membrane peeling, silicone oil removal, or Descemet’s stripping automated endothelial keratoplasty) at the time of IOL insertion, or having the surgery or follow-up performed at an outside institution (Figure 1).
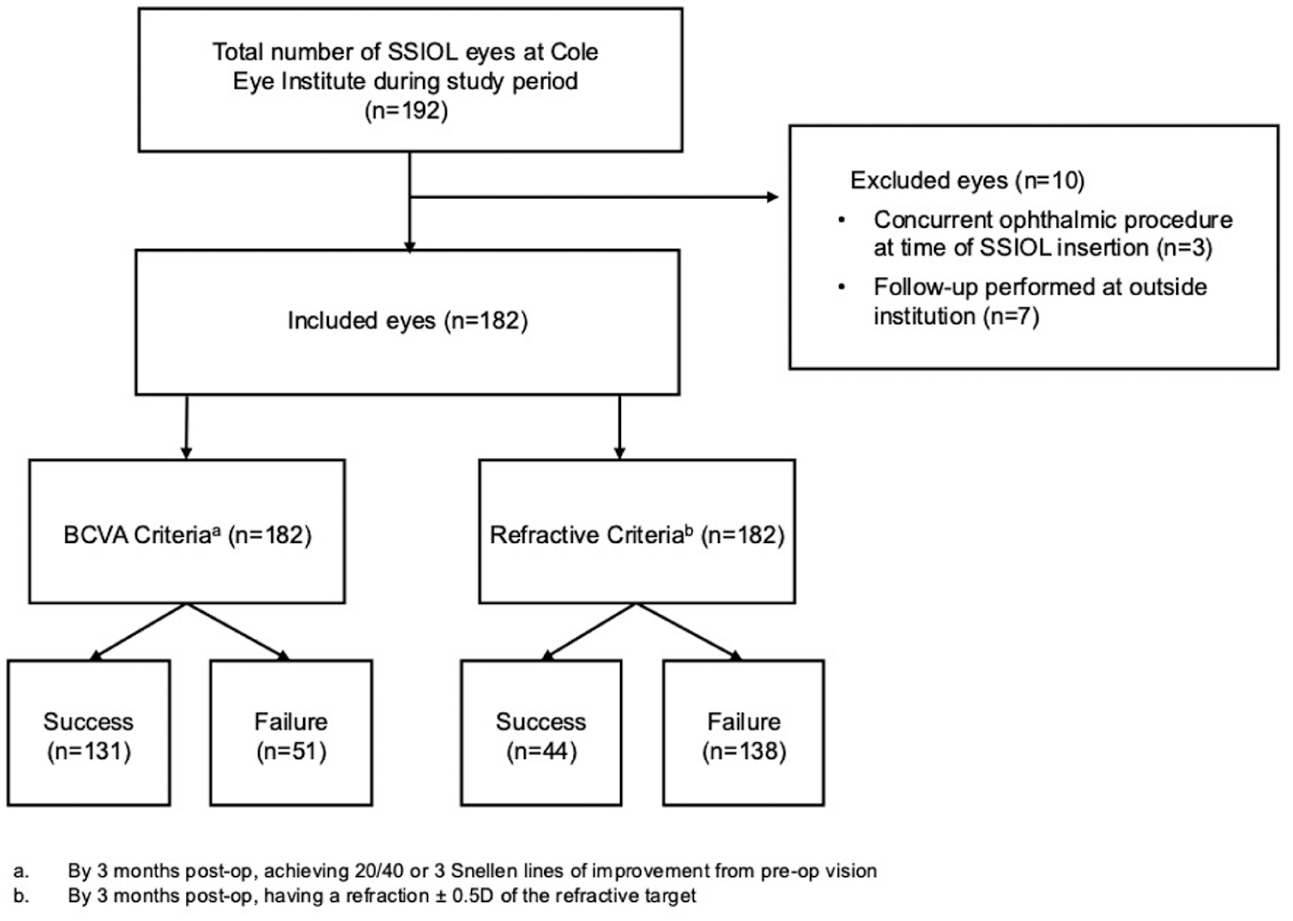
Distribution of patients based on study inclusion and exclusion criteria, and evaluation of success or failure of scleral-sutured intraocular lens (SSIOL) implantation (conducted in the study period January 1, 2013, to July 31, 2022), using best-corrected visual acuity (BCVA) and refraction at 3 months postoperatively (post-op) as outcomes.
Outcome Measures
The primary aim of this study was to identify variables associated with successful vision outcomes following scleral-sutured IOL placement. Based on existing literature, vision success was defined as achieving a visual acuity (VA) improvement to 20/40 (logMAR change –0.30) or at least 3 Snellen lines of improvement by 3 months postoperatively as compared with preoperative vision.9,12,14,22 To account for underlying ophthalmic conditions, such as ocular trauma, which can limit final visual potential, we also included patients who achieved 3 Snellen lines of improvement. Best-corrected visual acuity (BCVA) was converted to logMAR using the formula logMAR = –log(Snellen decimal), and categorical VA, such as counting figures or hand motion, was converted using a logMAR conversion to enable comparability. 23 For the purposes of the study, BCVA was defined as the best vision recorded (VA uncorrected or corrected at distance ± pinhole) in the preoperative visit most immediate to the surgical date and the 3-month postoperative visit.
A secondary aim of this study was to understand the variables associated with refractive success after scleral-sutured IOL placement. Alongside vision success, this complementary measure of surgical success serves to prevent overinterpretation of success based on pinhole acuity alone. By aggregating existing literature reporting refractive outcomes, refractive success was defined as meeting within 0.5 diopters of the preoperative refractive target by 3 months postoperation.9,14,24,25 Although refractive success is often clinically defined as achieving a postoperative refraction within 1.0 diopters of the preoperative target, for the purposes of increasing precision and enabling a more granular analysis of variables, a stricter criteria of 0.5 diopters was utilized. Included eyes were categorized according to 3-month postoperative surgical outcomes into success and failure groups, as determined based on the aforementioned definitions.
Statistical Analysis
Demographic, biometric, preoperative, intraoperative, and 3-month postoperative variables were collected using EMRs (Supplemental Table 1). 21 For example, the scleral-sutured IOL lens placed intraoperatively (Akreos AO60 [Bausch + Lomb], CZ70BD [Alcon], or enVista [Bausch + Lomb]) was determined based on surgeon preference and recorded using procedure notes. Additional analysis of outcomes with use of the Akreos AO60 lens compared with the CZ70BD lens was performed to determine the influence of surgeon variability, preoperative BCVA, and ocular comorbidities on vision success. Numerical data were described as the mean with SD for normally distributed variables and median with interquartile range (IQR) for nonnormally distributed variables. Continuous variables were compared between vision/refractive success and failure groups using independent t tests or Wilcoxon rank-sum tests. Categorical variables were described using counts and percentages and compared across vision/refractive success and failure groups using χ2 or Fisher exact tests.
We additionally performed multivariable logistic regression analyses, reporting odds ratios (ORs) with their 95% CIs and P values. To avoid overfitting these models, we utilized the 10:1 event-to-regression coefficient rule, where the event is the less frequent state of the binary outcome, to identify the desired number of variables. We then utilized a random forest model to identify the variables most strongly associated with the outcome of interest based on the variable importance rankings. In this model, the variables found to be most strongly associated with vision success were baseline BCVA, brand of IOL implant, patient age, and the number of ocular conditions. For refractive success, the model demonstrated the strongest associations with implant power, procedure length, patient age, and baseline IOP. These top variables of interest were incorporated into the logistic regression analyses.
Associations with demographic characteristics and results of univariate and multivariate analyses for likelihood of BCVA and refractive success were repeated after matching by primary IOL indication (Supplemental Tables 2–7).
In addition, scatter plots were generated to further describe any relationship between the variables of clinical interest and the absolute error difference between the target refraction and the 3-month postoperative refraction.
All statistical analyses were performed using JMP Pro version 18 (SAS Institute). Forest plots were generated in Rstudio version 2023.06.0+421, and scatter plots were generated in Microsoft Excel. Statistical significance was defined as a P value less than or equal to .05.
Results
Baseline Characteristics
In this retrospective cohort, the majority of eyes (113 of 182, 62%) were in male patients (Table 1). At baseline, the mean number of ocular comorbidities was 1.2, most commonly ocular hypertension or glaucoma, and the mean number of previous ocular surgeries was 1.5, most frequently cataract removal with IOL implantation (Tables 1 and 2). Patients were generally healthy, with the mean number of systemic chronic disorders in the whole cohort being 1.1.
Demographic and Clinical Characteristics of Patients Receiving a Scleral-Sutured Secondary IOL (N = 182).
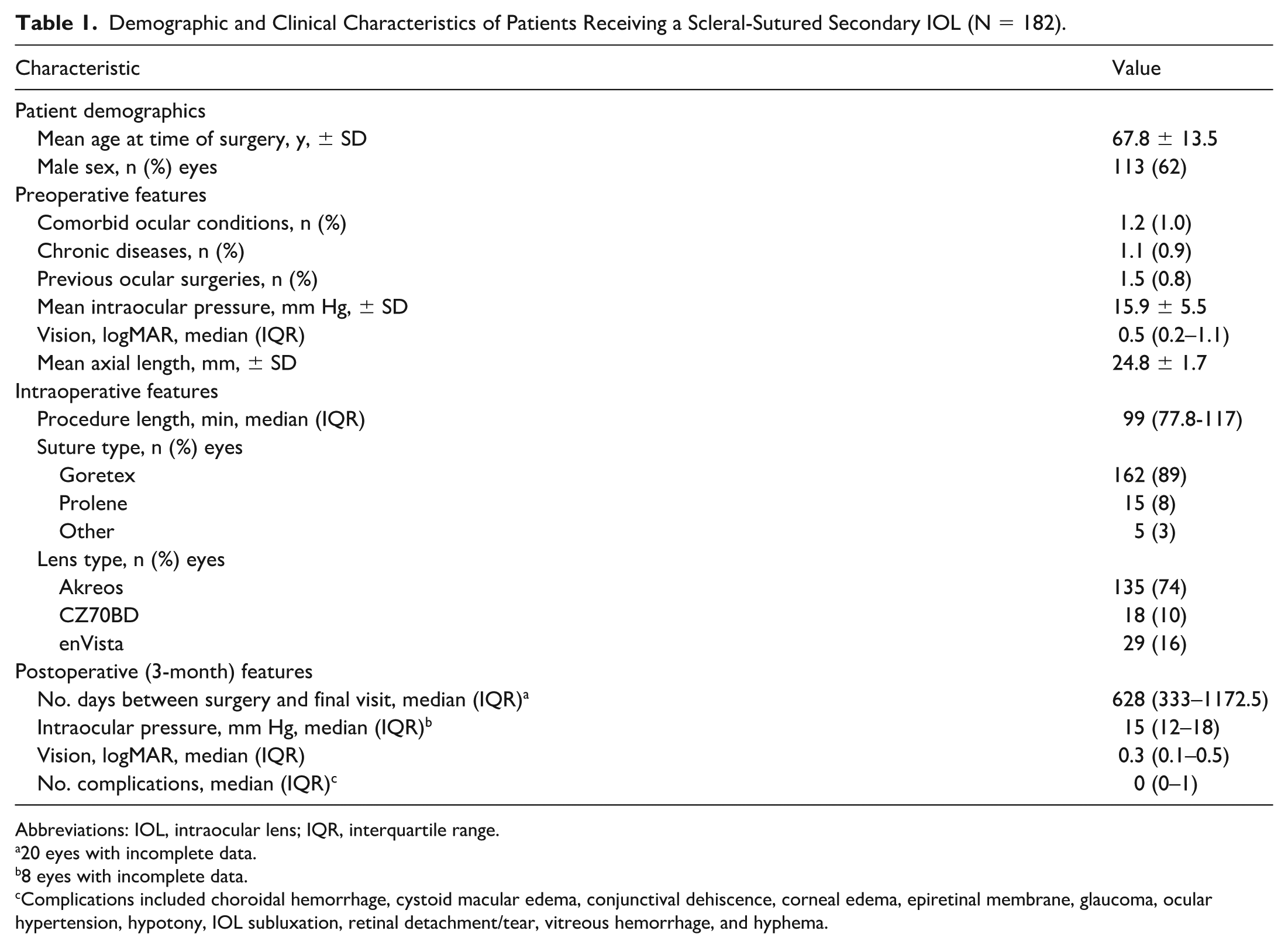
Abbreviations: IOL, intraocular lens; IQR, interquartile range.
20 eyes with incomplete data.
8 eyes with incomplete data.
Complications included choroidal hemorrhage, cystoid macular edema, conjunctival dehiscence, corneal edema, epiretinal membrane, glaucoma, ocular hypertension, hypotony, IOL subluxation, retinal detachment/tear, vitreous hemorrhage, and hyphema.
Ocular Comorbidities, Surgical History, and Indication for Scleral-Sutured IOL by Postoperative Success or Failure Outcomes. a
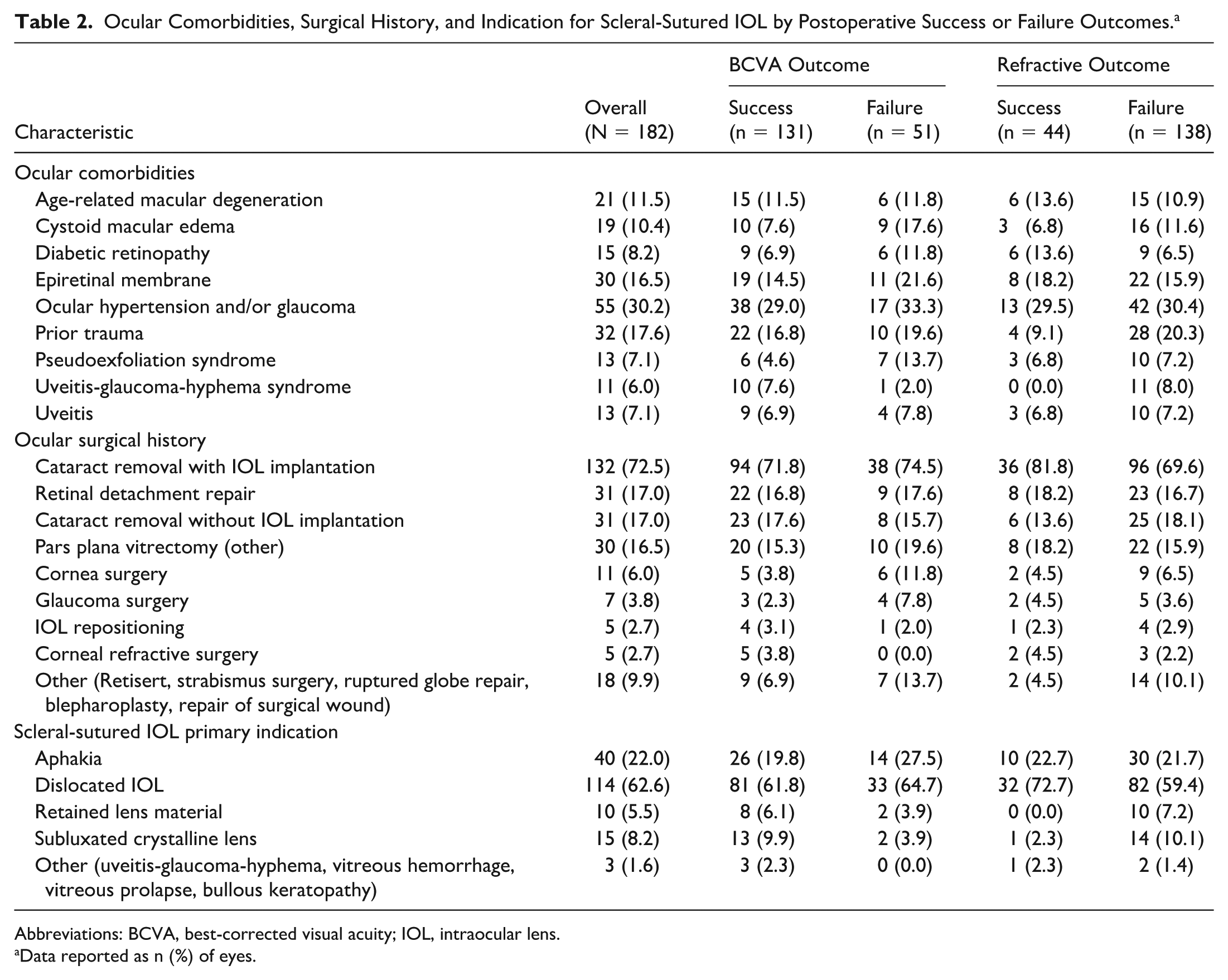
Abbreviations: BCVA, best-corrected visual acuity; IOL, intraocular lens.
Data reported as n (%) of eyes.
The mean axial length was 24.8 mm, and median preoperative VA was 0.5 logMAR (mean Snellen equivalent 20/63). The most common indication for surgery was a dislocated or malpositioned IOL (114 cases), followed by aphakia (40 cases) (see Table 2 for all other indications). The median time for duration of surgery was under 2 hours (median, 99 minutes, IQR, 77.8–117 minutes), with a median follow-up period of 1.7 years.
Postoperative Characteristics
By 3 months postoperatively, scleral-sutured IOL placement was associated with a 37% improvement in logMAR VA, or about 2 Snellen lines of vision gained. Eyes had a stable intraocular pressure at 3 months, and the median number of complications was 0 (Table 1). The most prevalent complication at 3 months was cystoid macular edema. All active complications at 3 months postoperatively and at the last collected visit are detailed in Table 3.
Active Complications at 3 Months Postoperatively and at the Final Visit After Scleral-Sutured IOL Insertion, by Success or Failure Outcomes. a
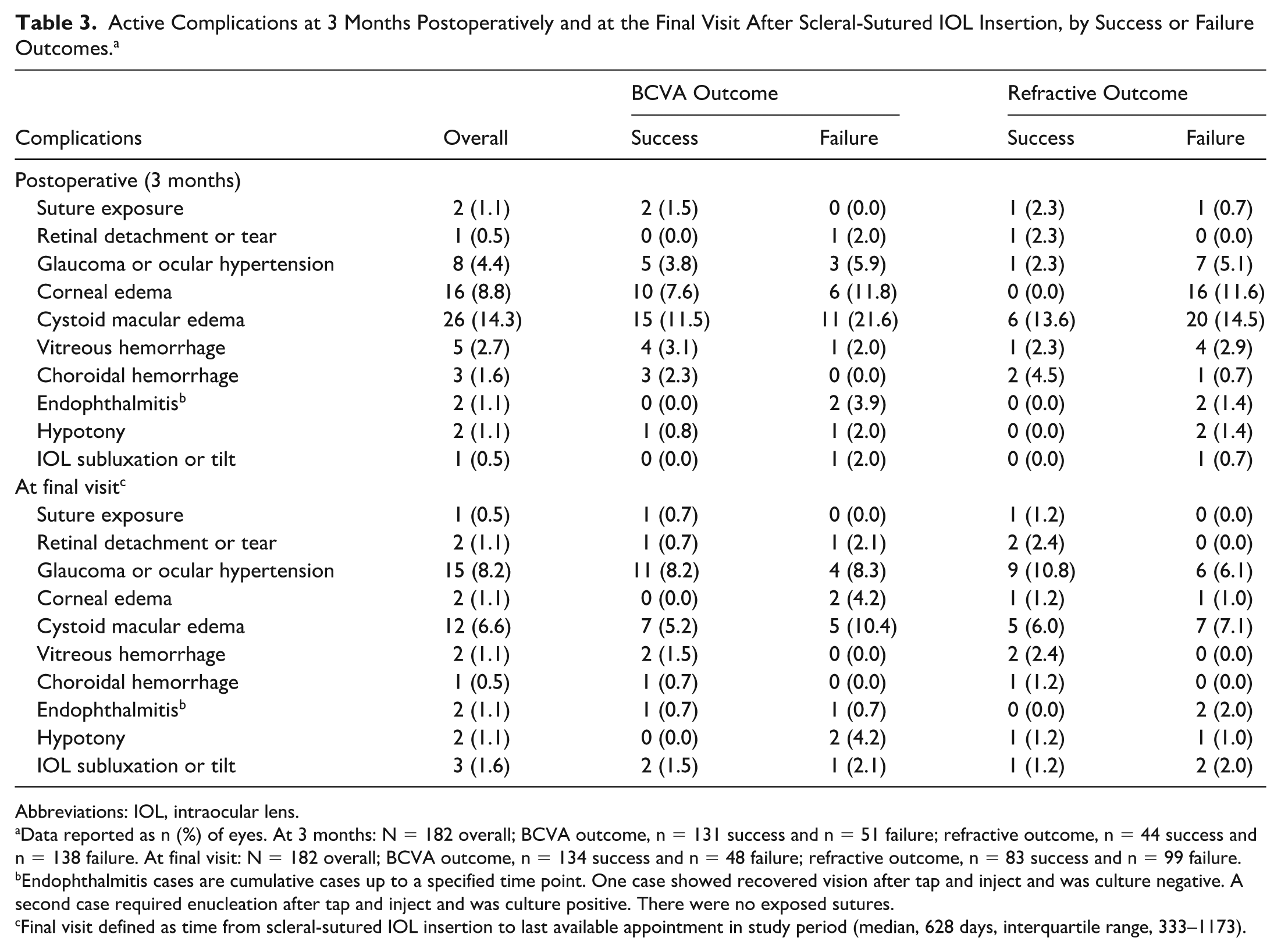
Abbreviations: IOL, intraocular lens.
Data reported as n (%) of eyes. At 3 months: N = 182 overall; BCVA outcome, n = 131 success and n = 51 failure; refractive outcome, n = 44 success and n = 138 failure. At final visit: N = 182 overall; BCVA outcome, n = 134 success and n = 48 failure; refractive outcome, n = 83 success and n = 99 failure.
Endophthalmitis cases are cumulative cases up to a specified time point. One case showed recovered vision after tap and inject and was culture negative. A second case required enucleation after tap and inject and was culture positive. There were no exposed sutures.
Final visit defined as time from scleral-sutured IOL insertion to last available appointment in study period (median, 628 days, interquartile range, 333–1173).
BCVA Outcome
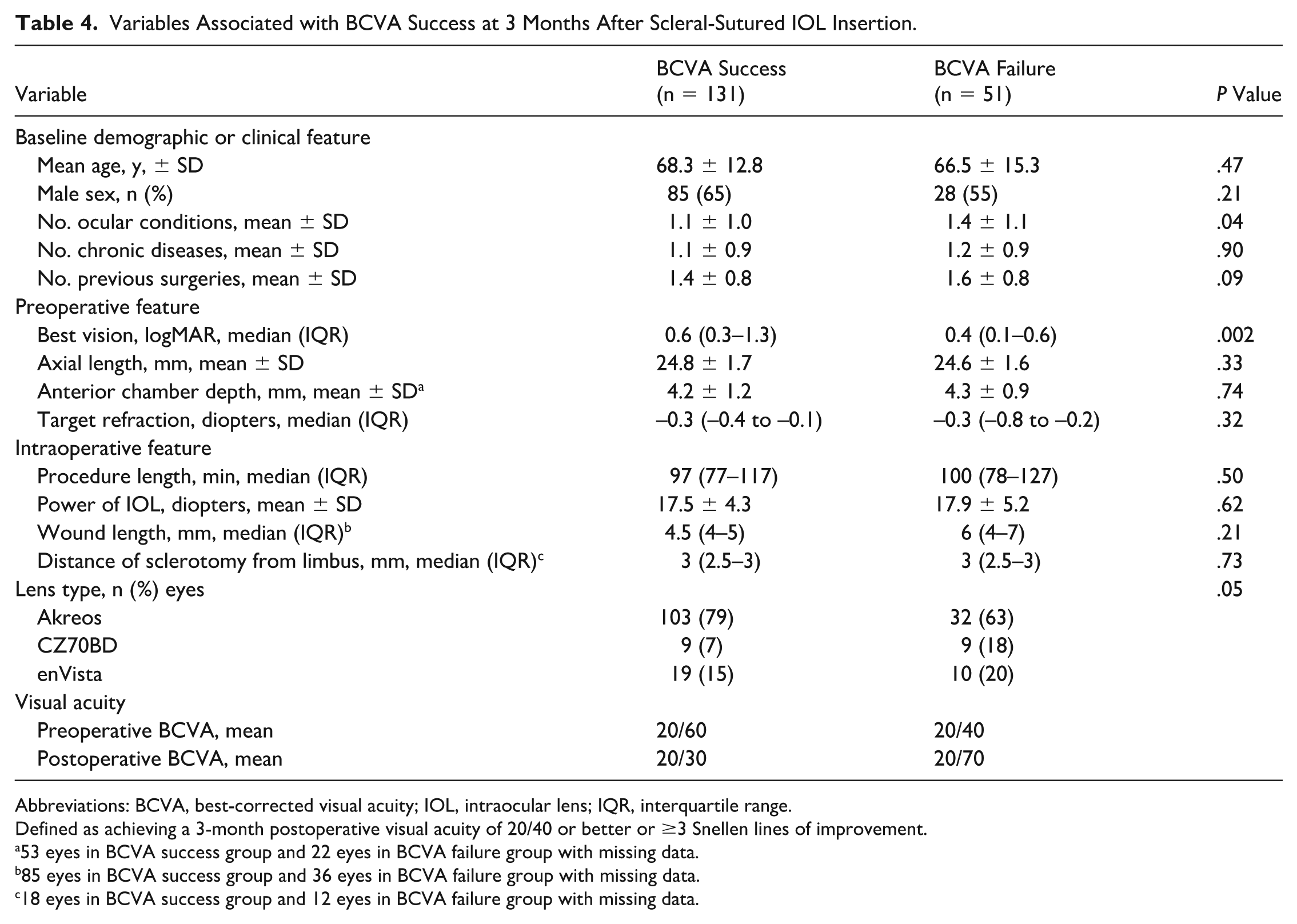
Overall, 72% of the 182 eyes met the BCVA success criteria (3 lines of vision gain or Snellen VA 20/40 or better) at 3 months postoperatively (Table 4). Eighty-four eyes met the 3 lines of vision gain criteria and 109 eyes met the 20/40 vision criteria, suggesting that a total of 62 eyes achieved BCVA success following scleral-sutured IOL implantation through meeting both of the defined success criteria. VA in the success group improved from a mean 20/60 to 20/30, while the failure group worsened from a mean 20/40 to 20/70.
Variables Associated with BCVA Success at 3 Months After Scleral-Sutured IOL Insertion.
Abbreviations: BCVA, best-corrected visual acuity; IOL, intraocular lens; IQR, interquartile range.
Defined as achieving a 3-month postoperative visual acuity of 20/40 or better or ≥3 Snellen lines of improvement.
53 eyes in BCVA success group and 22 eyes in BCVA failure group with missing data.
85 eyes in BCVA success group and 36 eyes in BCVA failure group with missing data.
18 eyes in BCVA success group and 12 eyes in BCVA failure group with missing data.
Patient age, sex, number of prior ocular surgeries, and number of systemic chronic disorders were not associated with achieving postoperative vision success. Variables associated with greater odds of BCVA success were having fewer preexisting ocular comorbidities (mean ± SD number, 1.1 ± 1.0 in success group vs 1.4 ± 1.1 in failure group; P = .04), worse preoperative BCVA (median 0.6 logMAR in success group vs 0.4 logMAR in failure group; P = .002), and use of the Akreos AO60 lens (Bausch + Lomb) compared with the CZ70BD lens (Alcon) (P = .05). There was no significant association of use of the enVista lens (Bausch + Lomb) with BCVA success. Matching 102 eyes on IOL indication showed a loss of statistical power and evidence of remaining covariate imbalance (standardized difference >0.1) (Supplemental Table 3).
The multivariable logistic regression analysis (Figure 2) demonstrated that having worse preoperative vision was associated with higher odds of postoperative vision success (OR, 3.92, 95% CI, 2.03–8.66; P < .001), whereas having more preexisting ocular conditions was associated with lower odds of postoperative vision success (OR, 0.55, 95% CI, 0.37–0.78; P = .001). Similarly, use of the CZ70BD lens was associated with lower odds of postoperative vision success compared with use of the Akreos lens (OR, 0.23, 95% CI, 0.07–0.72; P = .01). Eyes that received the enVista lens did not show significant associations with vision success. IOL indication–matched analysis did not change these significant results (Supplemental Table 4).
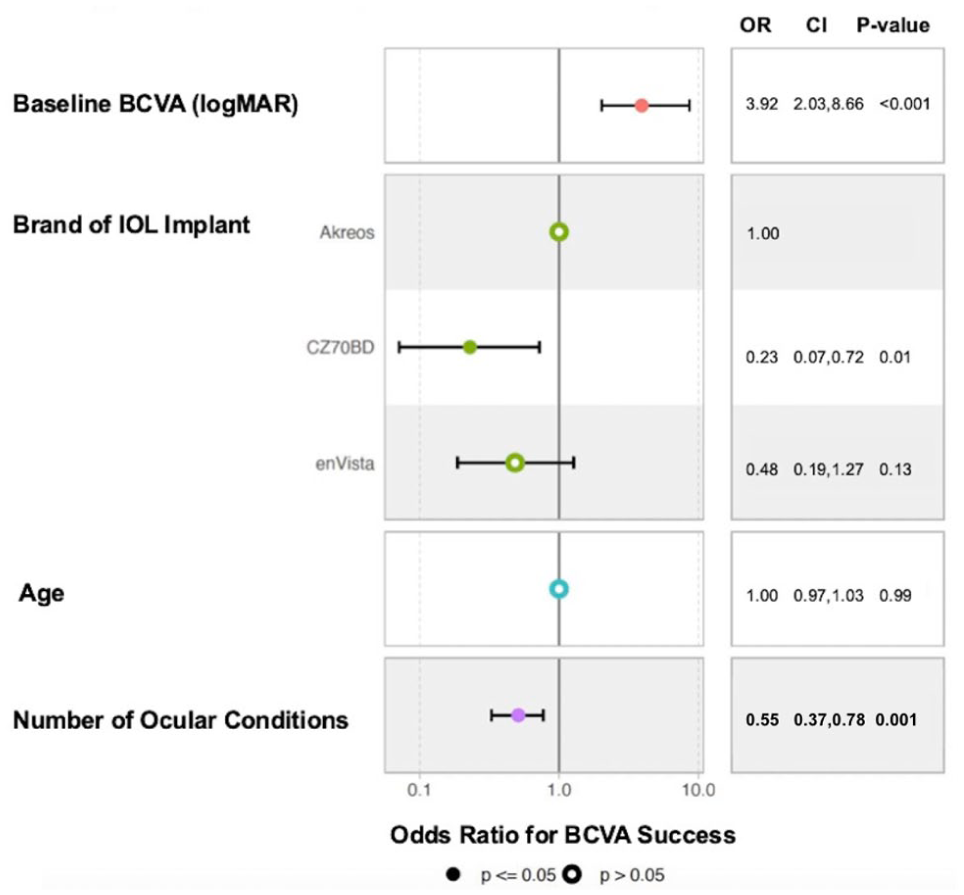
Forest plot depicting multivariable logistic regression analysis results for the 4 variables most predictive of BCVA success.
Further analyses assessing whether there were outcome differences based on use of the Akreos AO60 lens vs use of the CZ70BD lens found that 10 surgeons performed implantation with Akreos AO60 lenses and 4 surgeons used CZ70BD lenses. Only 1 of the 4 surgeons in the CZ70BD lens group was not represented in the Akreos AO60 lens group, and this surgeon was responsible for 1 case (5.6%) of the overall 18 CZ70BD lens cases. The remaining 17 (94%) of 18 CZ70BD lens procedures were performed by 3 surgeons who also performed 21 (15.6%) of the 135 Akreos AO60 lens procedures. Comparison of preoperative BCVA between the lens brands showed no statistically significant difference (median BCVA, 0.54 logMAR [IQR, 0.18–1.18] for Akreos vs 0.57 logMAR [IQR, 0.4–0.95] for CZ70BD; P = .77). Similarly, there was no significant difference in the number of chronic ocular comorbidities between patients in each lens brand group (mean ± SD number, 1.2 ± 1.1 for Akreos vs 0.8 ± 1.0 for CZ70BD; P = .10).
Refractive Outcome
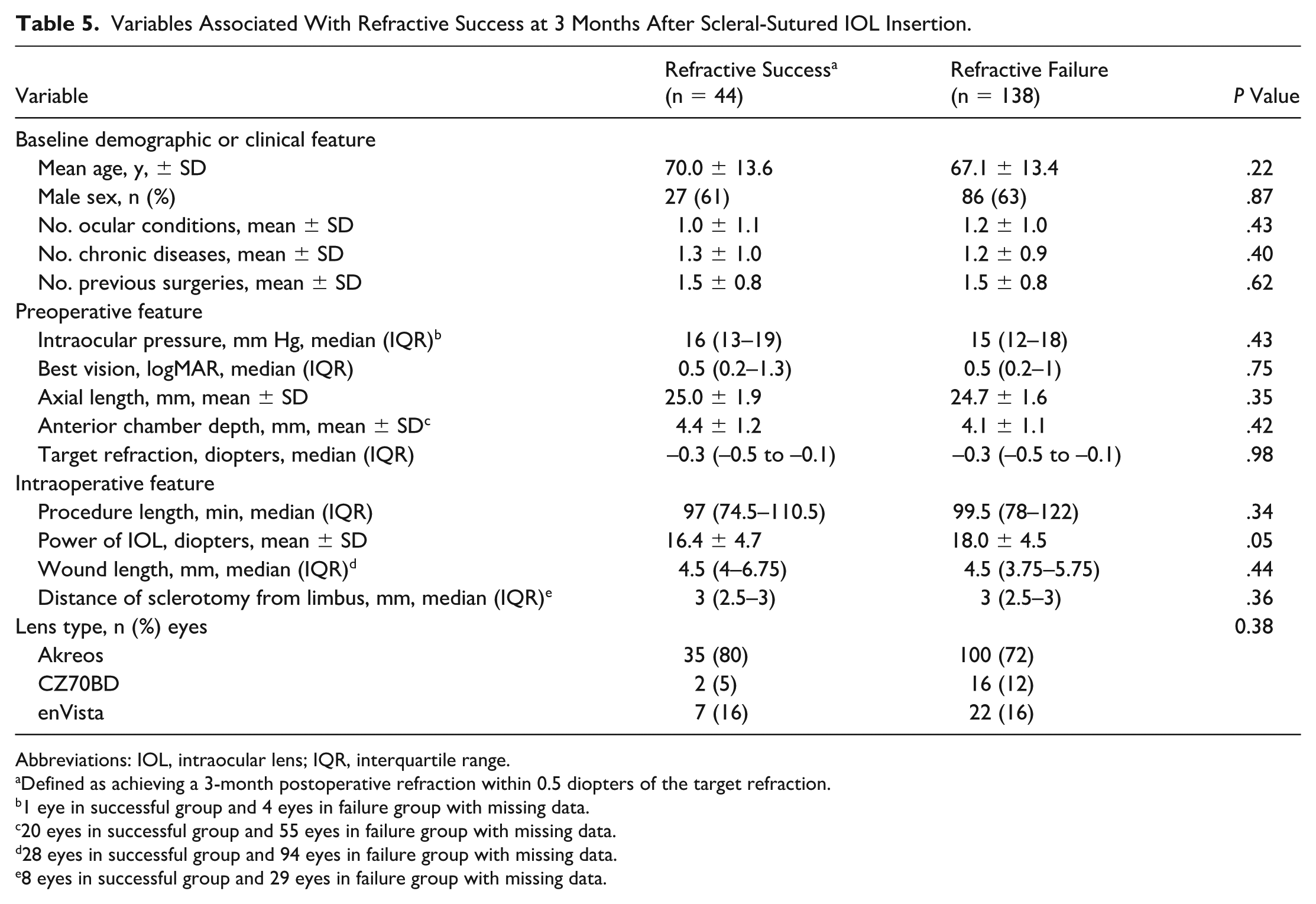
Forty-four (24%) of 182 eyes met the stringent refractive success criteria, showing a 3-month postoperative refraction within 0.5 diopters of the target refraction (Table 5).
Variables Associated With Refractive Success at 3 Months After Scleral-Sutured IOL Insertion.
Abbreviations: IOL, intraocular lens; IQR, interquartile range.
Defined as achieving a 3-month postoperative refraction within 0.5 diopters of the target refraction.
1 eye in successful group and 4 eyes in failure group with missing data.
20 eyes in successful group and 55 eyes in failure group with missing data.
28 eyes in successful group and 94 eyes in failure group with missing data.
8 eyes in successful group and 29 eyes in failure group with missing data.
The only variable associated with refractive success was implantation with a lower power IOL (mean IOL power, 16.4 diopters in the success group vs 18.0 diopters in the failure group; P = .05). Patient demographics, biometric data such as axial length, and intraoperative features such as the length of or distance of the sclerotomy from the limbus were not associated with postoperative refractive success. In analyses matching 88 eyes on IOL indication, a loss of statistical significance in these differences was observed, and covariate balance improved (Supplemental Table 6).
Multivariable logistic regression did not yield any significant associations between the 4 tested variables and odds of refractive success (Figure 3). In analyses matching eyes by IOL indication, results were not affected (Supplemental Table 7).
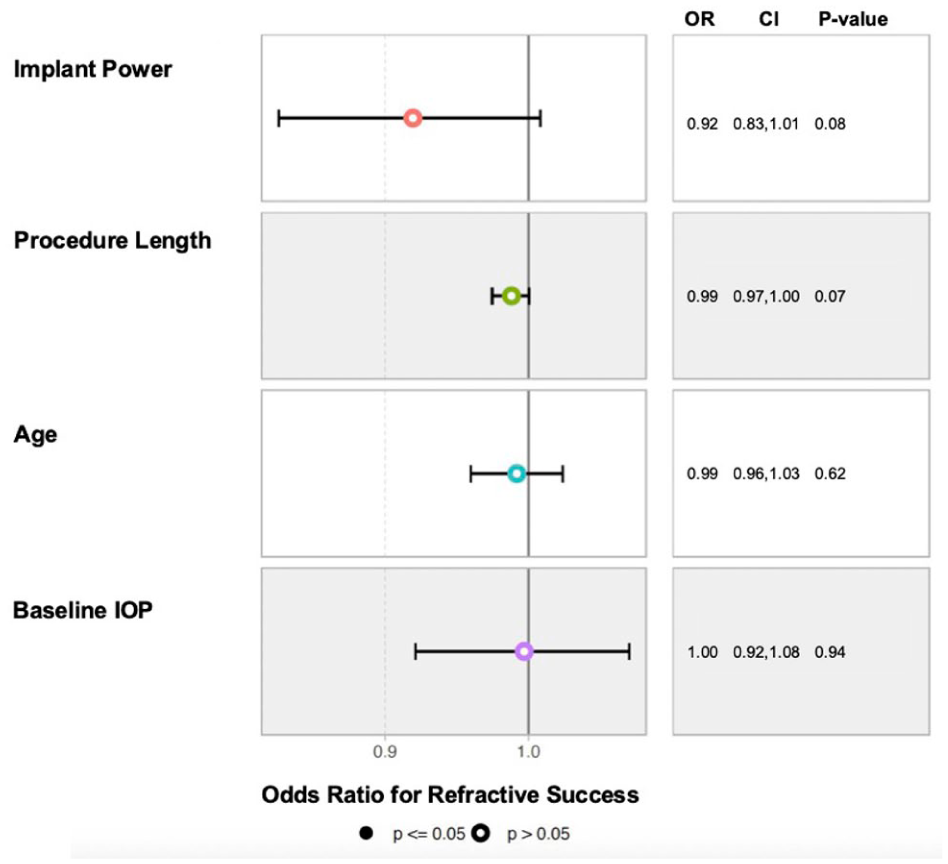
Forest plot depicting multivariable logistic regression analysis results for the 4 variables most associated with likelihood of refractive success (defined as improvement of ±0.5 diopters of the refractive target) at 3 months postoperatively in 182 eyes that received scleral-sutured intraocular lens implantation. Abbreviations: IOP, intraocular pressure; OR, odds ratio.
Scatter plots generated to characterize the relationship between the power of the IOL implant and absolute error from target refraction at 3 months after surgery showed a weak correlation (R = 0.3, P = .002) (Figure 4A), whereas scatter plots of the relationship between the distance of the sclerotomy from the limbus and absolute error from the target refraction at 3 months postoperatively showed a negligible correlation (R = 0, P = 1) (Figure 4B).
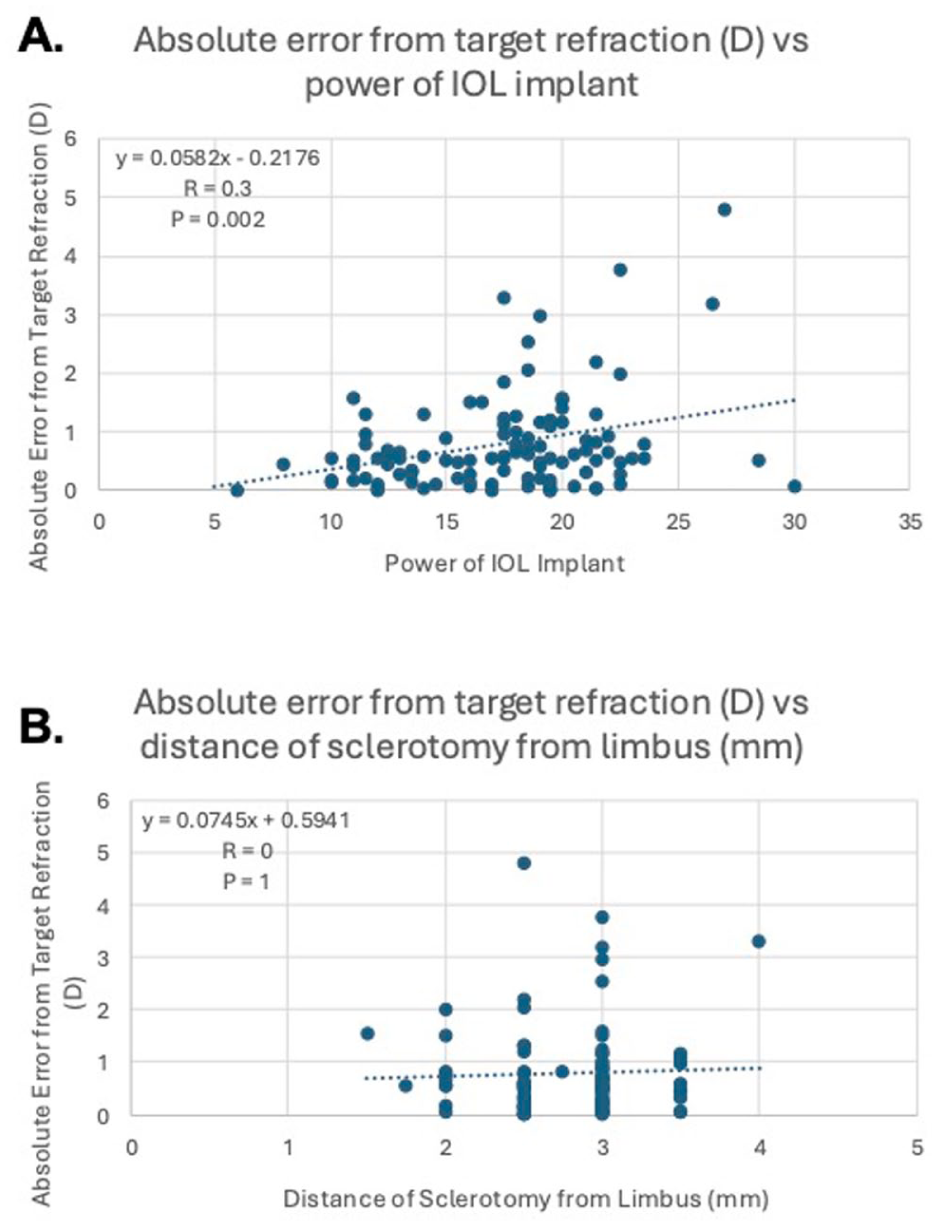
(A) Scatter plot demonstrating correlation between the power of the intraocular lens (IOL) implant (in diopters [D]) and the difference between target refraction and 3-month postoperative refraction (in diopters) in patients who received scleral-sutured IOL implantation. (B) Scatter plot demonstrating correlation between the distance of the sclerotomy from the limbus (in mm) and the difference between target refraction and 3-month postoperative refraction (in diopters). N = 182 eyes.
Conclusions
This retrospective cohort study evaluated 182 eyes at the Cole Eye Institute for variables associated with visual or refractive outcomes following a scleral-sutured IOL placement. We found that scleral-sutured IOL implantation was a safe procedure, resulting in a median complication rate of 0 at 3 months postoperatively (Table 3). This finding was likely influenced by the minimal number of comorbid conditions or prior surgical history in the majority of our patients. 25 However, even in the most recent large-scale retrospective analysis of alternative-site IOLs by Kaufmann et al, 26 patients with more complicated cataract surgical history (International Classification of Diseases, Tenth Revision codeet al H5902x) were more likely to have a scleral-sutured IOL implanted over an anterior chamber IOL, suggesting that the scleral-sutured IOL technique is still a safe technique in more complicated cases. Furthermore, Patel reported that, although each IOL technique is associated with a unique set of complications, the scleral-sutured IOL performed significantly better than other secondary IOLs in terms of rates of complications such as postoperative IOL tilt and dislocation. 14
Of note, this study was restricted to a 3-month postoperative follow-up period because of variable follow-up after this time point (median, 628 days, IQR, 333–1173 days). However, by the final follow-up visit, our dataset only included 3 cases of IOL subluxation or IOL tilt requiring repositioning at 687 to 2570 days after scleral-sutured IOL implantation. These data align with studies that report complications such as IOL tilt or decentration occurring at a higher frequency shortly after surgery, with this risk stabilizing over time. In studies by Chang et al 27 and Wendelstein et al, 28 the highest difference in IOL rotation was observed within 1 day and 1 week postoperatively. Pardini et al found that the scleral-sutured IOL position was stable at 1 to 6 months postoperatively, 29 further suggesting that the follow-up period within our study, though limited, can still be a reliable measure of complications affecting clinical success.
Our most robust analysis, the multivariable logistic regression, revealed that patients were more likely to achieve a VA of 20/40 or at least 3 Snellen lines of improvement by 3 months postoperatively if they had worse preoperative vision (OR, 3.92, 95% CI, 2.03–8.66; P < .001). It is possible that the vision success definition, particularly its clause regarding lines of improvement, has biased the analysis to favor success in patients with worse preoperative vision. Despite this limitation, the majority of our patients meeting the vision success criteria achieved it through attainment of a VA of 20/40 postoperatively, suggesting that implantation of an alternative-site IOL can lead to remarkable visual improvement. The literature acknowledges that worse preoperative BCVA is correlated with greater postoperative BCVA gain in various ophthalmic operations, including cataract surgery.30–33 This study further adds scleral-sutured IOL to the list of operations in agreement with this conclusion.
This study also demonstrated that patients with fewer preoperative ocular comorbidities had greater vision success by 3 months post–scleral-sutured IOL implantation (OR, 0.55, 95% CI, 0.37–0.78; P = .001 vs more preoperative ocular comorbidities). The association between fewer ocular conditions and vision success is supported by the literature as well.34–36 Glaucoma was the most burdensome comorbidity across all our cohorts. Glaucomatous change includes damaged retinal ganglion cells in the macula, which directly impacts VA, as it depends on the density of functioning retinal ganglion cells. 36 Other retinal processes can induce structural changes to the fovea, as in epiretinal membrane pathology, zonular or capsular weakness in the setting of pseudoexfoliation or prior trauma, or chronic inflammation seen in uveitis or diabetic retinopathy. These changes affect the integrity of the retina and optic nerve and limit VA despite correcting a patient’s refractive error.35,36 The optimal timing for IOL implantation in patients with ocular comorbidities remains controversial. A related area of future research may be in comparing the rates of BCVA success in patients with and those without these comorbidities to quantify the extent to which other ocular diagnoses affect the visual outcome potential after scleral-sutured IOL placement.
Analysis of lens type demonstrated that use of an Akreos AO60 lens was significantly associated with BCVA success compared with use of a CZ70BD lens. The Akreos AO60 lens has benefits of folding through a smaller incision with greater stability via 4-point fixation, although its hydrophilic material creates a drawback of opacifying in the setting of gas or silicone oil exposure. 37 The CZ70BD lens has its own benefits, including reduced suture-related strain and effective lens positioning error due to its eyelet location and large size, but it requires a larger incision with less stability via 2-point fixation. 37 Our additional analyses explored variables inherent to each lens cohort that may explain the variable performance of the lens brands but demonstrated no significant differences in preoperative BCVA and the number of chronic ocular comorbidities between groups. Similarly, although surgeon variability can be a confounder for visual outcomes, nearly 95% of the CZ70BD lens procedures were performed by surgeons who also implanted Akreos AO60 lenses, which suggests that surgeon variability is unlikely to be a confounding factor.
One hypothesis to potentially explain worse visual outcomes with the use of CZ70BD lenses compared with the use of Akreos AO60 lenses may be related to the higher reported incidence of significant IOL tilt and decentration in 2-point fixation compared with 4-point fixation.38–40 It is possible that the study eyes receiving a CZ70BD lens had mild tilt or decentration significant enough to cause functional astigmatism but not significant enough to be clinically noted as a postoperative complication. Alternatively, the CZ70BD lens may have introduced more astigmatism due to the larger wound necessitated for its placement or due to its spherical design that causes spherical aberrations. 37 Our findings are consistent with those of Khan et al, 41 who reported better postoperative VA in patients who received the Akreos AO60 lens (mean Snellen VA 20/63) compared with patients who received the CZ70BD lens (mean Snellen VA 20/112). Ultimately, however, this finding would benefit from further analysis with a larger sample and longer follow-up periods within each lens brand group.
With regard to achieving refractive success, we found that lower power IOLs were associated with increased likelihood of reaching within 0.5 diopters of the refractive target (mean IOL power, 16.4 diopters in the success group vs 18.0 diopters in the failure group). Importantly, this association was at the boundary of achieving statistical significance with unadjusted analysis and was not significant with adjusted or IOL indication–matched analysis, suggesting further study is necessary to strengthen findings. Nevertheless, achieving a maximally accurate refractive outcome is often a surgical goal.42–44 The literature to date delineates the effects of biometry, corneal shape change, and effective lens position on the accuracy of an IOL to its target refraction.44,45 Additionally, different IOL power calculators may be more accurate with a certain range of axial length and keratometry measurements.44,46,47 Although we did not specifically evaluate the performance of different IOL power calculators, it is possible that the methods used in our cohort performed better with lower IOL power. Future studies evaluating the accuracy of different power calculators stratified by IOL power for secondary lens implants may also help improve outcomes.
With regard to associations with biometric variables, to our knowledge, the most recent analysis of refractive success and axial length was in a study by Vounotrypidis et al 24 in which 6 scleral-sutured IOLs were evaluated for refractive success according to axial length; the authors found no correlation between these 2 variables. Our findings similarly corroborate that a patient’s axial length, which contributes to the IOL calculation, does not significantly impact refractive success. Furthermore, anterior chamber depth, which also is incorporated into the IOL calculation, was not found to significantly impact refractive success in our study.
Corneal changes are also implicated in affecting the accuracy of IOL calculations. Aramberri et al 45 reported that one of the sources of IOL calculation error stems from eyes that have undergone refractive surgery, as postoperative keratometry is an underestimation of the true biometric data. However, only 5 of 182 eyes in our study had a history of refractive surgery. Combined with the lack of relationship between biometric measurements and refractive success, it is unlikely that corneal refractive surgery could explain our findings.
Rather, the most likely hypothesis explaining our findings of a correlation between IOL power and refractive success is related to the effective lens position, an optimal parameter that serves as a proxy for the distance between the IOL and the cornea and one of the highest contributors to IOL calculation predictability error.48,49 Unlike conventional cataract surgery, secondary lens implants are subject to additional factors outside of the location of the capsular bag, which can influence final lens position. These factors, such as accurate sclerostomy placement and tension of fixation sutures, can cause small changes in the effective lens position that translate to a much greater impact on high-powered lenses. In a study using an IOL eye model, Gatinel et al 50 found that the same 0.1 mm effective lens position shift in a higher power IOL caused a larger refractive change (0.5 diopters) compared with the refractive change observed with a lower power IOL (0.07 diopters). This suggests that higher powered IOLs are more sensitive to small changes in effective lens position and thus can be less predictable in achieving target refraction than lower powered IOLs. 51 Figure 4A shows a weak but positive correlation between IOL implant power and the diopter difference between the target refraction and 3-month postoperative refraction, further corroborating that in the absence of significant analyses for biometry or corneal change, the effective lens position may be a causative factor in the contribution of lower power IOLs to refractive success.
This study is not without its limitations. Its retrospective nature introduces inherent biases, such as the selection bias created in excluding patients who underwent a concurrent ophthalmic procedure. This may limit the generalizability of the study and also undermine the true safety and efficacy profile of the scleral-sutured IOL in more complex cases. Furthermore, including pinhole measurements in the visual success definition may have inflated visual outcomes. However, this effect is likely minimal, as only 11 (6%) of 182 eyes demonstrated an improvement of >3 Snellen lines with pinhole. Additionally, a more stringent refractive target (within 0.25 diopters) was also analyzed but not reported, as the limited sample size (n = 29) prevented meaningful conclusions. Thus, we reported the most stringent refractive success criteria, consistent with recent literature on refractive error. 24 The inclusion of patients with ocular comorbidities and prior ophthalmic surgical history may have limited preoperative and postoperative visual and refractive potential, though our cohort is a more accurate representation of the eyes requiring a secondary IOL. Furthermore, ocular comorbidities were not further stratified by disease severity, which may have variably impacted outcomes.
Although this was a single-center study, multiple surgeons contributed to the dataset. Variables related to surgical technique may affect the outcomes in these patients. Furthermore, as scleral-sutured IOL candidacy and alternative-site IOL choice are surgeon dependent, our study cohort had varying baseline ocular complexity that can further affect visual and refractive outcomes. A related area of future study could compare ocular comorbidities, stratified by disease severity, and outcomes across different alternative-site IOLs. Another appropriate follow-up study might longitudinally document surgeon-specific preferences and techniques to control for surgical variability and its impacts on visual or refractive outcomes. Finally, our matched univariate analysis of refractive success demonstrated that IOL indication may be a confounder, emphasizing that this finding should be interpreted with caution and requires further study.
In conclusion, this study is, to our knowledge, one of the first to investigate patient and operative variables possibly associated with vision or refractive success with a scleral-sutured IOL. Our findings regarding preoperative vision, the number of preexisting ocular conditions, and type of IOL implanted being associated with surgical outcomes serve to guide clinical decision-making when determining whether a scleral-sutured IOL is the best match for a patient, as opposed to a different, alternative-site IOL. 52 Though IOL power is a potential predictor of refractive outcomes, further prospective study is needed to strengthen these findings. Possible clinical recommendations include consideration for how patient biometric measurements, refractive surgery history, and IOL power requirements can all factor into the postoperative refraction and guide a discussion of anticipated results with the patient. The findings from this study could help to guide provider–patient conversations regarding postoperative expectations with scleral-sutured IOL implants, which could enhance patient satisfaction and postoperative quality of life.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264261457976 – Supplemental material for Factors Influencing Visual and Refractive Outcomes for Scleral-Sutured Intraocular Lenses
Supplemental material, sj-docx-1-vrd-10.1177_24741264261457976 for Factors Influencing Visual and Refractive Outcomes for Scleral-Sutured Intraocular Lenses by Sonia B. Kim, Kevin C. Allan, Amy S. Nowacki, Neha Sharma, Alexis Braunrot, Akiva Eleff, Aleksandra Rachitskaya, Katherine Talcott, Alex Yuan and Leanne Clevenger in Journal of VitreoRetinal Diseases
Footnotes
Ethical Considerations
This study received ethical approval from the Cleveland Clinic Institutional Review Board (IRB approval no. 22-832) on August 7, 2022, and was deemed an exempt protocol. Patient data will not be shared with third parties.
Consent to Participate
This is an IRB-approved retrospective study, and all patient information was de-identified and patient consent not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Talcott received consulting fees from 4D Molecular Therapeutics, AbbVie, Alimera, Apellis, Astellas, Bausch + Lomb, EyePoint, Genentech, Harrow, Ocular Therapeutics, Outlook, Regeneron, and Zeiss; research fees from Regeneron and Zeiss; and speaking fees from Astellas, Genentech, and Zeiss. Dr. Rachitskaya received consulting fees from 4D Molecular Therapeutics, AbbVie/Allergan, Alcon, Apellis Pharmaceuticals, Astellas, Boehringer Ingelheim, Ethis, EyePoint, Lenz Therapeutics, Ocular Therapeutix, Regeneron, Roche/Genentech, Samsara, and Zeiss; received personal fees and served on the scientific advisory board for Samsara; received speaker fees from Apellis Pharmaceuticals, Astellas, Boehringer Ingelheim, Genentech, and Regeneron; and received research fees from 4D Molecular Therapeutics, Apellis Pharmaceuticals, Beacon Therapeutics, DRCR Retina Network, and Roche/Genentech. Dr. Clevenger received consulting fees from Alimera, Bausch + Lomb, Harrow, and Ocular Therapeutix; received institutional research patients from Regeneron.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.