
Abstract
Purpose:
To present a case series of patients who underwent pars plana vitrectomy (PPV) for dense vitreous hemorrhage (VH) secondary to avulsed retinal vessels in the setting of acute posterior vitreous detachment (PVD).
Methods:
The clinical presentation, surgical management, and outcomes of patients who underwent PPV for VH caused by avulsed retinal vessels were evaluated.
Results:
Four patients underwent PPV for dense VH. After evacuation of the VHs, all eyes were found to have avulsed retinal vessels without retinal tears.
Conclusions:
Dense VH in the setting of a PVD may preclude adequate examination of the fundus and require urgent PPV for timely management of possible retinal tears, retinal detachments, or avulsed retinal vessels. Retinal vessel avulsion without retinal tear is an uncommon but important cause of dense VH and may have favorable outcomes after vitrectomy.
Keywords
Introduction
Vitreous hemorrhage (VH) has numerous etiologies, one of the most common being posterior vitreous detachment (PVD). 1 PVDs involve complete separation of the hyaloid from the retina, including areas of strongest attachment at the optic nerve, macula, and retinal vessels. 2 Retinal tears associated with PVD carry a risk of progression to vision-threatening rhegmatogenous retinal detachment. In the setting of PVD-associated VH, there is a 50%–70% likelihood of concomitant retinal tear or retinal detachment.3,4
Inability to adequately examine the posterior segment in the setting of dense VH, or suspicion for retinal tear or detachment on B-scan ultrasonography, may necessitate urgent surgical intervention to rule out or treat potential rhegmatogenous pathology. While intraoperative examination of the peripheral retina during pars plana vitrectomy (PPV) often confirms the presence of retinal breaks, VH is not always associated with a full-thickness retinal defect. 5 This case series describes a relatively rare cause of VH in the setting of PVD: avulsion of retinal vessels in the absence of retinal tears.
Methods
Case Selection
This retrospective case series included 4 patients who were treated at the Retina Group of Washington. Patients were selected if they had a diagnosis of dense VH and underwent PPV, with intraoperative findings confirming retinal vessel avulsion without concomitant retinal tear or retinal detachment. Patients were included regardless of their preoperative PVD status. Dense VH was defined as a hemorrhage that was severe enough to preclude adequate visualization of the fundus. Patients were excluded if a retinal tear or detachment was observed on initial or subsequent evaluations or intraoperatively.
Data Collection
Clinical data between January 1, 2016, and December 31, 2025, were obtained through retrospective review of office visit and operative notes and included patient demographics, presenting symptoms, ocular history, best-corrected visual acuity (BCVA), initial examination findings, imaging findings, intraoperative procedures and details, and follow-up outcomes.
Ethical Considerations
This institutional review board-approved study was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a Health Insurance Portability and Accountability Act-compliant manner.
Cases
Case 1
A 65-year-old woman with a remote history of uncomplicated branch retinal vein occlusion (BRVO) presented with acute-onset floaters in the left eye. Five years before presentation, she had been diagnosed by a neuro-ophthalmologist with BRVO based on inferonasal optic nerve swelling and delayed arterial and venous filling of the inferior arcade on fluorescein angiography. BCVA was 20/20 OD and 20/70 OS. Intraocular pressure was 14 mm Hg OD and 12 mm Hg OS. Initial anterior segment examination demonstrated a posterior chamber intraocular lens (PCIOL) in the right eye and 2+ nuclear sclerotic cataract in the left eye and was otherwise unremarkable. Dilated fundus examination of the right eye revealed a nonvisually significant epiretinal membrane (ERM), whereas examination of the left eye demonstrated a hemorrhagic PVD with no evidence of retinal tear or retinal detachment.
The patient was followed closely and initially demonstrated partial resolution of the VH with improvement of BCVA to 20/60. However, 1 week after the initial presentation, she returned with a sudden worsening of vision in the left eye. BCVA of the left eye had declined to counting fingers (CF). Examination showed worsened VH with no view of the retina. B-scan ultrasonography demonstrated no definitive retinal tear or retinal detachment.
The patient underwent 25-gauge PPV in the affected left eye 3 days later. No retinal tears or retinal detachment were identified. A focally avulsed and lacerated retinal arteriole was visualized in the superonasal quadrant. Both ends of the arteriole were treated with endodiathermy, and the surrounding area was treated with endolaser photocoagulation.
On postoperative day (POD) 1, BCVA improved to 20/70 OS under partial air tamponade. At 2 years postoperatively, BCVA had improved to 20/20. Optical coherence tomography (OCT) of the macula demonstrated a normal foveal contour without evidence of an ERM.
Case 2
A 71-year-old man presented with a “pink veil” over the vision in his left eye for 2 weeks. BCVA was 20/25 OD and light perception in the left eye at initial evaluation. Intraocular pressure was 23 mm Hg OD and 16 mm Hg OS. Anterior segment examination demonstrated a mildly dislocated 3-piece sulcus intraocular lens in the right eye and a well-centered PCIOL in the left eye. Dilated fundus examination of the right eye was notable for 2 horseshoe retinal tears that had previously been well-treated with laser retinopexy, whereas examination of the left eye revealed dense VH with no view of the posterior segment. B-scan ultrasonography demonstrated a posteriorly tethered, partially mobile hyperreflective membrane that was concerning for rhegmatogenous retinal detachment. The affected left eye underwent 25-gauge PPV the next day.
After evacuation of the dense VH, a partial PVD was identified. No retinal detachment or retinal tear was observed; instead, an avulsed and lacerated retinal arteriole was identified and treated with endodiathermy. On POD 1, BCVA was CF under near-complete air tamponade. Final BCVA improved to 20/25 OS at 7 months postoperatively. Final OCT of the left eye demonstrated a normal foveal contour with a mild ERM.
Case 3
A 67-year-old man with a history of high myopia and laser-assisted in situ keratomileusis in both eyes presented with blurry vision and floaters in the right eye for 1 day. BCVA at presentation was hand motion in the right eye and 20/20 OS. Initial intraocular pressure was 15 mm Hg OU. Anterior segment examination demonstrated prior laser-assisted in situ keratomileusis flaps and well-centered multifocal PCIOLs in both eyes. Dilated fundus examination of the right eye showed dense VH with no view of the posterior segment. Dilated fundus examination of the left eye demonstrated peripapillary atrophy and was otherwise unremarkable. B-scan ultrasonography of the right eye (Figure 1) demonstrated a PVD without evidence of retinal tear or retinal detachment.
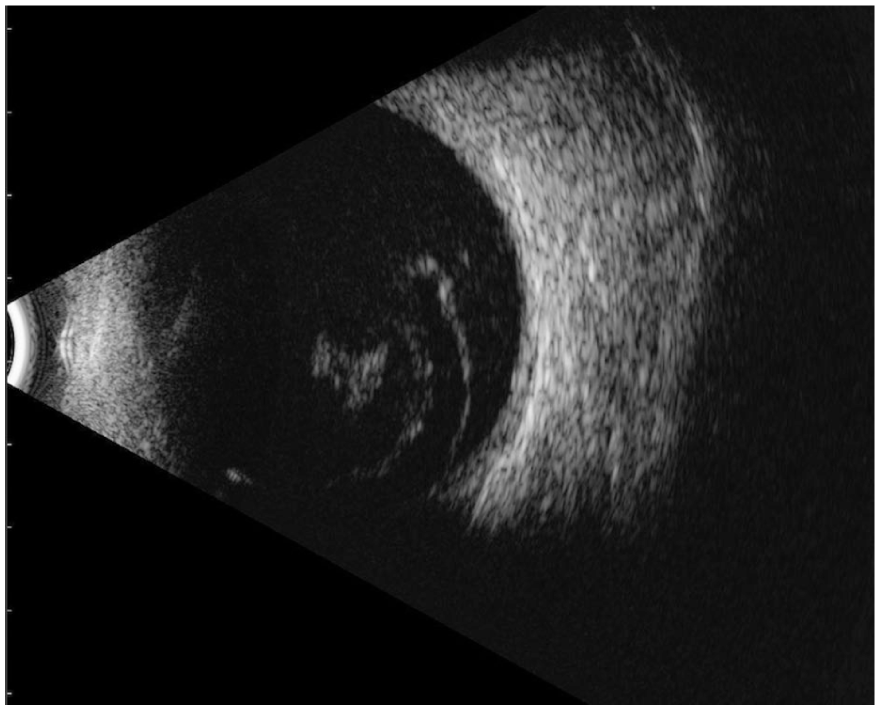
Preoperative B-scan ultrasonography image of the right eye in Case 3 demonstrating vitreous hemorrhage without evidence of retinal tear or retinal detachment.
Given the increased risk of retinal tears associated with high myopia and the inability to examine the fundus, the affected right eye underwent 25-gauge PPV 2 days later. After evacuation of the VH, a preexisting PVD was identified, along with an avulsed superonasal retinal vessel without a horseshoe tear. No further intraoperative treatment was performed. On POD 1, BCVA was CF under near-complete air tamponade, with final BCVA improving to 20/20 at 3 months postoperatively. OCT of the right eye at the final recorded follow-up demonstrated a mild ERM with a good foveal contour.
Case 4
A 74-year-old woman with a history of intermediate dry age-related macular degeneration in both eyes and a mild ERM in the right eye presented with 1 day of vision loss in the right eye. BCVA was CF in the right eye and 20/40 OS. Intraocular pressure was 21 mm Hg OD and 23 mm Hg OS. Anterior segment examination demonstrated well-centered PCIOLs in both eyes.
Dilated fundus examination of the right eye showed dense VH with no view of the retina. Examination of the left eye was notable for a PVD, macular drusen, and rare peripheral dot-blot hemorrhages consistent with mild hypertensive retinopathy. B-scan ultrasonography of the right eye revealed a PVD with no obvious retinal tear or retinal detachment.
The affected right eye underwent 25-gauge PPV 1 day later. After evacuation of the VH, a partial PVD was identified. An avulsed blood vessel without active bleeding was identified superotemporally. No intraoperative treatment was performed on the avulsed vessel, and no tamponade agent was used.
On POD 1, BCVA improved to 20/100, further improved to 20/20 by postoperative week 1, and stabilized at 20/25 at 13 months postoperatively. OCT of the right eye demonstrated a mild, stable ERM with preserved foveal contour, along with drusen, without any areas of chorioretinal atrophy or any signs of subretinal or intraretinal fluid.
Conclusions
The causes of VH are numerous and include proliferative diabetic retinopathy, retinal vascular occlusion, PVD, intraocular tumors, and various blood dyscrasias.6,7 PVD results from vitreous liquefaction and subsequent separation of the posterior hyaloid from the retinal surface. 8 During this process, adherent vitreous may exert traction on the peripheral retina, macula, optic disc, and retinal vasculature as it collapses anteriorly toward the vitreous base. 9 Acute PVDs are typically detected clinically when patients present with the sudden onset of floaters or flashing lights. 10 Studies have demonstrated a 7% to 12% risk of retinal tear in eyes with acute PVD, with the risk increasing to 50% to 70% in the presence of associated VH.3,4
PVD-associated VH due to avulsed retinal vessels was initially described by Robertson et al 11 in the context of round retinal breaks. De Brusio later expanded upon this finding to include avulsed retinal vessels with concomitant retinal tears or retinal detachment and termed the condition “avulsed retinal vessel syndrome.” 12 While PVD can lead to avulsed retinal vessels without associated retinal tears or retinal detachment, such cases are uncommon. A study of 65 cases of avulsed retinal vessels demonstrated a 12% occurrence of vessel avulsion without retinal tear. 6
Due to the high risk of retinal tear or retinal detachment in eyes with fundus-obscuring VH after vessel avulsion, B-scan ultrasonography is necessary to evaluate for concomitant rhegmatogenous pathology. Close follow-up is also prudent to allow for frequent serial examination as the hemorrhage clears. Although preoperative PVD status was known only in Case 1, either partial or complete PVD was identified intraoperatively in all 4 cases. Despite B-scan ultrasonography in Cases 1, 3, and 4 demonstrating VH without findings suggestive of retinal tear or retinal detachment, patients were advised to undergo vitrectomy owing to the density of hemorrhage and the risk of unidentified rhegmatogenous pathology.
Most cases reported in the literature have been diagnosed and treated in the office rather than in the operating room. Several in-office management strategies for avulsed retinal vessels have been evaluated in the past and have been found to be largely unsuccessful. Early reports describing medical management with cryotherapy, ruby laser, and xenon arc photocoagulation demonstrated limited success in preventing recurrent VH.5,11 Reports on argon laser photocoagulation, 13 Nd:Yag laser release of vitreous traction, 14 and scleral buckling5,11,15 have described variable success in preventing recurrent VH.
More recent literature has suggested the need for surgical management with vitrectomy to effectively relieve vitreous traction on avulsed retinal vessels. For example, Cruzado-Sanchez et al 16 described a case of an avulsed retinal vessel that was unsuccessfully treated in the office with repeated argon laser photocoagulation and ultimately required vitrectomy after recurrence of VH. Washio and Tsuchida similarly described the surgical management of 2 patients who underwent PPV, with or without vascular coagulation, without postoperative recurrence of VH. 17
All patients in this case series presented with dense VH. Although B-scan ultrasonography performed in the office did not demonstrate retinal tears or retinal detachments, PPV was deemed necessary to rule out rhegmatogenous pathology (Table 1). Thorough vitrectomy may also relieve persistent vitreous traction on the causative avulsed retinal vessel. The use of endodiathermy was variable among the cases, suggesting that simply releasing vitreous traction alone, without vessel coagulation, may be sufficient in some cases. Patients in Cases 3 and 4 underwent PPV without endodiathermy, and neither patient developed recurrent hemorrhage during long-term follow-up. If the causative avulsed vessel appears to have achieved hemostasis by the time of surgery, or if the vessel is avulsed from the retinal surface without full-thickness rupture, observation without cauterization may be considered.
Preoperative Presentation With Associated Surgical Management and Postoperative Outcomes.
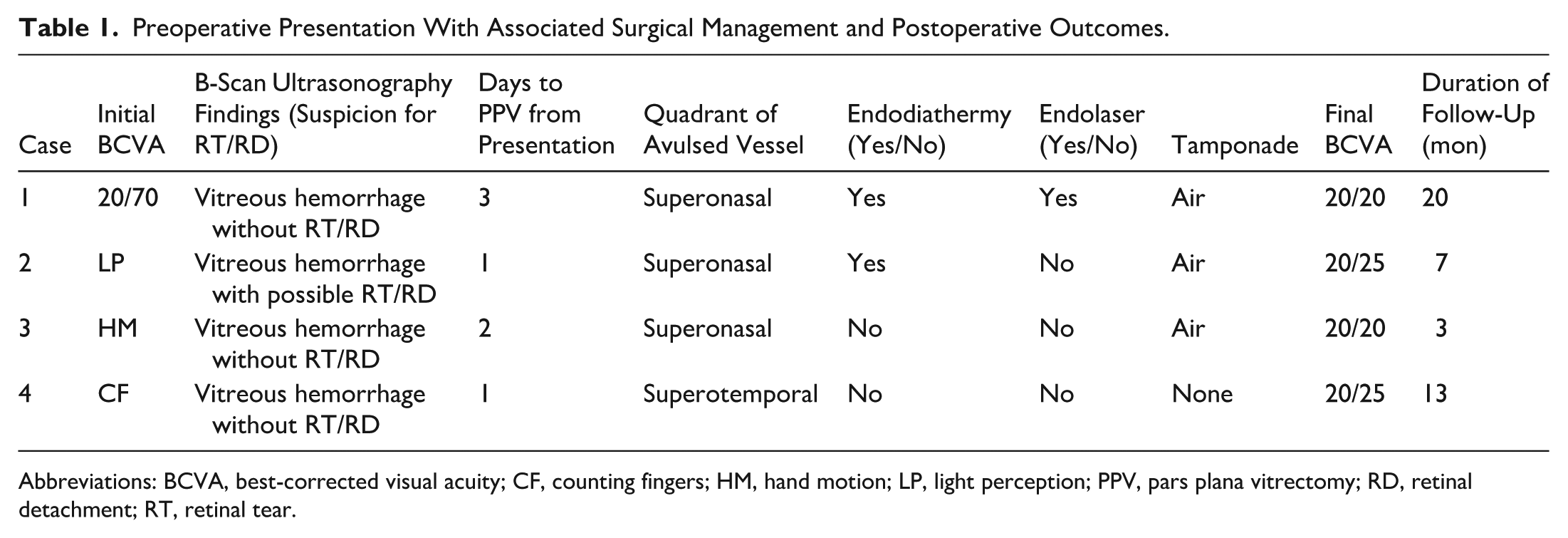
Abbreviations: BCVA, best-corrected visual acuity; CF, counting fingers; HM, hand motion; LP, light perception; PPV, pars plana vitrectomy; RD, retinal detachment; RT, retinal tear.
Although none of the patients in our series who received endodiathermy developed complications related to vessel cauterization, retinal vein occlusion with subsequent cystoid macular edema has previously been reported following coagulation of the avulsed retinal vessel. 17 Therefore, we recommend that the decision to use endodiathermy, as well as the degree of vessel cauterization, should be individualized on a case-by-case basis.
The use of intraocular tamponade also varied among cases. In the absence of retinal tears or retinal detachment, no tamponade or short-term air tamponade may be sufficient. In 3 of the 4 cases, a complete or partial air–fluid exchange was performed to facilitate closure of sclerotomies and prevent postoperative hypotony. 18 Longer-acting gas tamponade was deemed unnecessary in all 4 cases, as no full-thickness retinal breaks or retinal detachment requiring longer-term tamponade were identified. None of the patients in this case series developed recurrent VH, and despite the severity of visual loss at presentation, all patients achieved excellent long-term visual outcomes after vitrectomy.
In conclusion, we present 4 cases of dense VH secondary to avulsed retinal vessels without a concomitant retinal tear or retinal detachment. This clinical entity is an uncommon cause of VH that should be considered in the differential diagnosis of acute vision loss in the setting of PVD. Early surgical intervention should be considered when dense VH obscures visualization of the fundus to assess for possible retinal tears, retinal detachment, or, as highlighted in this case series, retinal vessel avulsion syndrome. Intraoperative management includes thorough vitrectomy to relieve all traction on the avulsed vessel and vessel coagulation to prevent recurrent hemorrhage in select cases.
Footnotes
Ethical Considerations
This institutional review board-approved retrospective case series was conducted within the PRISM Vision Group and the Retina Group of Washington in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information were performed in a Health Insurance Portability and Accountability Act-compliant manner.
Consent to Participate
Informed consent was obtained from all patients before participation in the study.
Consent for Publication
Informed consent for publication, including permission for the use of all photographs and images, was obtained from all patients before the procedures.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.