
Abstract
Introduction
Retinoblastoma is the most common primary intraocular malignancy in childhood and is managed using a multimodal approach that may include intravenous chemotherapy, intra-arterial chemotherapy, and focal consolidation therapies such as laser photocoagulation and cryotherapy. While systemic and intra-arterial chemotherapy constitute the backbone of treatment for many patients, selected cases may be controlled with focal therapies alone, depending on disease extent and location. These approaches have significantly improved globe salvage rates, particularly in early-stage disease. However, recurrent retinal tumors after initial remission remain a significant therapeutic challenge. These tumors may be resistant to additional systemic therapy, necessitating localized intraocular treatment strategies. 1
The introduction of intravitreal (IVT) chemotherapy, particularly melphalan, revolutionized the management of vitreous seeding in retinoblastoma. Although administered intravitreally, the drug distributes throughout the vitreous cavity, providing whole-eye exposure rather than lesion-directed treatment. Both melphalan and topotecan have been used as IVT agents in clinical practice. Although melphalan has been widely adopted, concerns regarding retinal and retinal pigment epithelium toxicity, especially with higher cumulative exposure, have sustained interest in alternative drugs and dosing strategies. Topotecan, a topoisomerase I inhibitor with potent antitumor activity and a favorable pharmacokinetic profile, has been administered via multiple routes (systemic, periocular, and IVT). Studies suggest that IVT topotecan can achieve high intraocular drug exposure while maintaining a generally favorable safety profile.2–5
Preclinical studies by Del Sole et al demonstrated that high-dose IVT topotecan (up to 50 µg in rabbits, approximately equivalent to a 100 µg human dose) was associated with preserved retinal function and no significant histopathologic retinal damage in rabbit eyes. These findings provided the pharmacologic rationale for clinical dose escalation in eyes with recurrent disease.5–8
More recently, Abramson et al 9 reported preliminary clinical success using high-dose IVT topotecan (90 µg) combined with focal laser consolidation in eyes with recurrent solid retinal tumors, without significant ocular toxicity. While higher doses of IVT topotecan have also been explored in the context of vitreous and subretinal seeding, evidence specifically addressing solid retinal tumors remains limited. Subsequently, Shields et al described a series of 13 eyes with recurrent retinoblastoma, including 3 with isolated solid retinal tumors, treated with high-dose IVT topotecan (90–100 µg). Tumor regression was observed in 92% of the eyes, with globe salvage in 100%, and without major complications. 10
Based on this preliminary experience and supporting preclinical evidence, we aimed to evaluate the tumor control efficacy and ocular safety of high-dose IVT topotecan as a salvage option for isolated recurrent solid retinal tumors in retinoblastoma at a tertiary referral center.
Methods
Study Design and Setting
This retrospective case series was based on a prospectively maintained clinical database from the Retinoblastoma Program at Hospital de Pediatría “Prof. Dr. Juan P. Garrahan,” Buenos Aires, Argentina, and included patients treated between June 2023 and June 2025. All treatments were administered as part of routine clinical care according to institutional practice guidelines. Clinical data were recorded contemporaneously in the database and later analyzed retrospectively.
The study was approved by the Institutional Review Board/Ethics Committee of Hospital de Pediatría “Prof. Dr. Juan P. Garrahan.” Written informed consent for treatment was obtained from the parents or legal guardians of the patients. The Ethics Committee granted a waiver of additional informed consent for the retrospective analysis of de-identified clinical data.
Patients and Eligibility
A total of 10 eyes from 10 patients previously treated for intraocular retinoblastoma that subsequently developed isolated recurrent solid retinal tumors were included. Inclusion criteria were as follows: (1) documented recurrence of a solid retinal tumor after a period of clinical inactivity; (2) prior treatment with systemic and/or intra-arterial chemotherapy; and (3) treatment with high-dose, IVT topotecan (100 µg/0.1 mL). Tumor size and location at recurrence were documented, with the largest basal diameter recorded in disc diameters and/or millimeters. Adjunctive focal consolidation therapy, including laser photocoagulation and/or cryotherapy, was performed at the discretion of the treating physician based on tumor location and clinical characteristics.
Exclusion Criteria
Eyes with active vitreous or subretinal seeding at the time of recurrence requiring alternative IVT agents, anterior segment involvement, suspected ciliary body disease, suspected extraocular extension, media opacity precluding adequate assessment, or inability to adhere to the follow-up regimen were excluded. Ultrasound biomicroscopy was performed when clinically indicated to assess anterior segment and ciliary body involvement before IVT injection.
Intravitreal Injection Protocol
All procedures were performed in the operating room under general anesthesia. After placement of a lid speculum and antisepsis with 5% povidone-iodine, a 32-gauge needle was introduced through the pars plana at an age-adjusted distance from the limbus, avoiding tumor zones. Topotecan was prepared from commercially available formulations and diluted under sterile conditions to achieve a final dose of 100 µg/0.1 mL, which was injected intravitreally. No anterior chamber paracentesis (“aqueous tap”) was performed, and no preinjection globe-softening maneuvers (eg, digital massage) were routinely performed.
Indirect ophthalmoscopy was performed immediately before and after injection. Upon needle withdrawal, triple freeze–thaw cryotherapy was applied at the injection site using an external cryoprobe. Adjunctive focal consolidation therapy, including laser photocoagulation and/or cryotherapy, was administered during the same session as the IVT injection or during subsequent sessions, depending on tumor response and location. Treatments were repeated at 4-week intervals until complete clinical regression of the recurrent solid tumor was documented. No additional IVT topotecan injections or consolidation treatments were administered after complete tumor regression was achieved.
Follow-Up Regimen and Definitions
Follow-up examinations under anesthesia (EUAs) included RetCam imaging and indirect ophthalmoscopy and were performed at baseline to document recurrence, during treatment, and after completion of IVT chemotherapy. EUAs were scheduled every 4 weeks during active treatment and every 4 to 8 weeks thereafter according to institutional practice. Optical coherence tomography (OCT) was not routinely performed, and assessment of retinal toxicity was based on clinical examination and imaging findings. Tumor response was assessed clinically and documented at each EUA. Complete regression (complete response) was defined as the disappearance of a clinically active tumor at the recurrence site on EUA and RetCam imaging, with conversion to an inactive regressed scar and no evidence of residual viable tumor.
Outcome Measures
Primary outcomes included complete tumor regression, globe salvage, ocular toxicity, and the occurrence of systemic adverse events or metastatic disease. Secondary outcomes included the number of IVT injections required to achieve complete regression and the need for adjunct focal consolidation therapy.
Statistical Analysis
Descriptive statistics were used for data analysis. Continuous variables are reported as mean ± SD or median (range), as appropriate, and categorical variables as counts and percentages.
Results
A total of 10 eyes from 10 patients with recurrent or new retinal solid tumors were treated with high-dose IVT topotecan (100 µg per injection), administered in combination with focal laser photocoagulation (10/10 eyes) and cryotherapy (2/10 eyes). The mean age at initial retinoblastoma diagnosis was 7 (range, 1–24) months, whereas the mean age at diagnosis of recurrent retinal tumor was 4 (range, 1–7) years. Overall, 70% of patients were men (7/10) and 30% were (3/10). Retinoblastoma was bilateral in 9 out of 10 patients, and 4 out of 10 cases involved a single remaining eye. According to the International Classification of Retinoblastoma at initial diagnosis, 2 eyes were classified as Group B, 6 eyes as Group C, and 2 eyes as Group D.
All tumors treated in this study were solid retinal lesions without associated vitreous or subretinal seeding, and no evidence of extraocular dissemination was observed. Recurrent tumors arose adjacent to previous scar lesions in 8 eyes, whereas in 2 eyes, the lesions developed in a retinal topography different from that of the original tumors. Recurrences occurred after initial tumor control had been achieved with prior treatment consisting of systemic intravenous chemotherapy followed by intra-arterial chemotherapy in 4 patients, or intra-arterial chemotherapy alone in 6 patients. The mean interval between the last prior treatment and detection of recurrence on EUA with RetCam imaging (“delta time”) was 13 (range, 3–24) months (Table 1). At the time of recurrence, no patient demonstrated clinical evidence of extraocular disease. Tumor characteristics at recurrence are summarized in Table 1.
Clinical Characteristics and Outcomes of 10 Eyes Treated With High-Dose Intravitreal Topotecan (100 µg) and Focal Consolidation Therapy.
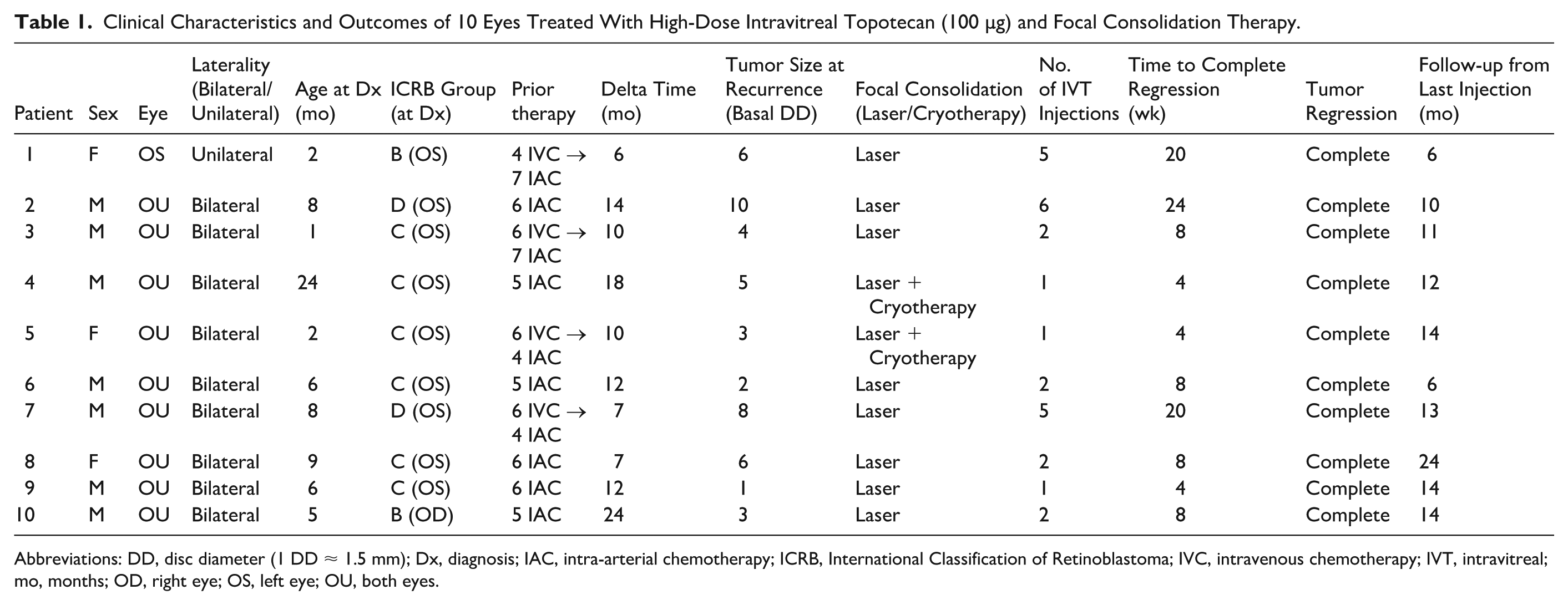
Abbreviations: DD, disc diameter (1 DD ≈ 1.5 mm); Dx, diagnosis; IAC, intra-arterial chemotherapy; ICRB, International Classification of Retinoblastoma; IVC, intravenous chemotherapy; IVT, intravitreal; mo, months; OD, right eye; OS, left eye; OU, both eyes.
Each eye received IVT topotecan at a fixed dose of 100 µg per injection. The median number of injections per eye was 2 (range, 1–6), with a mean of 3 injections per eye. Injections were administered at approximately 4-week intervals according to the planned treatment schedule. Overall, a total of 27 IVT injections were administered. IVT topotecan was administered as part of a combined treatment approach with adjunctive laser photocoagulation and/or cryotherapy, as described in the Methods section. No protocol deviations in dose or injection interval were recorded.
Complete tumor regression was achieved in all 10 eyes (100%), with no evidence of tumor persistence on fundus examination after completion of treatment (Figure 1). No eyes required enucleation, and there were no cases of metastatic disease or death. Over a mean follow-up of 12 (range, 6–24) months, no ocular or systemic adverse events related to treatment were observed. Specifically, there were no clinically evident cases of anterior segment inflammation, retinal hemorrhage, retinal pigment epithelium toxicity, retinal detachment, or optic nerve atrophy on serial EUA or RetCam imaging. All eyes maintained complete tumor control, with no post-treatment recurrences observed, and no additional IVT chemotherapy was required beyond the planned treatment course. No late-onset complications were observed during the available follow-up period.
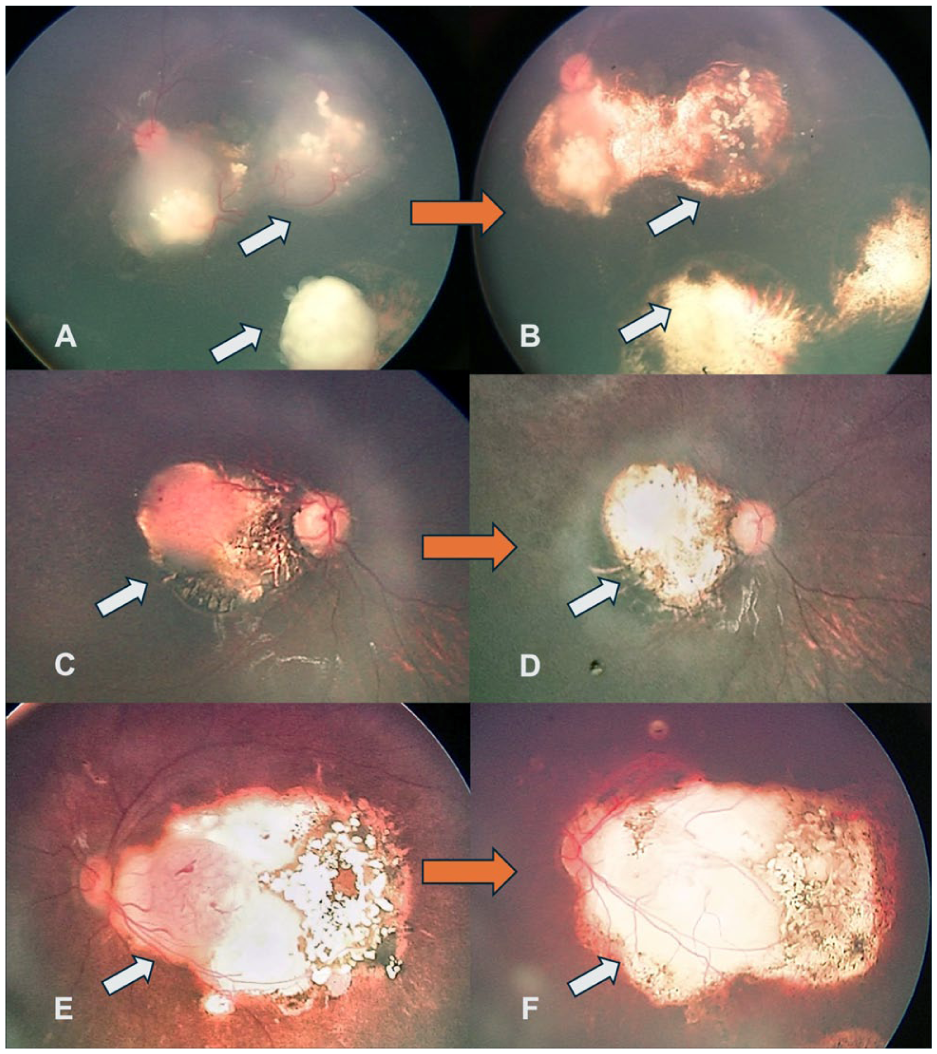
RetCam images obtained before treatment (left panels: A, C, and E) and after treatment (right panels: B, D, and F) with intravitreal topotecan (100 µg) in 3 patients with recurrent solid retinal tumors. White arrows highlight the retinal tumor in each case before and after treatment.
Conclusions
High-dose IVT topotecan seems a promising treatment option for isolated recurrent solid retinal tumors in retinoblastoma, achieving excellent tumor control with a low observed risk of toxicity in the short-to-medium term. Although IVT melphalan has historically been widely used for the treatment of vitreous seeding, and topotecan is increasingly being used as a first-line IVT agent in many centers, concerns regarding melphalan-associated retinal toxicity, particularly at higher cumulative doses, have supported continued exploration of alternative IVT agents and dosing strategies.2–4,6
Topotecan, a topoisomerase I inhibitor, has shown favorable pharmacokinetic and safety characteristics in both preclinical and clinical settings. In rabbit models, IVT topotecan doses of up to 50 µg (approximately corresponding to 100 µg in the human eye based on interspecies differences in vitreous volume) were associated with preserved electroretinographic responses and no significant histopathologic retinal damage.5,7,8 These experimental data provided the rationale for cautious clinical dose escalation in eyes with recurrent intraocular disease.
Initial clinical experience with high-dose IVT topotecan was reported by Abramson et al, 9 who described tumor regression using a 90 µg dose administered in conjunction with focal laser consolidation in 3 eyes, without reported systemic toxicity or major ocular complications. More recently, Shields et al reported outcomes in 13 eyes treated with 90 to 100 µg IVT topotecan combined with laser photocoagulation and/or cryotherapy; 3 eyes had solid retinal tumors as the only manifestation of recurrence. Complete response was achieved in 92% of cases, with globe salvage in 100%, and no cases of retinopathy or extraocular extension were reported. 10
Despite these encouraging reports, there remains limited evidence specifically addressing the role of high-dose IVT topotecan for solid retinal tumor recurrence without vitreous or subretinal seeding, representing a biologically and anatomically distinct therapeutic scenario. Our study focused exclusively on isolated recurrent solid retinal tumors, most of which were associated with previous scar sites, as well as new solid tumors arising in different retinal locations, treated with 100 µg IVT topotecan in combination with focal consolidation therapy.
In this cohort, complete tumor regression was achieved in all treated eyes, with no enucleations and no requirement for additional systemic rescue therapy. During a mean follow-up period of 12 (range, 6–24) months, no ocular or systemic adverse events related to treatment were observed. Notably, OCT was not routinely performed in all patients. Therefore, while no clinically appreciable retinal toxicity was detected, subtle structural retinal changes could have been missed, representing a limitation of the present study. A longer follow-up will be important to better define the durability of tumor control and the potential for late-onset toxicity, particularly in patients with shorter follow-up durations.
Although the 2 eyes requiring the highest number of IVT injections were originally classified as International Classification of Retinoblastoma Group D at diagnosis, the initial classification may be less informative for recurrence management than the characteristics of the recurrent lesion itself. Although no formal statistical analysis was performed due to the limited sample size, larger recurrent tumors tended to require a higher number of IVT injections and a longer time to achieve complete regression. Future studies should evaluate whether the size and thickness of recurrent solid retinal tumors correlate more directly with treatment burden and duration.
From a clinical perspective, achieving globe salvage in eyes with isolated recurrent solid retinal tumors supports the concept that IVT chemotherapy may have a therapeutic role beyond the management of vitreous disease, particularly in cases in which intra-arterial chemotherapy is not feasible or has been previously exhausted. 11 As IVT chemotherapy is technically feasible and can be implemented in centers with established retinoblastoma expertise, this approach may be relevant in regions with limited access to intra-arterial chemotherapy. As topotecan becomes more widely available and its safety profile is further characterized, high-dose IVT treatment regimens may contribute to reducing enucleation rates in selected cases, including in resource-constrained environments; however, broader validation in larger cohorts and with longer follow-up durations is required before generalizing these findings across diverse clinical practice environments.
Nonetheless, several limitations of our study should be acknowledged, including its retrospective design, small sample size, and relatively short follow-up duration. Therefore, conclusions regarding long-term safety, including cumulative retinal toxicity, visual outcomes, and late adverse effects, cannot be definitively established. Future multicenter studies with standardized imaging protocols, including routine OCT when feasible, longer follow-up periods, and larger patient cohorts, are needed to validate these findings and to better define optimal indications, dosing regimens, and combination treatment strategies for IVT topotecan in recurrent solid retinal tumors.
In summary, high-dose IVT topotecan (100 µg), combined with laser photocoagulation and/or cryotherapy, appears to be a promising salvage treatment option for isolated recurrent solid retinal tumors in retinoblastoma, achieving excellent tumor control with a low observed risk of toxicity during the available follow-up period. This approach may be considered in selected cases and warrants further evaluation in larger cohorts with longer follow-up and standardized imaging protocols.
Footnotes
Ethical Considerations
This retrospective case series adhered to the tenets of the Declaration of Helsinki. The Institutional Review Board of Hospital J.P. Garrahan reviewed and approved the protocol.
Consent to Participate
Informed consent for participation was obtained in accordance with the applicable institutional guidelines and regulations.
Consent for Publication
Informed consent for publication of all photographs and images was obtained in accordance with the applicable institutional guidelines and regulations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.