
Abstract
Purpose:
To describe the optical coherence tomography (OCT) features of retinal leukemic infiltrates and determine their association with visual and systemic prognosis in leukemic retinopathy.
Methods:
A retrospective, cross-sectional multicenter study was conducted on patients diagnosed with leukemia from January 2016 to December 2024 who had OCT imaging at presentation. Demographic, clinical, and OCT data were reviewed. Univariate and multivariate regression analyses were performed to identify OCT biomarkers associated with poor visual and systemic outcomes.
Results:
Seventy-seven eyes of 47 patients (mean age, 41.7 ± 21.75 years; 83% male) were included. Bilateral involvement was present in 70% of patients. Acute lymphocytic leukemia was the most common subtype (53%), followed by chronic myeloid leukemia (25%). Leukemic infiltrates were identified in 39% of eyes, most frequently within the inner retinal layers (70%), with preservation of the retinal pigment epithelium. On univariate regression, cystoid macular edema (CME) (odds ratio [OR], 0.114; 95% CI, 0.014-0.932; P = .043) and ellipsoid zone (EZ) loss (OR, 3.882; 95% CI, 1.289-11.692; P = .016) were significantly associated with visual outcome. Multivariate regression confirmed CME (OR, 0.022; 95% CI, 0.008-0.687; P = .022) and EZ loss (OR, 5.598; 95% CI, 1.571-19.943; P = .008) as independent predictors of poor vision. Infiltrate location, size, and configuration were not associated with visual prognosis.
Conclusions:
Retinal leukemic infiltrates predominantly involve the inner retinal layers. CME and disruption of the EZ are key OCT biomarkers predictive of poor visual outcome, irrespective of leukemia subtype or infiltrate morphology.
Keywords
Introduction
With an average incidence of approximately 50% for ocular manifestation in hematologic disorders, leukemic infiltrates have been reported in 6% to 10% of cases.1,2 Retinal leukemic infiltrates are characterized by yellowish-white lesions that may be subtle on clinical examination. Although they can be associated with surrounding hemorrhage or perivascular sheathing, they are independent entities during resolution. These infiltrates can be as small as 100 to 250 µm in diameter and generally lack back shadowing (posterior signal attenuation) on optical coherence tomography (OCT) imaging behind the infiltrate. The loss of the figure-of-8 configuration of retinal blood vessels on cross-sectional OCT due to the impedance of intraluminal blood flow and separate inner and outer hyperreflective lesions related to intraretinal hemorrhages and retinal infiltrates are 2 important features of leukemic infiltrates described on OCT.3,4
Certain OCT features in the literature have also been suggested as presenting features in leukemia.2,4–12 Neurosensory detachment can present early in cases of acute lymphocytic leukemia (ALL) due to leukemic infiltration of choroidal vessels, subsequently leading to stagnation of blood due to external compression or hyperviscosity. Further ischemia of the retinal pigment epithelium (RPE)–Bruch complex leads to disruption of the outer blood retinal barrier and, eventually, accumulation of choroidal fluid in the subretinal space. 13 Previous reports also suggest the incidence of sub-inner limiting membrane (ILM) bleeds on OCT in cases of acute promyelocytic leukemia after initiation of chemotherapy. 14 Extended depth imaging OCT and laser speckle flowgraphy helped to show increased choroidal thickness and presence of leukemic cells largely at the posterior choroid, supporting the histopathologic description provided by Leonardy et al.15–17 The thickness of the ganglion cell–inner limiting membrane (GC-IPL) in patients with leukemia is more than the normal population and negatively correlated with platelet levels. This is secondary to acute ischemia dye to axoplasmic flow stasis and inflammatory axonal swelling. 18 It has also been noted that the vascular density of the superficial and deep capillary plexus in patients with leukemia is particularly increased due to increased blood viscosity.10,19,20
Despite these insights, the nature and morphologic characteristics of retinal leukemic infiltrates need to be understood. To our knowledge, this is the first study to comprehensively describe the OCT features of retinal infiltrates in leukemic retinopathy and evaluate their correlation with both visual and systemic prognosis.
Methods
This retrospective, multicenter, cross-sectional study was conducted at the Centre of Excellence in Southeast Asia. The study included patients of all ages and sexes diagnosed with any stage of leukemia from January 2016 to December 2024 (as per the available electronic medical record database) with documented OCT at the first visit, regardless of whether the patient presented with acute or chronic leukemia. All patients with inconclusive diagnoses or incomplete records were excluded. The institutional review board approved the study (LEC-BHR-R-03-24-456), which adhered to the tenets of the Declaration of Helsinki.
Collected data included patients’ demographic profile (age, sex, leukemia type, and laterality of the affected eye), presenting symptom and best-corrected visual acuity (BCVA) in logMAR at presentation and at last follow-up. The OCT macula findings (Cirrus HD-OCT, Carl Zeiss Meditec; Topcon, Topcon Medical Systems; Spectralis, Heidelberg Engineering) included changes at the vitreoretinal interface, presence or absence of leukemic infiltrates, characteristics of leukemic infiltrates, size of leukemic infiltrates, presence or absence of back shadowing, and macular findings (Table 1) (Figures 1 and 2). A single investigator reviewed all OCT images, and discrepancies were resolved by consulting the senior ophthalmologist.
Comparative Difference of OCT Features in Various Forms of Leukemia and Their Correlation With Visual Acuity.
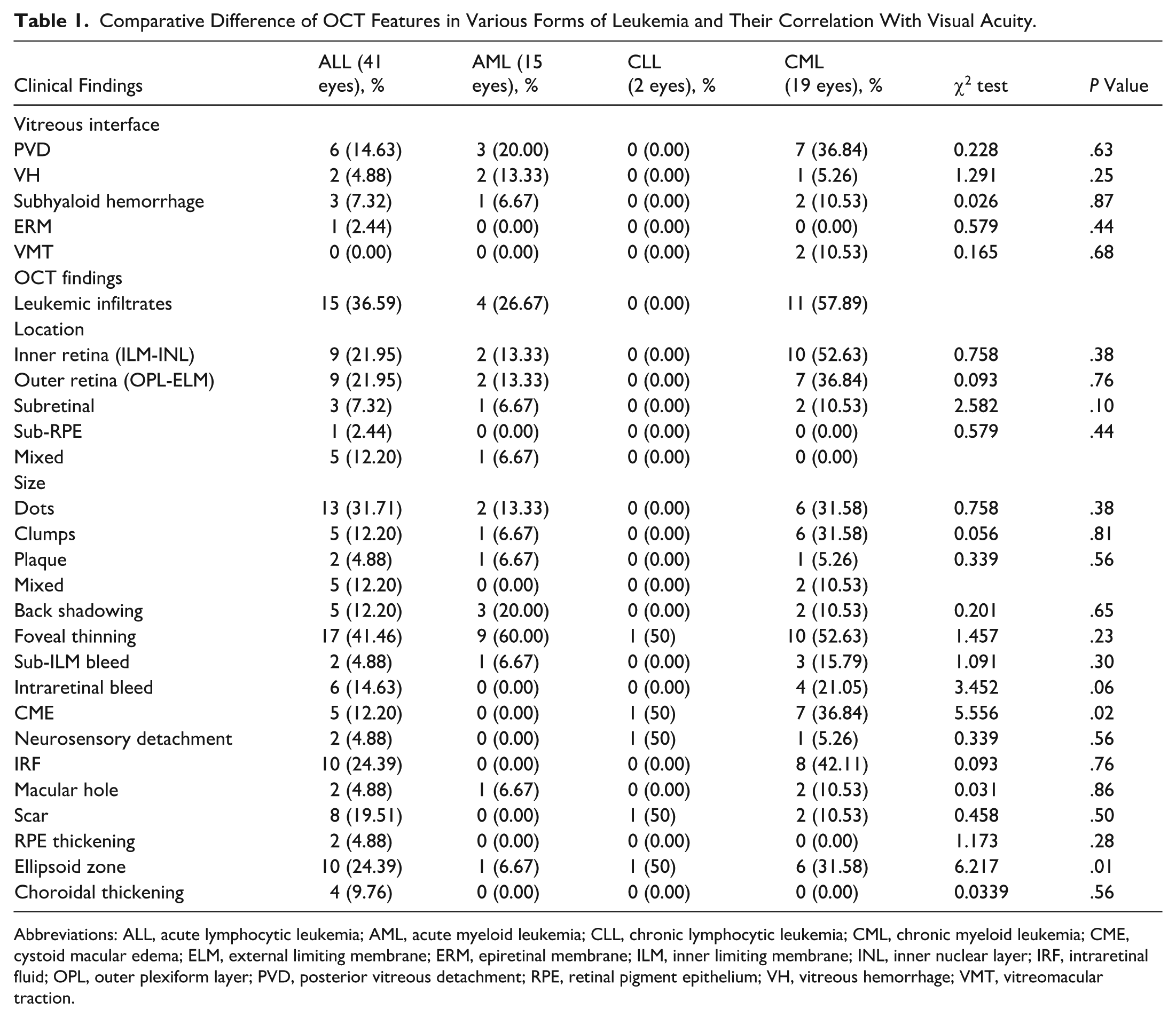
Abbreviations: ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; CME, cystoid macular edema; ELM, external limiting membrane; ERM, epiretinal membrane; ILM, inner limiting membrane; INL, inner nuclear layer; IRF, intraretinal fluid; OPL, outer plexiform layer; PVD, posterior vitreous detachment; RPE, retinal pigment epithelium; VH, vitreous hemorrhage; VMT, vitreomacular traction.
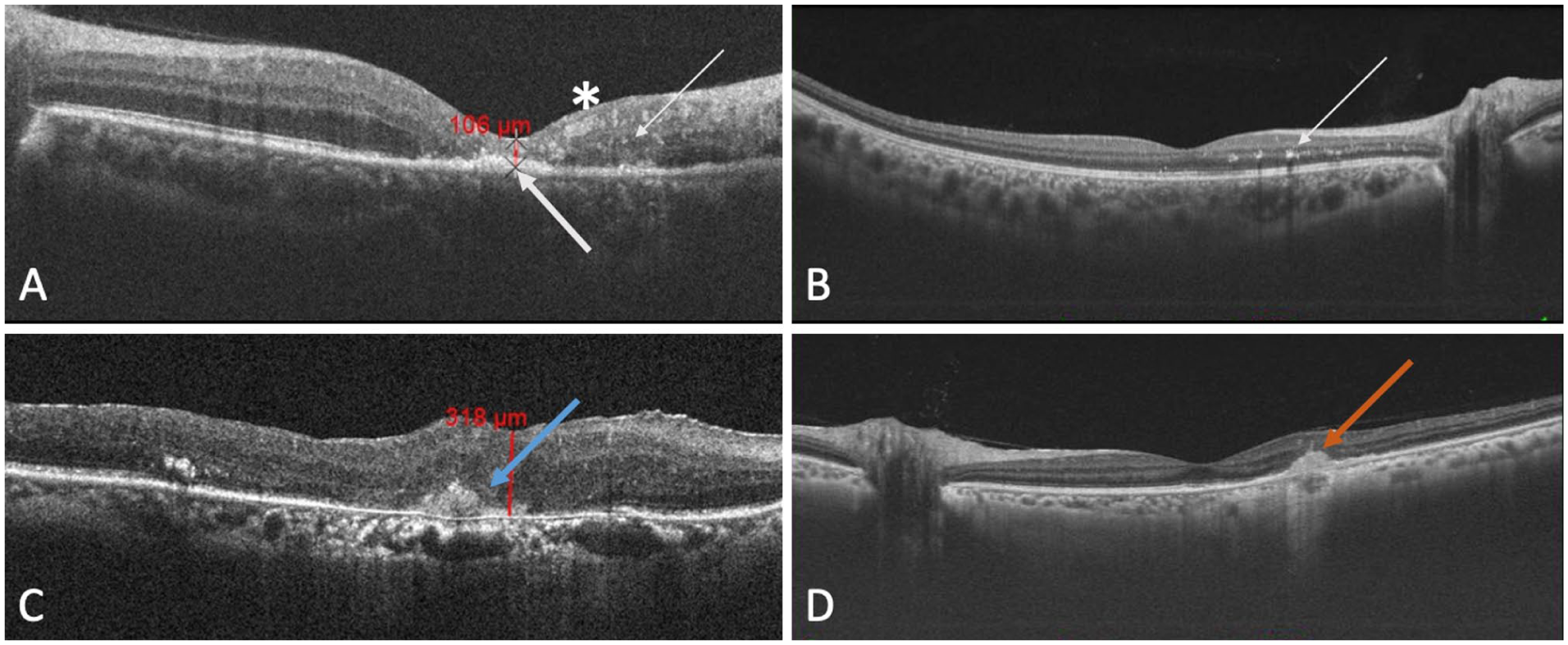
Optical coherence tomography images of leukemic infiltrates. (A) Multiple hyperreflective clumps in the inner nuclear layer (asterisk), outer nuclear layer, and outer plexiform layer (OPL, thin white arrow), and plaque-like subretinal deposition (bold white arrow), with associated loss of subfoveal ellipsoid zone and interdigitation zone. (B) Multiple hyperreflective foci and clumps in the OPL (thin white arrow) temporal to the fovea. (C) Multiple hyperreflective foci diffusely in all retinal layers with clumped deposition above the retinal pigment epithelium (RPE) juxtafoveally (blue arrow) as subretinal leukemic infiltrate. (D) Sub-RPE deposit (orange arrow) with back shadowing.
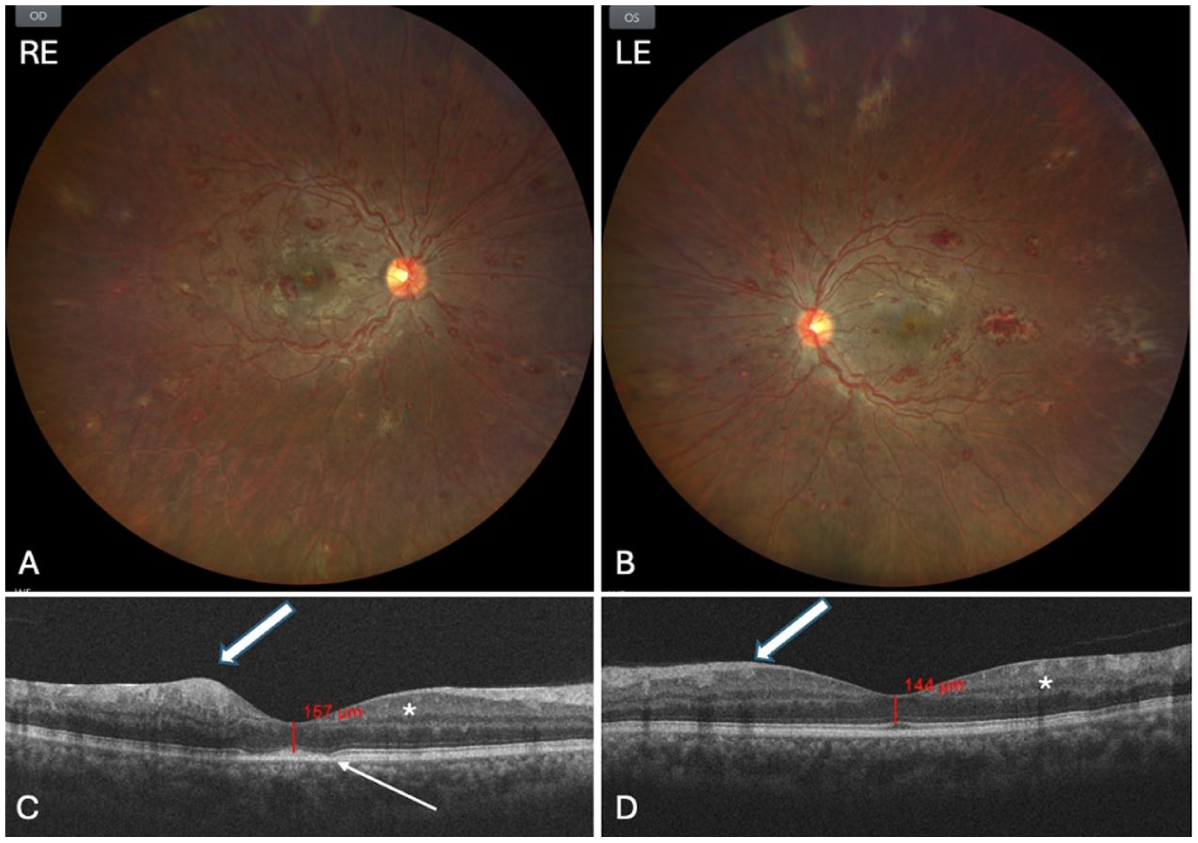
(A, B) Fundus photographs showing bilateral Roth spots and leukemic infiltrates in all quadrants. (C, D) Optical coherence tomography reveals sub-inner limiting membrane hemorrhage (bold white arrow), subfoveal ellipsoid zone disruption (thin white arrow), and clustered leukemic infiltrates in the inner retina (asterisk). The patient was later confirmed to have chronic myeloid leukemia.
All patients underwent laboratory workup, including complete blood profile, peripheral blood smear, cerebrospinal fluid analysis, bone marrow biopsy or aspiration, and radiologic investigation (magnetic resonance imaging or computed tomography, if needed). Immunophenotyping was performed with flow cytometry in all bone marrow samples to differentiate acute myeloid leukemia (AML) from acute lymphocytic leukemia (ALL).
A detailed description of ocular and systemic treatment as treatment naïve, treatment failure, and treatment recurrence was noted for all patients. Treatment-naïve patients were newly diagnosed patients with leukemia with no previous history of systemic therapy. Treatment failure was indicated by lymphoblasts totaling more than 5% in the bone marrow or more than 1% minimal residual disease, assessed no earlier than the end of the induction phase. Recurrence was defined as the reappearance of leukemic cells at any site after remission (confirmed by minimal residual disease and lymphoblasts). Complications associated with chemotherapy or radiation therapy were documented.
Depending on the extent of involvement (retina/choroid/optic nerve), visual loss, and current state at which they presented (treatment naïve/under treatment/remission/relapse), patients were treated locally with antivascular endothelial growth factor (VEGF) injections, laser photocoagulation, and vitreoretinal surgery, or were kept under observation under the guidance of a treating hematoncologist. All patients kept under observation were asked to follow up in 3 months to look for any reversal of clinical findings and improvement in hematologic parameters.
Statistical Analysis
Data were recorded and compiled into a Excel spreadsheet (Microsoft). The data were summarized using descriptive statistics. Categorical variables were expressed as frequencies and percentages, whereas continuous variables were expressed as mean ± SD or median (interquartile range). For categorical variables, Pearson χ2 test was used when expected cell count were adequate. Fisher exact test was applied when expected cell counts were low. In analyses with very small subgroup sizes, statistical testing was not performed, and results are presented descriptively as percentage to avoid overinterpretation. Univariate and multivariate regression analyses were performed to identify OCT factors associated with disease relapse or poor visual outcome in patients. A model selection procedure was used to reduce model complexity, and the parameters chosen were based on their clinical relevance and importance. P < .05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 16, IBM, SPSS Inc.).
Results
Demographics
A total of 77 eyes of 47 patients were analyzed. The mean age was 41.75 ± 21.75 years, ranging from 7 to 76 years (Table 2). Of the 47 patients, 39 (83%) were men and 8 (17%) were women. Unilateral presentation was observed in 23 patients (29.8%) and bilateral presentation in 54 (70.1%). Of the 77 eyes, 37 (48%) were right, and 40 (51.9%) were left. The average follow-up period was 13.43 ± 21.98 months (range, 4.93-83.8 months).
Demographic Profile of Patients Diagnosed With Leukemia.
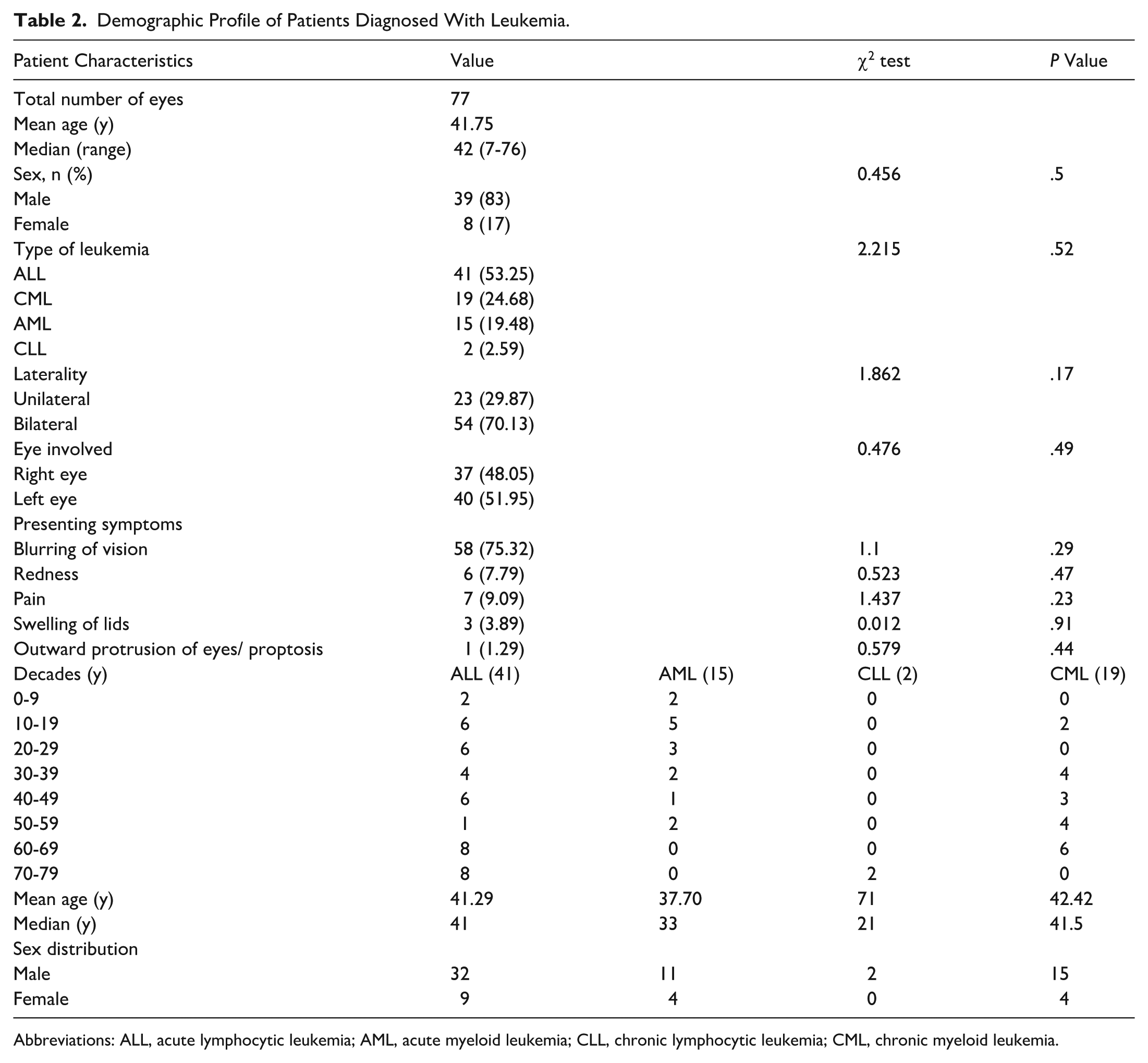
Abbreviations: ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia.
In our study, ALL was the most common type of leukemia, in 41 eyes (53.25%), followed by CML in 19 eyes (24.68%), AML in 15 eyes (19.48%), and CLL in 2 eyes (2.59%). The most common ocular complaint was blurring of vision in 58 eyes (75.32%), followed by pain in 7 eyes (9.09%), redness in 6 eyes (7.79%), swelling of lids in 3 eyes (3.89%), and proptosis in 1 eye (1.29%). No statistical significance was found with respect to BCVA.
OCT Findings
The OCT findings (Table 1) are divided into 3 broad categories: Vitreoretinal interface, leukemic infiltrates, and macula.
Vitreoretinal Interface
Posterior vitreous detachment (PVD) was defined as complete separation of the posterior hyaloid from the macular surface on OCT irrespective of attachment at the optic nerve head. PVD was the most common finding at the vitreoretinal interface (16 eyes [20.8%]) and was most often seen in patients with CML (7 eyes [36.8%]), followed by patients with ALL (6 eyes [14.6%]). Other findings included vitreous hemorrhage (VH) (5 eyes [6.5%]), subhyaloid hemorrhage (6 eyes [7.8%]), epiretinal membrane (ERM) (1 eye [1.3%]), and vitreomacular traction (VMT) (2 eyes [2.6%]). Changes in the vitreoretinal interface were not statistically significant with respect to BCVA, probably due to the small sample size and heterogeneity in hemorrhage characteristics.
Leukemic Infiltrates
Of 77 eyes, 30 patients (39%) had leukemic infiltrates visible on OCT. Approximately 57.9% of patients with CML had leukemic infiltrates at the posterior pole (n = 11), followed by 36.6% of patients with ALL (n = 15) and 26.6% of patients with AML (n = 4). No patients with CLL had infiltrates. Leukemic infiltrates were independent of sex, laterality, and leukemia type. Leukemic infiltrates were statistically significant in all layers (P < .01) except the subretinal pigment epithelium (sub-RPE) layer. Infiltrates were most often observed in the inner retinal layers from the inner limiting membrane to the inner nuclear layer (ILM-INL) (n = 21 [70%]), with 10 eyes in patients with CML (52.6%), 9 in patients with ALL (21.9%), and 2 in patients with AML (13.3%). This was followed by the outer retinal layers from the outer plexiform layer to the external limiting membrane (OPL-ELM) (n = 18 [60%]), with 7 eyes in patients with CML (36.8%), 9 eyes in patients with ALL (21.9%), and 2 eyes in patients with AML (13.3%). Leukemic infiltrates in the subretinal space were observed in 6 eyes (20%), 3 eyes in patients with ALL (7.3%), 2 in patients with CML (10.5%), and 1 eye in a patient with AML (6.7%). Patients with subretinal infiltrate tended to have worse BCVA, but the difference was not statistically significant. Only 1 patient with ALL (3.3%) had sub-RPE infiltrate. A mixed pattern was present in 6 eyes (40%), with 5 eyes (12.2%) in patients with ALL and 1 eye (6.7%) in a patient with AML. The location of the leukemic infiltrate had no significant effect on BCVA.
Most leukemic infiltrates were small/dots (n = 21 [70%]), with 13 (31.71%) found in patients with ALL, 6 (31.6%) in patients with CML, and 2 (13.3%) in patients with AML. Larger size infiltrates or clumps were seen in 12 eyes (40%), with 6 eyes (31.6%) in patients with CML, 5 eyes (12.2%) in patients with ALL, and 1 eye (6.7%) in a patient with AML. Plaque-like accumulation of leukemic infiltrates was observed in 4 eyes (13.3%), with 2 eyes (4.8%) in patients with ALL, 1 eye (5.2%) in a patient with CML, and 1 eye (4.8%) in a patient with AML. A mixed pattern was observed in 7 eyes (23.3%), with 5 eyes (12.2%) in patients with ALL, and 2 (10.5%) in patients with CML. The size of the leukemic infiltrate was not significantly different between patients’ BCVA.
Of 30 eyes with leukemic infiltrates, 10 eyes (33.3%) had back shadowing, with 5 eyes (12.2%) in patients with ALL, 3 eyes (20%) in patients with AML, and 2 eyes (10.5%) in patients with CML. This was not statistically significant for BCVA.
Macular Findings
Of the 77 total eyes, foveal thinning was present in 37 eyes (48%), with 17 eyes (41.5%) in patients with ALL, 10 eyes (52.6%) in patients with CML, 9 eyes (60%) in patients with AML, and 1 eye (50%) in a patient with CLL. A sub-ILM bleed was observed in 6 eyes (7.8%), with 3 eyes (15.8%) in patients with CML, 2 eyes (4.9%) in patients with ALL, and 1 eye (6.7%) in a patient with AML. An intraretinal bleed was observed in 10 eyes (13%), with 6 eyes (14.63%) in patients with ALL and 4 eyes (21%) in patients with CML. Cystoid macular edema (CME), defined as the presence of well demarcated cystoid hyporeflective spaces within the retinal layers, typically the inner nuclear layer or outer plexiform layer, was seen in 13 eyes (16.9%), with 7 eyes (36.8%) in patients with CML, 5 eyes (12.2%) in patients with ALL, and 1 eye (50%) in a patient with CLL. CME was significantly associated with worse BCVA (χ2, 5.56) (P = .01).
Neurosensory detachment was present in 4 eyes (5.1%), 2 eyes (4.9%) in patients with ALL, 1 eye (5.26%) in a patient with CML, and 1 eye (50%) in a patient with CLL. Intraretinal fluid (IRF), defined as diffuse, noncystoid spaces or spongy edema within the retinal layers, was observed in 18 eyes (23.4%), with 10 eyes (24.3%) in patients with ALL and 8 eyes (42.1%) in patients with CML. Macular hole was observed in 5 eyes (6.5%), with 2 eyes (4.9%) in patients with AML, 2 eyes (10.5%) in patients with CML, and 1 eye (6.7%) in a patient with AML. Scars were observed in 11 eyes (14.3%), with 8 eyes (19.5%) in patients with ALL, 2 eyes (10.53%) in patients with CML, and 1 eye (50%) in a patient with CLL. RPE thickening was observed in 2 eyes (2.6%), both in patients with ALL.
Ellipsoid zone (EZ) loss was observed in 18 eyes (23.38%), of which 10 (24.4%), 6 (31.6%), 1 (6.67%), and 1 eye (50%) belonged to patients with ALL, CML, AML, and CLL, respectively. Loss of EZ was significantly associated with worse BCVA (χ2, 6.27, P = .013). Choroidal thickening (defined as a subjective increase in thickness of the choroid with dilated Haller layer) was seen in 4 eyes (5.2%), all of which were in patients with ALL. In addition to CME and EZ loss, other OCT findings were not statistically significant with respect to BCVA (Figure 3). The treatment-naïve patients had significantly more sub-ILM (χ2, 10.77, P < .01) and intraretinal bleeding (χ2, 13.4, P < .01). Patients with treatment failure frequently presented with neurosensory detachment (χ2, 6, P = .01) and IRF (χ2, 10.66, P < .01). Patients with recurrence most often presented with intraretinal bleeding (P = .01).

Optical coherence tomography of a patient with chronic myeloid leukemia in blast crisis. (A, B) Foveal scans show cystoid macular edema (bold white arrow), loss of the ellipsoid zone (thin white arrow), and multifocal leukemic infiltrates in the inner and outer retina.
Univariate regression analysis was used to analyze various factors associated with disease outcome (Table 3), revealing a significant relationship between the presence of CME (odds ratio [OR], 0.114; 95% CI, 0.014-0.932; P = .04) and EZ loss (OR, 3.8821; 95% CI, 1.289-11.692; P = .01) with visual outcome. This relationship was further validated using multivariate regression analysis by adjusting for other variables, confirming CME (OR, 0.022; 95% CI, 0.008-0.687; P = .02) and EZ loss (OR, 5.598; 95% CI, 1.571-19.943; P < .01) were associated with poor visual outcome.
Cox Predictive Regression Model to Determine OCT Risk Factors Predictive of Disease Remission in Patients With Leukemic Ophthalmopathy.
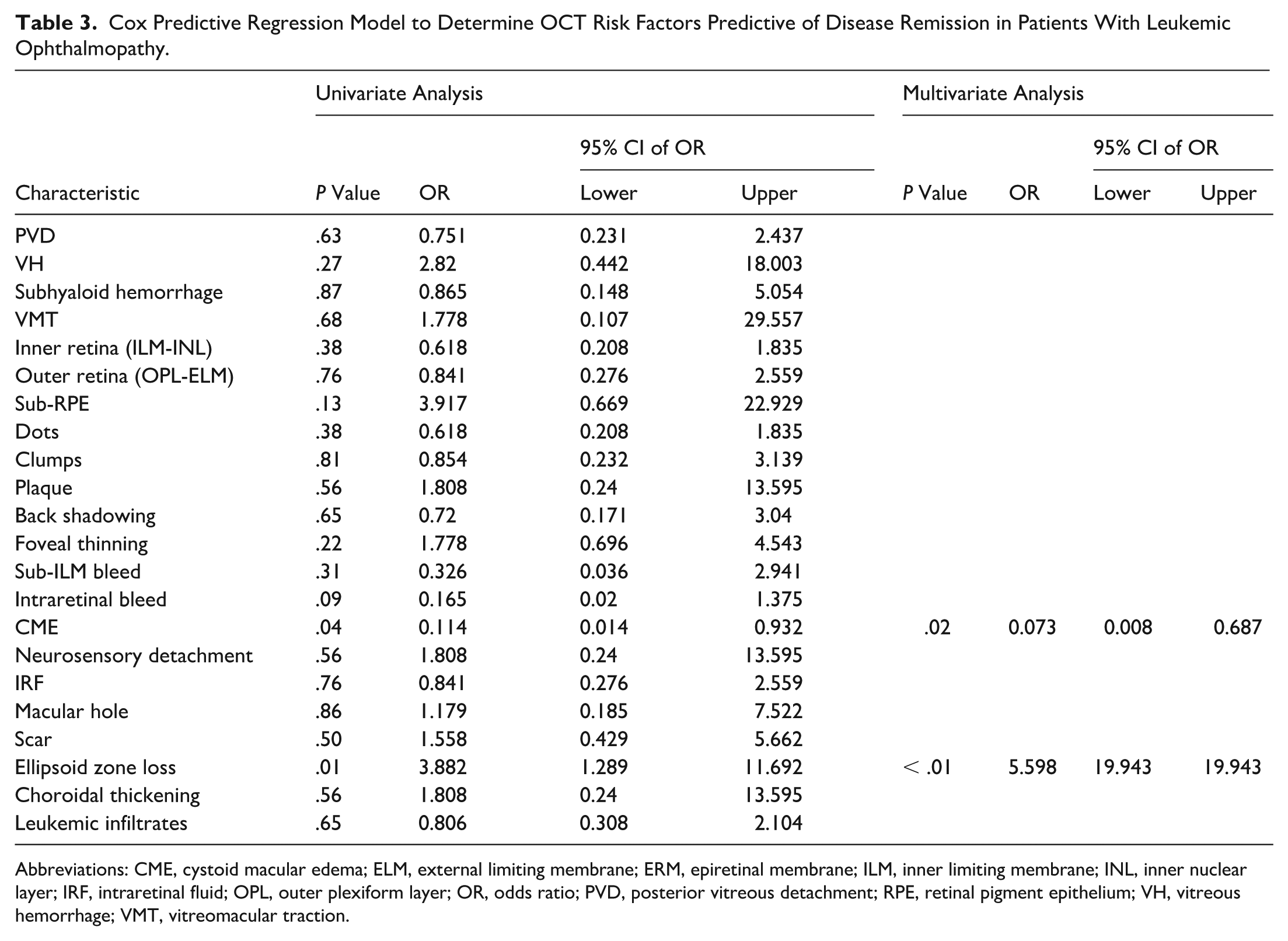
Abbreviations: CME, cystoid macular edema; ELM, external limiting membrane; ERM, epiretinal membrane; ILM, inner limiting membrane; INL, inner nuclear layer; IRF, intraretinal fluid; OPL, outer plexiform layer; OR, odds ratio; PVD, posterior vitreous detachment; RPE, retinal pigment epithelium; VH, vitreous hemorrhage; VMT, vitreomacular traction.
Management
Of the 77 eyes included in the present study, 29 (37.7%) were treatment naïve, with 14 eyes (34.1%) in patients with ALL, 9 eyes (60%) in patients with AML, and 6 eyes (31.6%) in patients with CML. Nine eyes (11.7%) experienced treatment failure, with 5 eyes (12.2%) in patients with ALL, 2 eyes (10.53%) in patients with CML, and 2 eyes (13.3%) in patients with AML. Recurrences occurred in 25 eyes (32.5%), with 14 eyes (34.1%) in patients with ALL, 8 eyes (42.1%) in patients with CML, and 3 eyes (20%) in patients with AML (Table 4). Data regarding the treatment status of patients with CLL could not be retrieved. Treatment status was not statistically significant with BCVA or leukemic infiltrates.
Comparison of Treatment Status and Ocular and Systemic Management in Different Forms of Leukemia and Their Correlation With Visual Acuity.
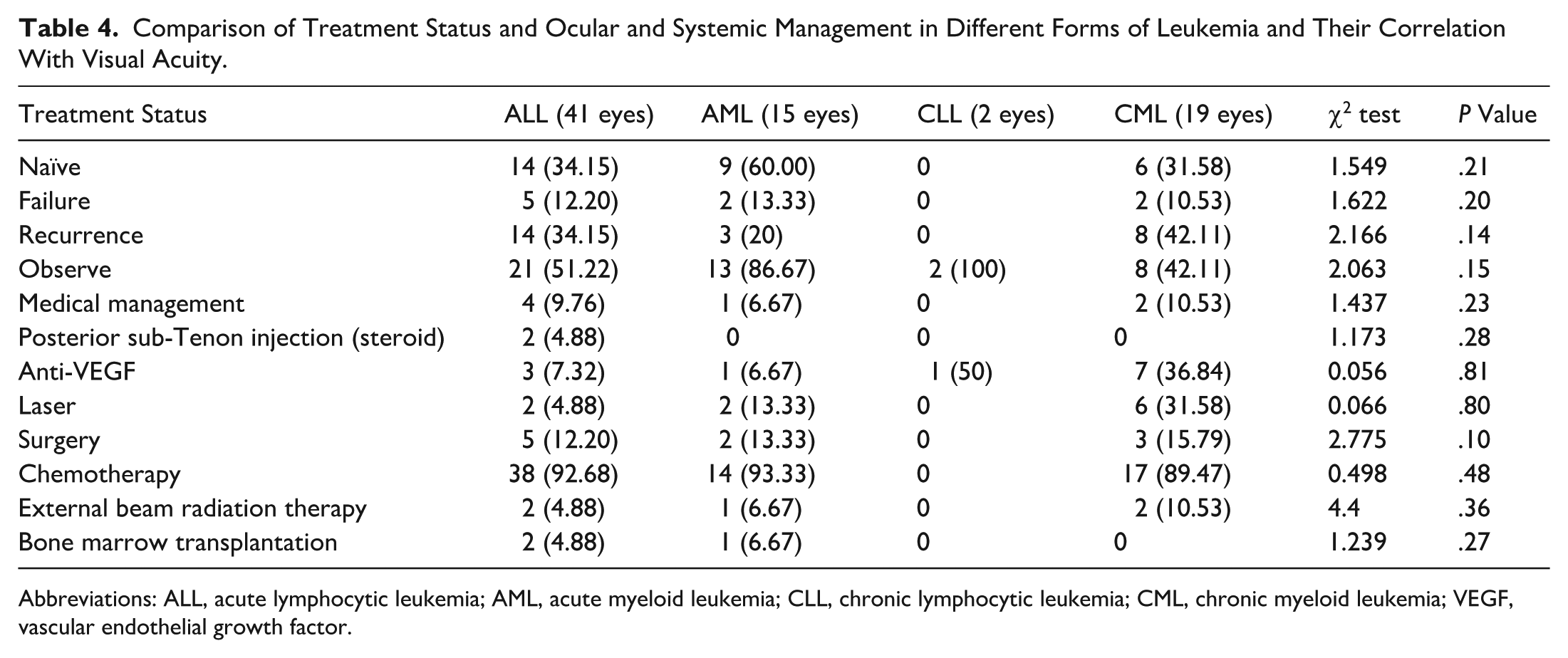
Abbreviations: ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; VEGF, vascular endothelial growth factor.
If we inspect the systemic treatment, 69 of 77 eyes (89.61%) were receiving chemotherapy. Although the details of the chemotherapy are outside the scope of this study, chemotherapy was administered to 38 eyes (92.7%) in patients with ALL, 17 eyes (89.5%) in patients with CML, and 14 eyes (93.3%) in patients with AML. Five eyes (6.5%) underwent external beam radiotherapy, with 2 eyes (10.5%) in patients with CML, 2 eyes (4.9%) in patients with ALL, and 1 eye (6.7%) in a patient with AML. Three eyes belonged to patients who underwent bone marrow transplantation, with 2 eyes (4.9%) in patients with ALL and 1 eye (6.7%) in a patient with AML. Patients with treatment failure underwent external beam radiotherapy. No significant difference was observed between chemotherapy and bone marrow transplantation.
Regarding ocular treatment, 44 eyes (57.1%) were kept under observation, with 21 eyes (51.2%) in patients with ALL, 13 eyes (86.7%) in patients with AML, 8 eyes (42.1%) in patients with CML, and 2 eyes (100%) in patients with CLL. Seven eyes (9%) were managed medically with topical steroids, cycloplegics, or nonsteroidal anti-inflammatory drugs, with 4 eyes (9.8%) in patients with ALL, 2 eyes (10.5%) in patients with CML, and 1 eye (6.7%) in a patient with AML. Only 2 eyes (2.6%) needed posterior sub-Tenon steroid injection for CME, both in patients with ALL (4.9%). Twelve eyes (15.5%) with bleeds, leukemic infiltrates, CME, neurosensory detachment, or IRF required anti-VEGF injection, such as bevacizumab 1.25 mg/0.05 mL, ranibizumab 0.5 mg/0.05 mL, aflibercept 2 mg/0.05 mL, or triamcinolone acetonide 2 mg/0.05 mL. Of these 12 eyes, 7 (36.9%) were in patients with CML, 3 (7.3%) in patients with ALL, and 1 eye (50%) in a patient with CLL. Laser photocoagulation was required in 10 eyes (13%), with 6 eyes (31.6%) in patients with CML, 2 eyes (4.9%) in patients with ALL, and 2 eyes (13.3%) in patients with AML. Ten eyes (13%) underwent surgical procedures, including pars plana vitrectomy for nonresolving or persistent VH or subhyaloid hemorrhage, 5 eyes (12.2%) in patients with ALL, 3 eyes (15.8%) in patients with CML, and 2 eyes (13.3%) in patients with AML. Treatment-naïve patients and those experiencing recurrences were most often kept under observation (P < .01) or required intravitreal anti-VEGF injection (P < .01) or surgical intervention (P < .01). Neither ocular nor systemic treatment was statistically significant for BCVA and leukemic infiltrates.
Conclusions
Approximately 70% of the cases in the present study demonstrated bilateral involvement with asymmetrical presentation, reflecting the systemic nature of the disease. Leukemic infiltrates were most often present in the inner retinal layers, whereas the RPE was intact regardless of the leukemia subtype. However, CLL could not be studied because of the small sample size. The involvement of the outer retinal layers and sub-RPE was coexistent with that of the inner retinal layer. Direct infiltration from choroidal vessels is often attributed to leukemic infiltrates, but the superficial retinal capillary plexus plays a more pertinent role in circulating the infiltrates. This was also suggested by Yee et al, who documented the presence of hyperreflective lesions in inner retinal layers with no disruption of RPE or Bruch membrane, indicating a more likely involvement of inner retinal vasculature.4,21 Previous literature shows outer retinal layer involvement can also occur in the absence of choroidal involvement, and they can independently coincide with inner retinal hyperreflectivity, corresponding with intraretinal hemorrhages. 11
Eventually, these infiltrates may either resolve with systemic control or form clumps that invade deeper layers; in severe cases, plaques with back shadowing ultimately lead to EZ loss. Many case reports have shown that these inner retinal layer infiltrates resolve without atrophy of the inner retinal layers.4,22 On the other hand, there are reports that suggest the resolution pattern of large outer retinal leukemic infiltrates is associated with atrophy in the RPE-Bruch complex.11,23-26 In either case, a poorer prognosis was found in eyes with foveal involvement. 11 The proposed mechanism of subsequent atrophy is impedance of intraretinal microvasculature due to a space-occupying lesion effect or direct invasion of leukemic cells, causing retinal ischemia locally and subsequent retinal atrophy. 11 The impedance of the capillary plexus was supported by various studies through increased vascular density of the superficial and deep capillary plexus.10,27 The subsequent retinal ischemia has also shown changes on foveal avascular zone circularity on OCT angiography. 10
CME, which is a more frequent manifestation in CML cases, is reportedly secondary to tyrosine kinase inhibitor (TKI) use and typically responds well to their cessation and intravitreal anti-VEGF or steroids. 28 In our study, CME and the EZ were 2 important OCT biomarkers that correlated with poorer visual prognosis. In the literature, the loss of the outer retinal layer and EZ has been suggested to be an important cause of poor visual prognosis. 11
Notably, 13% of leukemic retinal infiltrates presented with back shadowing regardless of the location, pattern, or size. The absence of back shadowing has been reported as a factor that differentiates between leukemic infiltrates and typical retinal vasculature. 21 We saw that although back shadowing is a notable feature, it is not pathognomic in terms of definite differentiation. Interestingly, the location of retinal infiltrates did not influence visual acuity, unless associated with CME or EZ loss. The infiltrates appeared as dots, clumps, or plaques; however, their size did not affect the visual prognosis in the univariate or multivariate analysis. All plaque-like leukemic retinal infiltrates involved the outer retinal layers extending from the OPL to the sub-RPE region, supporting the hypothesis that multiple dots in inner retinal layers coalesce into clumps and eventually evolve into plaque through vertical progression. However, only 1 such case was associated with EZ loss, indicating that not all infiltrates are associated with poor visual prognosis.
Few hemorrhagic manifestations, such as VH, intraretinal bleed, and sub-ILM bleed, showed a trend toward poorer visual prognosis, but no statistical significance was achieved. No patient presented with choroidal neovascularization. An additional observation was that treatment-naïve and recurrent patients usually presented with hemorrhagic manifestations, such as sub-ILM or intraretinal bleeding, often necessitating anti-VEGF therapy or vitreoretinal surgery.29–31 In contrast, patients with treatment failure predominantly exhibited neurosensory detachment and CME. A longitudinal study would be instrumental in elucidating the pathophysiologic basis of these distinct patterns of presentation.
Although ours is the first study to describe the OCT features of leukemic infiltrates and its visual prognosis, this retrospective cross-sectional study has limitations that cannot be ignored. The unequal distribution of leukemia subtypes and the heterogeneous nature of the patient population can also introduce bias and skewness in the data. Hematologic parameters were not studied in association with OCT due to nonavailability. We could not analyze patients with CLL because of the small sample size and lack of information about treatment status. The selection of variables for multivariate analysis was based on a univariate P value threshold of < .1 which, while commonly used, may introduce selection bias and potentially overlook clinically relevant confounders. The heterogenous duration of follow-up rather than standardized time-specific end points may influence visual outcome and limits longitudinal visual prognosis. Future prospective studies with serial OCT imaging and hematologic correlation are warranted to validate our findings.
Although a wide variety of leukemic infiltrates were studied, the visual prognosis was affected by secondary structural changes at the macula, such as CME and EZ loss, regardless of the leukemia type and the location, size, or pattern of retinal infiltrates. CME and EZ loss emerged as important OCT prognostic markers in leukemic retinopathy. This can help stratify visual risk and monitor treatment response.
Footnotes
Ethical Considerations
This study was approved by the institutional review board at L V Prasad Eye Institute (Ethics Ref No. LEC-BHR-R-03-24-456).
Consent to Participate
Informed consent was obtained from all the parents or guardians of each subject after a thorough explanation of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an unrestricted departmental grant from Hyderabad Eye Research Foundation, Hyderabad, India. The funders had no role in the preparation, review, or approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.