
Abstract
Purpose:
To evaluate the potential retinal toxicity associated with ritonavir, a protease inhibitor widely used to treat HIV.
Methods:
This study comprised a literature review of PubMed and EMBASE for all published cases of ritonavir-associated retinal toxicity as well as a retrospective chart review of patients treated with ritonavir who underwent bilateral retinal macular and ultra-widefield imaging at an urban tertiary care medical center. Retinal images were evaluated for morphologies consistent with previously reported cases of ritonavir toxicity.
Results:
The literature review identified 16 cases of retinal toxicity potentially linked to ritonavir, 7 (44%) of which reported liver dysfunction. A chart review of 483 patients taking ritonavir with bilateral retinal imaging demonstrated no cases of ritonavir toxicity, consistent with the literature.
Conclusions:
Fewer than half of the published cases of ritonavir retinal toxicity had liver dysfunction, suggesting a possible dissociation between the liver and retinal toxicities. Based on the absence of retinal toxicity in our institution’s cohort, this study proposes that ritonavir retinal toxicity is far less common than previously considered, there may be a genetic predisposition to ritonavir toxicity, and previous reports may be cases of misdiagnosed hereditary maculopathies.
Introduction
Since the 1996 approval of ritonavir, 1 a protease inhibitor and antiretroviral medication for the treatment of HIV, there have been numerous reported cases connecting its use to retinal toxicity. 2 Ritonavir is primarily metabolized in the liver via the P450 isozyme system, and liver dysfunction has been associated with ritonavir toxicity through increased plasma concentration levels of the drug. 3 Inhibition of 2 crucial cytochrome metabolic pathways, CYP3A and 2D6, may lead to increased levels of ritonavir in patients with underlying liver conditions.3,4 This increased drug concentration is a proposed mechanism of retinal toxicity.2,5 A potential pathophysiology was observed in animal models, in which rodents treated with ritonavir showed hypertrophy of the retinal pigment epithelium (RPE) and retinal degeneration, with ultrastructural studies suggesting damage to the retina, liver, thyroid, and kidney secondary to phospholipidosis, with amorphous granular inclusion bodies in the liver and the retina. 6
Although there are reported cases of ritonavir-associated retinal toxicity, no study has investigated the prevalence of retinal toxicities in a patient population. Given the reported progressive, relentless, and usually permanent nature of ritonavir-associated retinopathies and their somewhat diverse phenotypic presentations, early recognition of toxicity is paramount.
This study seeks to evaluate ritonavir’s potential retinal toxicities through a combined approach that includes a thorough evaluation of existing literature related to ritonavir toxicity and an assessment of the prevalence and associated risk factors of ritonavir retinal toxicities in a large academic medical center patient population. Our aim is to better elucidate the prevalence of ritonavir retinal toxicity, describe potential risk factors for toxicity, and report on the breadth of possible presenting phenotypes.
Methods
A literature search was performed with PubMed, Cochrane Library, and Ovid using the terms ‘ritonavir’, ‘maculopathy’, ‘retinopathy’, and ‘toxicity’ to retrieve all available articles on the subject of ritonavir retinal toxicity. Inclusion criteria were articles reporting at least 1 case of retinal toxicity in humans and articles containing retinal imaging for comparison. Non-English publications and duplicate articles or cases were excluded from the study.
A retrospective, descriptive chart review was then performed of patients with current or previous ritonavir use seen in the Weill Cornell Medical Center Department of Ophthalmology from January 2010 to June 2023. Approval by the Weill Cornell Medicine Institutional Review Board was obtained for the review of clinical images and electronic health records (EHR; Epic). Informed consent was waived because this study posed minimal risk to patients, and all study research activities adhered to the tenets of the Declaration of Helsinki. Chart review was completed in November 2023, with statistical analysis occurring in November 2024.
The New York Presbyterian/Weill Cornell Medical Center patient database was queried for patients with the following inclusion criteria as defined by their EHR: 1) previously received or currently receiving highly active antiretroviral therapy (HAART) containing ritonavir (alone or in combination with another drug) for any duration; and 2) bilateral retinal imaging (Optos ultra-widefield, Optos PLC) or optical coherence tomography (OCT) available and interpretable after therapy initiation. All imaging reviewed was obtained in providing routine clinical care and with standard clinical practice protocols for Weill Cornell. The first order date for ritonavir was considered the drug initiation date. The drug stop date was considered the earlier of the 2 dates between the imaging date and the last date ritonavir was listed as ordered in the EHR.
Where available, patient information was recorded, including age, sex, age at the start of treatment, treatment duration, daily dose, and cumulative dose. Descriptive statistics were performed on the analyzed cohort using GraphPad Prism 9. Three reviewers (J.K., L.G., K.K.), one of whom is a board-certified vitreoretinal surgeon (K.K.), evaluated retinal images for evidence of toxicity and compared them with the identified case studies of ritonavir-induced retinopathy in the literature. Images were explicitly reviewed for features of outer retinal attenuation (ellipsoid and retinal pigment epithelial loss), and alternative etiologies for these features were also recorded via review of multimodal retinal imaging and the patient’s clinical history. Exclusion criteria were insufficient retinal imaging, retinal detachment with extensive laser treatment, active exudation from central serous chorioretinopathy or age-related macular degeneration, and extensive retinal scarring or schisis that precluded reliable image interpretation. Cumulative doses were compared between patients without any retinal findings and those with any degree of outer retinal changes to determine whether there was a dose-dependent relationship for these features.
Results
Literature Review
The literature search produced 12 articles with a total of 16 cases of ritonavir-associated retinopathy from 2011 to 2024 (Supplement 1).2,5,7–16
In total, there were 14 men and 1 woman reported to have ritonavir retinal toxicity, while 1 case study did not report the patient’s sex. Patients’ ages ranged from 30 to 68 years. The shortest reported duration on ritonavir with observed toxicity was 19 months after the start of treatment, while the longest duration was 224 months after the start of treatment. Cumulative ritonavir dose ranged from 40 to 504 g. The presence of liver dysfunction was reported in 7 of 16 cases and was absent in 7 of 16. Two of 16 articles did not report the status of the patient’s liver function. Eleven cases had information on follow-up after cessation of ritonavir. Seven of 11 cases reported worsening of the patient’s retinopathy, while 3 cases reported stabilization of the retinopathy, and 1 reported improvement.
Of the current published case studies, both the shortest duration of ritonavir treatment (19 months) and the longest duration (396 months) were reported to have extensive maculopathy that worsened even after the cessation of ritonavir treatment. The case with the lowest cumulative dose had extensive bilateral maculopathy that worsened even after ritonavir cessation, while the case with the highest cumulative dose demonstrated a mild, unilateral hyperemic lesion of the fovea that improved within 2 weeks of ritonavir cessation.2,5
There was a heterogeneity in the phenotypes of ritonavir-induced retinopathy described in the literature. RPE and outer retinal atrophy or thinning were explicitly described in most (14/16) reports. Other phenotype characteristics were more variable and included a bull’s eye maculopathy pattern (4/16), parafoveal telangiectasis (2/16), intraretinal crystalline deposits (4/16), and midperipheral bone spicules (1/16). All but 1 case reported bilateral involvement. 5 All but 1 patient was male (15/16). None of the cases had genetic testing included in their report.
Retrospective Descriptive Chart Review
A total of 496 patients on ritonavir were identified with either form of retinal imaging; 467 of 496 patients had OCT images (Heidelberg or Zeiss), and 329 (329/496) patients had ultra-widefield retinal imaging. The final analysis included 483 patients (Table 1). Patients were prescribed ritonavir as part of treatment for HIV or hepatitis C. Although ritonavir has been used as part of a combination drug regimen for COVID-19 treatment (ie, nirmatrelvir/ritonavir [Paxlovid]), 15 the chart review did not identify patients with ritonavir prescriptions for this drug. Complete ritonavir prescription history was available for 471 of 483 reviewed patients. The average age at ritonavir initiation was 46 years (SD, 11; range, 4–75 years), while the average age at imaging was 58 years (SD, 11; range, 15–87 years). The sex distribution was 30.8% female (149/483) and 69.2% male (334/483).
Ritonavir Chart Review of 483 Patients.
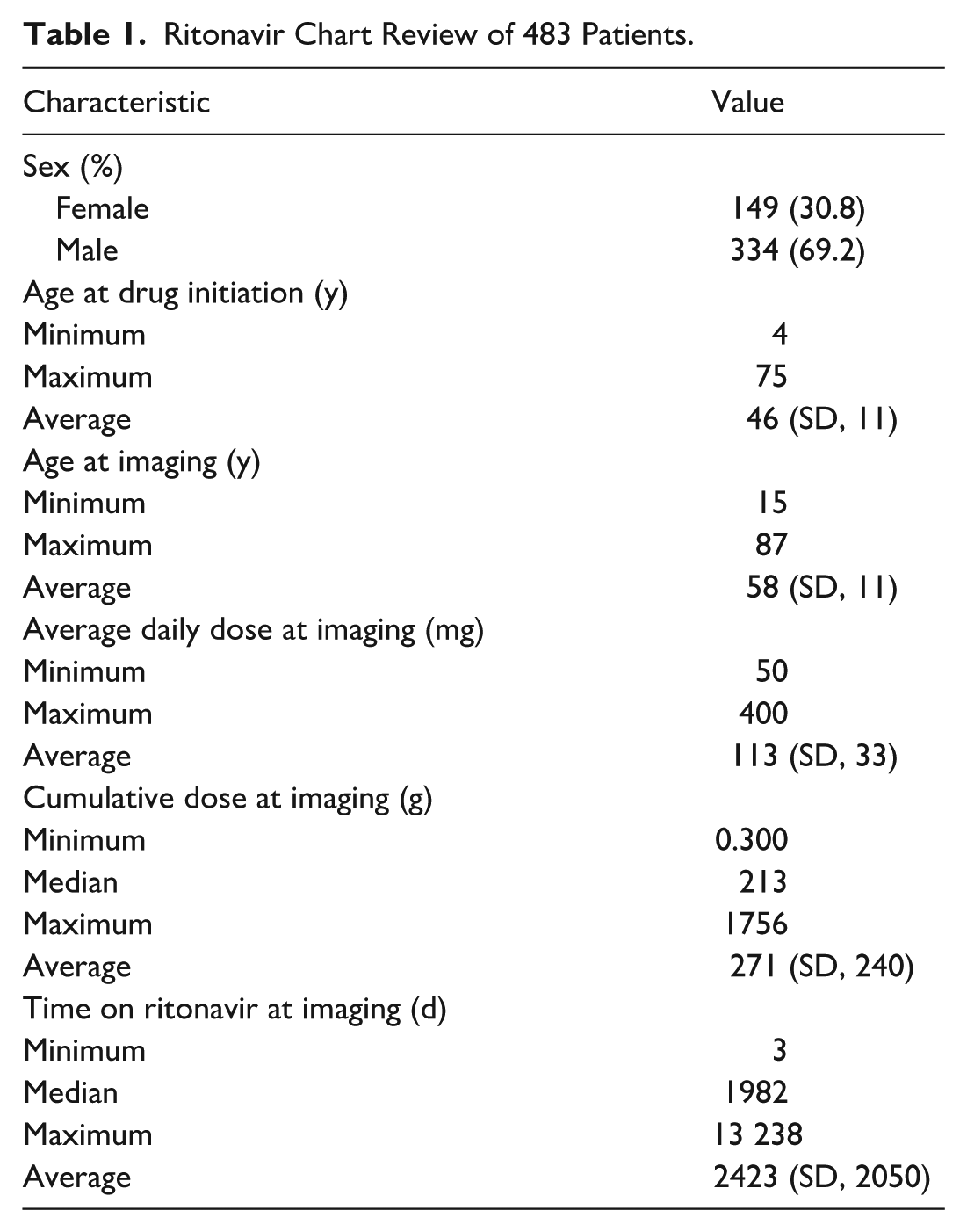
Of the other drugs patients had been prescribed as part of an antiviral regimen before imaging, the 5 most common were tenofovir (433 patients), maraviroc (399), emtricitabine (384), dolutegravir (235), and darunavir (218). The earliest drug start date was in 1996 and the latest was in 2020. The overall average daily dose was 113 mg (SD, 32; range, 50–400 mg), and the overall average cumulative dose at imaging was 271 g (SD, 240; range, 0.300–1756 g; median, 213). At the time of imaging, patients had received ritonavir treatment for an average of 2423 days (SD, 1980; range, 3–13 238 days). There was no significant difference in the cumulative dose for the 38 patients with outer retinal changes and 433 patients without outer retinal changes (average, 287 g with vs 269 g without; P = .66). The most recent CD4+ cell count before imaging was available for 221 patients (median, 265; range, 8–1511); the most recent aspartate aminotransferase was available for 477 patients (median, 26; range, 9–388 U/L); and the most recent alanine aminotrasferase was available for 477 patients (median, 25; range 9–221 U/L).
After all available images of each patient were reviewed, patients were identified with the following retinal diseases: CMV retinitis (11), diabetic retinopathy (14), hypertensive retinopathy (8), and HIV retinopathy (4) (Table 2). However, bilateral maculopathy or bilateral outer retinal degeneration that resembled any of the published case reports of ritonavir-induced retinal toxicities were not observed. This includes those characterized by either bilateral retinal pigment epitheliopathy, bull’s eye maculopathy, parafoveal telangiectasis, intraretinal crystalline deposits, or retinitis pigmentosa mimics. 17
Distribution of Patients and Eyes With EZ and RPE Abnormalities Attributable to Non–Ritonavir-Related Retinal Diseases in the Cohort.
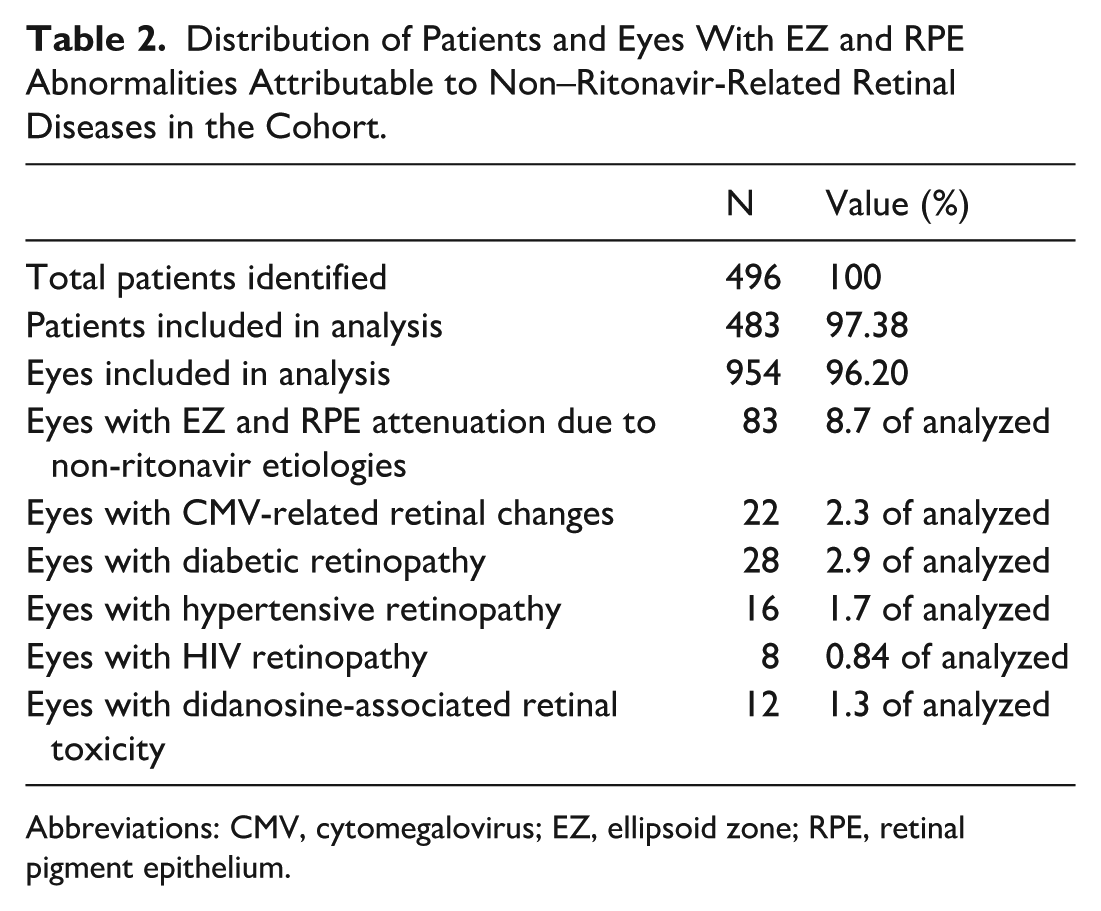
Abbreviations: CMV, cytomegalovirus; EZ, ellipsoid zone; RPE, retinal pigment epithelium.
Conclusions
Ritonavir is a protease inhibitor commonly used in treatment for HIV and hepatitis C. 18 The first observation of retinal changes after treatment with ritonavir was reported by Roe et al in 2011, 2 and today there are 16 reported cases of presumed ritonavir-induced retinopathy.2,14 RPE atrophy and outer retinopathy are recurrent findings in these patients. In addition, other changes, such as bull’s eye maculopathy, parafoveal telangiectasis, intraretinal crystalline deposits, and retinitis pigmentosa mimics, have been reported.2,17 Most cases demonstrated a worsening of retinopathy despite cessation of ritonavir. One patient, however, had improvement after cessation. Nevertheless, this was in the setting of a positive Rapid Plasma Reagin and Fluorescent Treponemal Antibody Absorption, and it is very possible that their retinal pathology was caused by syphilis rather than ritonavir. 5 In the review of published cases, half the patients had liver dysfunction, and nearly all were men. As previously mentioned, no reported cases included genetic testing. One report described the retinal findings as “retinitis pigmentosa-like.” 16 It also remains to be elucidated if there are possible genetic contributions that promote sensitivity to ritonavir retinal toxicity, which cannot be adequately assessed without genetic testing.
Currently, the most proposed mechanism of ritonavir retinopathy involves liver dysfunction via P450 inhibition, which leads to increased drug plasma levels.2,3,11 However, of the 16 cases reported, only 14 included the status of the liver; of these, only 7 cases reported any form of liver dysfunction, while 7 patients had normal liver function (Table 1). Although serum drug levels were not measured, this suggests that half the cases of ritonavir retinopathies with reported liver status are less likely fully explained via the proposed pathophysiology. Other studies have demonstrated that ritonavir can inhibit vascular endothelial growth factor (VEGF) and hypoxia-inducible factor 1α in vitro, which may contribute to the pathophysiology responsible for ritonavir-induced retinopathy. 19 However, to date, there have been no follow-up human trials that reveal evidence of vision loss or retinal toxicity through this mechanism. 6
In the institutional investigation of 483 patients’ retinal images, no images were found corresponding to retinopathy as previously described in the current literature. This population was reasonably representative, in both age and sex, of the demographics reported with ritonavir retinal toxicity in the literature. We also compared the demographics of our ophthalmology clinic imaging cohort (n = 483) with the total ritonavir-using population at our institution (n = 32 650). The institutional cohort had a mean age of 62 years and was 57.5% female, whereas the ophthalmology-imaged subset had a mean age at imaging of 58 years and was 31.5% female. Thus, while age distributions were broadly similar, our clinic-based sample included proportionally fewer women than the overall ritonavir population. These differences may reflect referral and utilization patterns specific to ophthalmology. The average patient was also on a ritonavir drug for sufficient time (1982 days) and with sufficient cumulative dose (271 g) to plausibly induce retinal toxicity. This may suggest that ritonavir-associated retinopathy has a lower prevalence than anticipated and therefore requires a greater sample size to measure its prevalence more accurately. However, it is also possible that the existing reports on ritonavir-induced retinopathies may be a result of an etiology different from the suspected ritonavir treatment (eg, a genetic retinal disorder).
Of note, didanosine is another antiretroviral drug that has been linked with retinopathy. To date, there have been at least 24 reported cases of didanosine-related retinopathy with characteristic bilateral peripheral retinal pigmentary changes with macular sparing.14,20 In a separate retrospective study conducted to investigate the prevalence of didanosine retinopathy, multiple instances of suspected didanosine-induced retinal toxicities were identified with consistency and specificity using these key characteristics from previous case reports. 21 Furthermore, while no in vitro or in vivo experiments have been performed to test for didanosine-induced retinopathy, the suggested pathophysiology has more evidence for biological plausibility proposed by previous studies, which have demonstrated that didanosine can cause mitochondrial toxicity.22–24 This was proposed to cause damage to denser populations of rods in outer segments with higher metabolic demand, while sparing the macula.14,22 For these reasons, there is better-established basic science and clinical evidence for didanosine retinopathy than ritonavir retinopathy. Although ritonavir retinal toxicity is considered uncommon, it is important to consider the context of its use in recent drug advancements, such as in COVID-19 treatment. We suggest that ritonavir, as a direct cause of retinal disease, could be eliminated from consideration in the absence of future studies confirming causal association.
Although this paper yielded negative results, it is an important step in challenging current beliefs about ritonavir toxicity. This should prompt reevaluation for ritonavir’s use in clinical practice, especially within the context of its use in more recent drugs, such as for the treatment of COVID-19. This study proposes that previous reports of ritonavir maculopathy may represent misdiagnosed alternative etiologies. It is also possible that there may be a genetic component predisposing patients to ritonavir toxicity or to ritonavir toxicity in the setting of liver dysfunction, but again this cannot be proven in the absence of genetic testing. These are just some possible explanations and should be a priority for future research.
This study was retrospective, which limited its impact. The query to identify patients with history of ritonavir was limited to patients who had documented previous or current ritonavir use in the medication section of the EHR. If a patient received ritonavir treatment in the past but it was not recorded in the EHR system, that could not be identified by the query. It is also possible that the inclusion of combination drugs could affect the toxicity risk. However, it does not seem likely that this would greatly influence results because ritonavir is primarily used in combination therapies. Similarly, the reliability of initiation date and, therefore, calculated time duration of treatment at time of imaging, cannot be entirely guaranteed based on potential variability in how the drug was recorded in the patient’s EHR. Further, this was not a randomized control study as it had a sampling bias toward patients in an ophthalmology department of an academic institution. It is also possible that this study was underpowered to detect ritonavir toxicity, although this would speak to the rarity of the entity if not found at all in this cohort. Finally, we excluded non-English publications in the literature review, which may have resulted in missing data on ritonavir toxicity. There is evidence, however, that this decision may not ultimately have altered our conclusions. 25 To our knowledge, this is the first study investigating the prevalence of ritonavir toxicity. If the causal relationship between ritonavir and ritonavir-induced retinopathy is to be strengthened, a follow-up study with a larger cohort would be required to more powerfully measure the prevalence of ritonavir retinal toxicity.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264261463163 – Supplemental material for Literature Review and Institutional Imaging Analysis of Ritonavir Retinal Toxicity
Supplemental material, sj-docx-1-vrd-10.1177_24741264261463163 for Literature Review and Institutional Imaging Analysis of Ritonavir Retinal Toxicity by Carla G. Dias, Tobin B.T. Thuma, Lili Gerendas, Joshua Seokju Kim, Jaffer Shah, M. Abdallah Mahrous, Donald J. D’Amico, Mahmood Khan, Szilard Kiss and Kyle D. Kovacs in Journal of VitreoRetinal Diseases
Footnotes
Ethical Considerations
This project received ethical approval from the Weill Cornell Institutional Review Board (IRB) under IRB #22-07025078.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received funding through an NYEE Foundation Grant.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kovacs previously consulted for Intergalactic Therapeutics and Regenxbio Inc. Dr. Kiss holds intellectual property associated with ocular gene therapy and cellular therapy and has provided consultancy services to Adverum, Gyroscope Therapeutics, Regenxbio Inc., and Spark Therapeutics. Apart from these disclosures, the authors have no other relevant affiliations or financial involvements with any organizations or entities having a financial interest or conflict regarding the subject matter or materials discussed in the manuscript.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.